
To the Editor:
Posterior ocular segment involvement in systemic sclerosis (SSc) is rare. To the best of our knowledge, the retinal vascular occlusion presenting at onset of SSc has never been reported in the literature. We describe 3 cases of patients with retinal thrombosis without apparent risks of ocular disease, followed by fully SSc typical manifestations. Of note, all 3 patients fulfilled the new 2013 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for the diagnosis of SSc at onset, while the previous 1980 ACR criteria were satisfied long after.
In SSc, the most frequent ocular manifestations involve anterior segment, such as eyelid skin fibrosis and keratoconjunctivitis sicca. Posterior segment involvement is less common, and findings similar to those observed in arterial hypertensive retinopathy, such as cotton wool spot, optical disc edema, and hemorrhages, have been reported1,2. Nevertheless, abnormal ocular findings are frequently detected by fluorescein angiography (FA), and posterior segment microvessel damage and pigment epithelium layer atrophy are shown in up to 50% of patients with SSc3. However, eye disease always occurred in established SSc and it has never been described at onset.
The first case was a 42-year-old woman with Raynaud phenomenon (RP) lasting 26 years, and with recent transient episodes of right eye scotoma and progressive visual loss. FA showed temporal retinal vein occlusion, optic disc edema, and hard cotton wool spots. Blood pressure was 100/65 mmHg. She had anticentromere antibodies (ACA) 1/160. The nailfold videocapillaroscopy (NVC) showed an “early scleroderma pattern”4 without further signs of systemic disease. One year later, esophageal scintigraphy showed low-middle segment reflux and basal interstitial fibrosis at chest computed tomography (CTC).
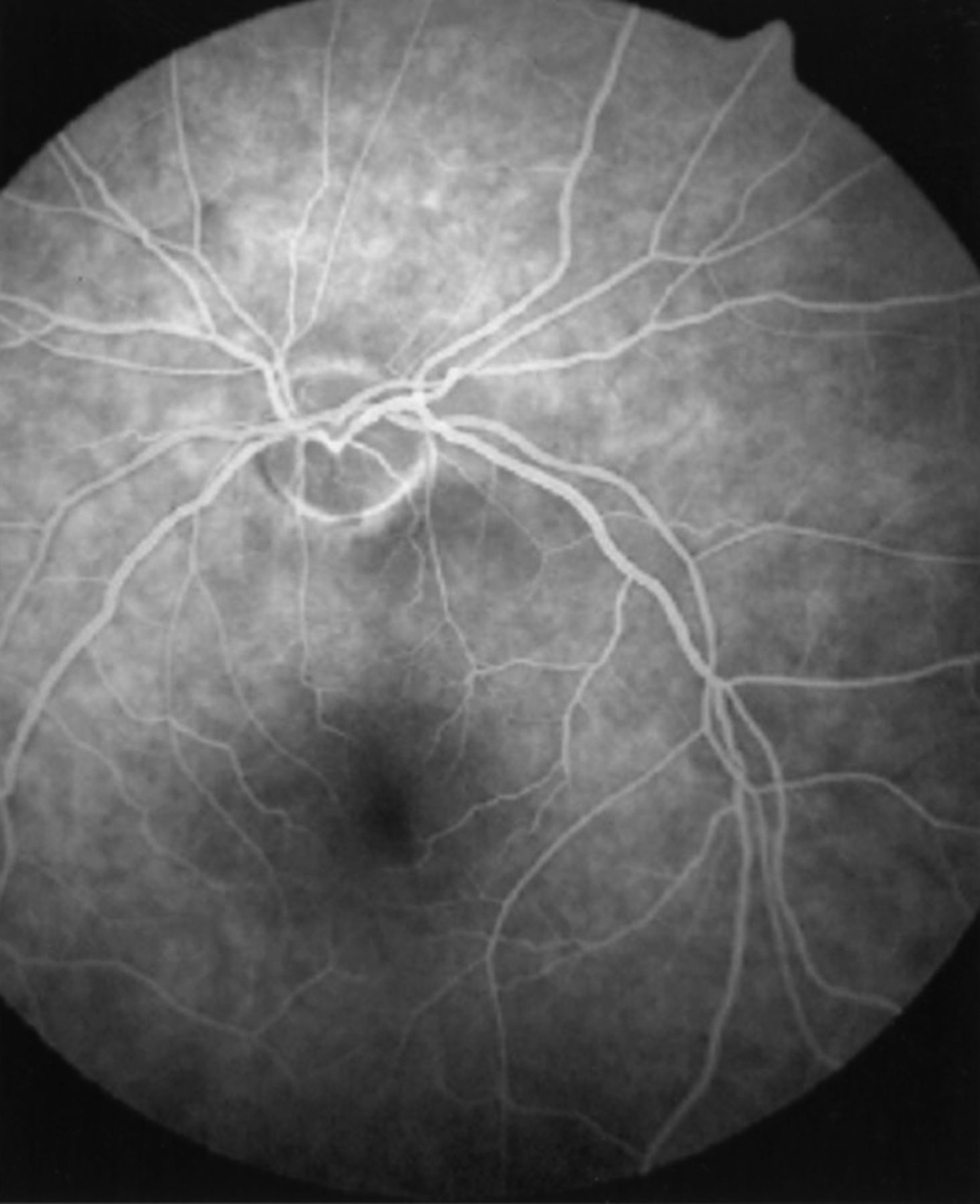
The second patient was a 57-year-old woman with 20 years of RP, sclerodactyly, and a 2-month history of acute visual loss in her left eye. FA showed hemorrhages and cotton wool spots because of central retinal vein occlusion (Figure 1). Blood pressure was 110/75 mmHg. ACA 1/1280 were present and NVC showing an “active scleroderma pattern”4. Esophageal scintigraphy showed low segment reflux. After 5 years, digital ulcers occurred.
{kind=link}
Fluorescein angiography of the left eye showing retinal pallor typical of central artery occlusion.
The third case was a 62-year-old woman with 12 years of RP and a 5-year history of visual disorders with findings of retinal artery ischemia at FA. Blood pressure was 125/80 mmHg. She was affected by fingertip pitting scars with ACA 1/160. Moreover, limited ground glass area of middle lobe at CTC and “active scleroderma pattern” at NVC were found. One year later, sclerodactyly and digital ulcers occurred. No patient had acquired or inherited activated protein C resistance, protein S deficiency, factor V Leiden mutation, antiphospholipid antibodies, hyperhomocysteinemia, or high D-dimers.
Eye involvement has never been described as an onset symptom of SSc. Here, we reported 3 cases of SSc in which retinal vessel occlusion occurred early and before the diagnosis of SSc was made. Retinal vein or artery occlusions have been previously described in late SSc2. Fibroproliferative vasculopathy may affect retinal vessels, and 3 cases of acute unilateral blindness because of arterial occlusion have been reported in established SSc5. To the best of our knowledge, for the first time, here we report 3 cases of retinal vessel occlusion in early SSc. In all cases, long-lasting RP, NVC changes, and ACA were detected. ACA are commonly reported in association with organic vasculopathy in SSc6,7. Further, the frequency of ACA was higher in patients with SSc who had retinal abnormalities than in those without8. Two patients also had vein and 1 arterial retinal thrombosis. It could be supposed that vasoactive molecules, such as endothelin-1, may be shed from artery to retinal veins because of their tight proximity7, thereby accounting for vein occlusion in our patients.
In all 3 patients, the retinal vessels occlusion occurred after RP and before the diagnosis of SSc was made according to the 1980 ACR classification criteria9. In reviewing these cases, after the new SSc ACR/EULAR 2013 classification criteria were issued10, we noted that in all patients the SSc diagnosis could have been made within a few months after the eye involvement. On this basis, they could be classified as definite SSc according to the 2013 ACR/EULAR criteria, whereas none of them satisfied the old 1980 ACR criteria (Table 1).
Comparison between the ACR 1980 classification criteria and the ACR/EULAR 2013 criteria in the 3 patients at the onset of retinal vessels occlusion.
Retinal vessels involvement has been described in established late SSc. Our report provides evidence that retinal vessel occlusion may be the first symptom occurring after RP in SSc. In these patients, despite suspected connective tissue disease, SSc diagnosis was made long after. All 3 case were SSc from the onset, but could not be classified according to the 1980 ACR criteria. The introduction of the new classification criteria may aid in identifying SSc in earlier stages, and as in our cases, linking rare clinical manifestations to the disease. In patients with acute vision abnormalities and retinal vessels occlusion, SSc should be taken into consideration and clinicians ought to proceed with adequate diagnostic investigations.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.