
Abstract
Objective. We introduce the use of 99mTc-hydroxymethylene diphosphonate (HDP) digital blood flow scintigraphy to diagnose Raynaud’s phenomenon (RP).
Methods. Fifty-seven patients with RP and 60 healthy controls were recruited. One hand was chilled by immersion into water at 4°C, and then an intravenous bolus of 740 MBq of 99mTc-HDP was injected. The radioactivity from the second to the fifth fingers of both hands was recorded. Acquisition was performed at a rate of one frame per 2 seconds until 155 frames. We calculated 4 ratios by comparing the activity curves of the chilled hand with those of the ambient hand.
Results. The chilled to ambient hand ratio of the initial slope was significantly lower in the patients with RP (0.28 ± 0.18) than in the controls (0.78 ± 0.20) (p < 0.001). The chilled to ambient hand ratio of the first peak height, 30-second area under the curve, and blood pool uptake were also lower in the patients with RP than in controls (p < 0.001 for each). The initial slope ratio of 0.51, used as a cutoff value, showed a sensitivity of 91.2% and specificity of 93.3%. The loss of the initial spike curve, the presence of a slowly progressing radioactivity curve, and the inhomogeneous radioactivity uptake in the blood pool image in either hand were characteristic findings of the patients with RP (p < 0.001).
Conclusion. 99mTc-HDP digital blood flow scintigraphy after one-hand chilling is a noninvasive, accurate, and quantitative method to evaluate RP.
- RAYNAUD’S PHENOMENON
- DIAGNOSIS
- 99mTc-HDP SCINTIGRAPHY
Raynaud’s phenomenon (RP) is an episodic, reversible, vasospastic, ischemic condition that affects the digits and manifests as a triphasic color response involving blanching, cyanosis, and subsequent rubor on rewarming after exposure to cold1,2. RP is a common condition that was found in 2.2% of women and 1.5% of men in a community study in Framingham, Massachusetts, USA3.
The underlying causes of secondary Raynaud’s syndrome are peripheral arterial disease, connective tissue disease, and paraneoplastic disorders4. In patients with connective tissue disorders, such as systemic sclerosis (SSc), RP is associated with small-vessel occlusive disease that can lead to digital pitting scars, ulceration, or gangrene5. It is essential to diagnose RP early, because it is a presenting manifestation in more than 90% of patients with SSc. The annual change in the diagnosis of primary Raynaud’s disease to secondary Raynaud’s syndrome is 1%–2%4. Early effective treatment of the underlying cause can reduce the functional impairment and tissue damage6.
Until recently, the diagnosis of RP has been based on the patient’s description of the clinical manifestations. Induction of visible RP by chilling the hand in cold water is often not successful in the routine clinical setting. Thus, many studies have been performed to establish an objective technique for the diagnosis of RP, but all these methods have shown some limitations. For example, the finger systolic pressure test requires complex tools, and cannot compare the severity between fingers simultaneously (usually only the middle phalanx)7. Arteriography does not show luminal obstruction in primary Raynaud’s disease8, and the color chart methods are limited with regard to quantitative measurement of RP. When the physician’s observation was the sole means of diagnosing RP, patients whose change in hand color was not witnessed by a physician were considered false-negatives. Laser Doppler blood flow monitoring, thermography, and Doppler ultrasound are used for patient evaluation, but no single method is regarded as diagnostic.
To avoid the disadvantages of all these methods, we developed a noninvasive method to diagnose RP using 99mTc blood flow scintigraphy. We have published a study on RP using 99mTc-methylene diphosphonate (MDP) blood flow scintigraphy9, and several studies have used radioisotopes to evaluate RP10–13. But there was no quantitative study presenting cutoff value with receiver-operating characteristic (ROC) curves and large-scale with more than 100 people enrolled. Additionally, there was no study comparing the chilled to ambient hand ratios in the same individual. In this study, we developed a more accurate and quantitative method using a computer-based picture archiving and communicating system (PACS) and image analysis software.
Most patients with connective tissue disease have musculoskeletal symptoms, and a musculoskeletal imaging method such as bone scintigraphy is helpful for many of them to differentiate the kind of the arthritis and rule out infectious or malignant disease. 99mTc-HDP is one of the most widely used radiopharmaceutical compounds for bone scintigraphy. 99mTc-HDP remains mostly in the blood for the first few minutes after an intravenous bolus injection (initial T1/2 = 1 hour), and then distributes to the tissues afterwards (later T1/2 = 3–4 hours) in proportion to the blood flow14.
Because RP is caused by vascular spasm and structural changes, we assessed the microcirculation of the fingers using digital blood flow scintigraphy for the first 5 minutes after an intravenous 99mTc-HDP bolus injection. We primarily investigated the usefulness of 99mTc-HDP blood perfusion and blood pool scintigraphy after one-hand chilling for diagnosing RP, and the secondary goal was the differentiation between primary Raynaud’s disease and secondary Raynaud’s syndrome. We also assessed the relationship between the scintigraphy measures and the presence of autoantibodies and nailfold capillary changes.
MATERIALS AND METHODS
Patient selection
One hundred seventeen individuals who visited a university hospital from February 2003 to July 2006 were enrolled in this study. The study population included 13 patients with primary Raynaud’s disease and 44 secondary Raynaud’s syndrome and 60 control patients with degenerative noninflammatory musculoskeletal diseases without evidence of vascular disease. Thirteen patients with primary Raynaud’s disease had purely the RP without associated disorder. Forty-four patients with secondary Raynaud’s syndrome included the patients with connective tissue disease such as SSc, systemic lupus erythematosus, and mixed connective tissue disease. The patients with RP had a clinical history of cold-induced intense pallor of the hands followed by cyanosis or rubor on rewarming, which had been observed by a physician. The primary Raynaud’s disease patients fulfilled LeRoy and Medsger’s criteria for primary Raynaud’s disease15. Medications with vasodilatory effects were withheld for more than a week before the scintigraphy. All patients were instructed to avoid cigarette smoking, coffee, and alcohol for 12 hours before the evaluation.
Informed consent was obtained from each patient. The Inha University Hospital ethical committee approved this study.
Nailfold capillaroscopy and serologic studies
Nailfold capillaroscopy was assessed by a rheumatologist blinded to the diagnoses. The fourth finger was observed using a zoom-type wide-field microscope (Meiji EMZ-TR, 12.6–114 times magnification range; Meiji Techno Co. Ltd., Tokyo, Japan) and analyzed using Adobe Photoshop v6.0 software. An avascular area was defined as the absence of 2 or more consecutive distal capillaries, and an ectatic loop was defined as capillaries dilated 4 times or more of the venous diameter compared with that of the adjacent normal microvasculature16. When both the avascular area and ectatic loop were found together in the same patient, they were classified as a scleroderma pattern. The presence of antinuclear antibody (ANA), anticentromere antibody (ACA), antitopoisomerase 1 (anti-topo 1) antibody, antiribonuclear protein (RNP) antibody, cryoglobulin, and antineutrophil cytoplasmic antibody (ANCA) were evaluated.
99mTc-HDP digital blood flow scintigraphy
All patients were rested in a seated position at 22°C for 20 minutes. The patient’s hand showing the more severe symptoms (RP group) or the nondominant hand (control group) was selected for chilling. The hand was chilled for 30 s in cold water at 4°C. The patient then rested for 15 min as a recovery time. Porter, et al measured the digital temperature recovery time after chilling in ice water for 20 s8. The average temperature recovery time was 10 min in the control individuals and 35 min in patients with RP. This vascular spasm reversal time was confirmed in our previous study9. Sarikaya, et al found that perfusion decreased by 7.85% ten minutes after finger chilling in normal individuals, indicating that recovery of normal perfusion after vasoconstriction required more than 10 minutes11. Based on the study of Sarikaya et al, we rested the patients for 15 min; patients were in sitting position with their hands placed closely above the surface of a gamma camera detector (Siemens Orbiter 75; Siemens Corp., Hoffman Estates, IL, USA) equipped with a high-resolution, parallel-hole collimator. Then a bolus of 740 MBq of 99mTc-HDP was injected intravenously at the level of the elbow in the contralateral arm. The acquisition was performed at a rate of 1 frame per 2 s until 155 frames.
The area below the proximal digital crease of the second, third, fourth, and fifth fingers was chosen as the region of interest, and was demarcated by a lead shield ring. We calculated 4 ratios by comparing the activity curves of the chilled hands with those of the ambient hands. The chilled to ambient hand ratios of the initial slope (from the base to the first peak of the radioactivity curve), the height of the first peak of the curve, the initial 30-second area under the curve (AUC), and the blood pool uptake 4 min after injection were calculated using a PACS and image analysis software (M-view version 5.4; Infinitt, Seoul, Republic of Korea). Three scintigraphic characteristics were found: the initial spike curve, a slow progress pattern, and the inhomogeneous radioactivity uptake in the blood pool image on the activity curve. The quantitative variables and the presence of the characteristics on the scintigraphic image were compared between RP patients and the controls. The relationships of these variables with the presence of scleroderma-specific autoantibodies (ACA and anti-topo 1 antibody) and the scleroderma pattern of the nailfold capillaroscopy were assessed.
Statistical analysis
Each value was described using the mean ± SD. Statistical analysis was performed using the SPSS software package for Windows v12.0. The 4 ratios in each group were compared by t test or analysis of variance (ANOVA) with multiple comparisons (Scheffe’s test). ROC curves were used to establish a cutoff value, and to compare the testing ability of the variables to identify RP. The presence of the scintigraphic characteristics was tested using Fisher’s exact test or a chi-square test. The relationships between the scintigraphic variables and the presence of scleroderma-specific autoantibodies and the scleroderma pattern of nailfold capillaroscopy were evaluated using the Mann–Whitney U test. Results were considered significant if the p value was < 0.05.
RESULTS
The patients with primary Raynaud’s disease comprised 9 men and 4 women, whose mean age was 38 ± 13 years. There were 44 patients with secondary Raynaud’s syndrome, 6 men and 38 women, and their mean age was 43 ± 13 years. In the 60 controls there were 25 men and 35 women, of mean age 45 ± 13 years. Demographic characteristics of the patients are summarized in Table 1.
Demographic characteristics of patients.
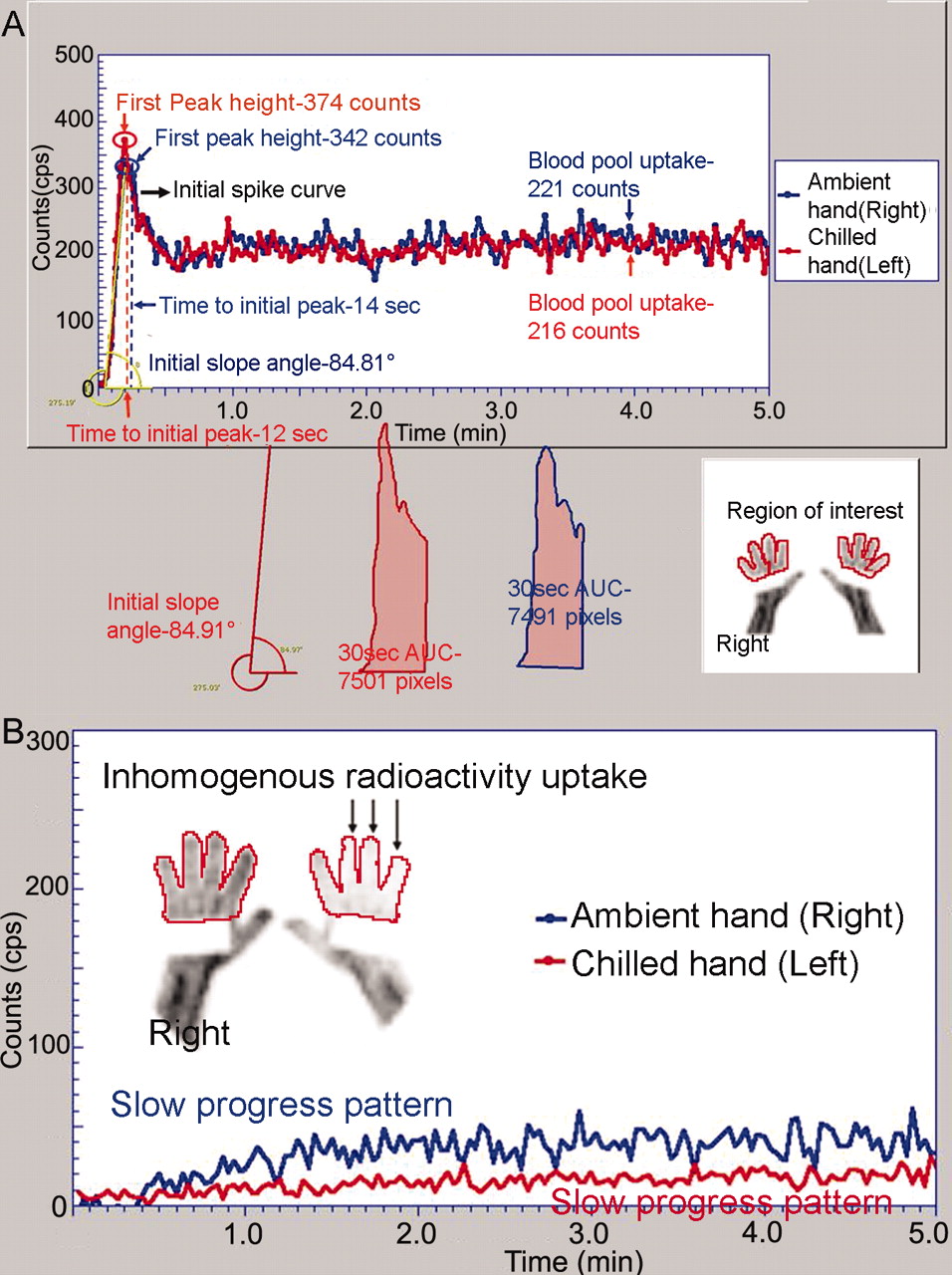
Figure 1 shows the process of the 99mTc-HDP blood flow scintigraphy. There was the initial spike curve in the controls, with nearly the same initial slope, first peak height, 30-second AUC, and blood pool uptake in both hands (Figure 2A). Figure 2B shows the specific slow progress pattern without the initial spike curve in both hands, and the presence of inhomogeneous radioactivity uptake in a patient with RP.

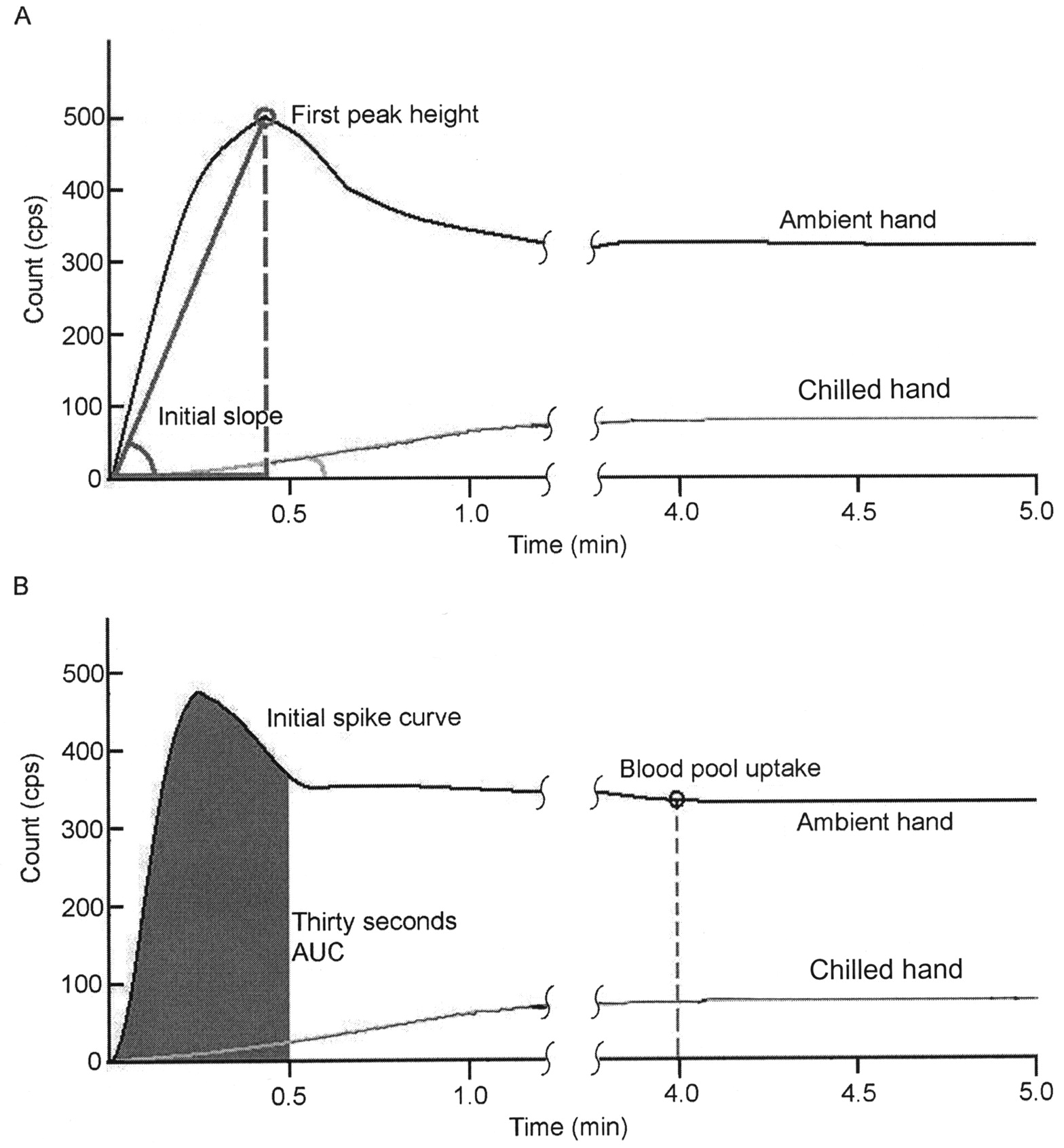
Results of 99mTc-HDP blood flow scintigraphy. A. The initial slope angle and the first peak height. The initial slope of the activity curve was measured from the tangent value of the angle made by the line drawn from the base to the initial peak of the radioactivity curve and the x-axis. B. The 30-second AUC and the blood pool uptake. 30-second AUC was measured from the pixels of a picture archiving and communicating system and image software. Blood pool uptake was the radioactivity measured 4 minutes after injection. We calculated 4 ratios by comparing activity curves of the chilled and ambient hands.
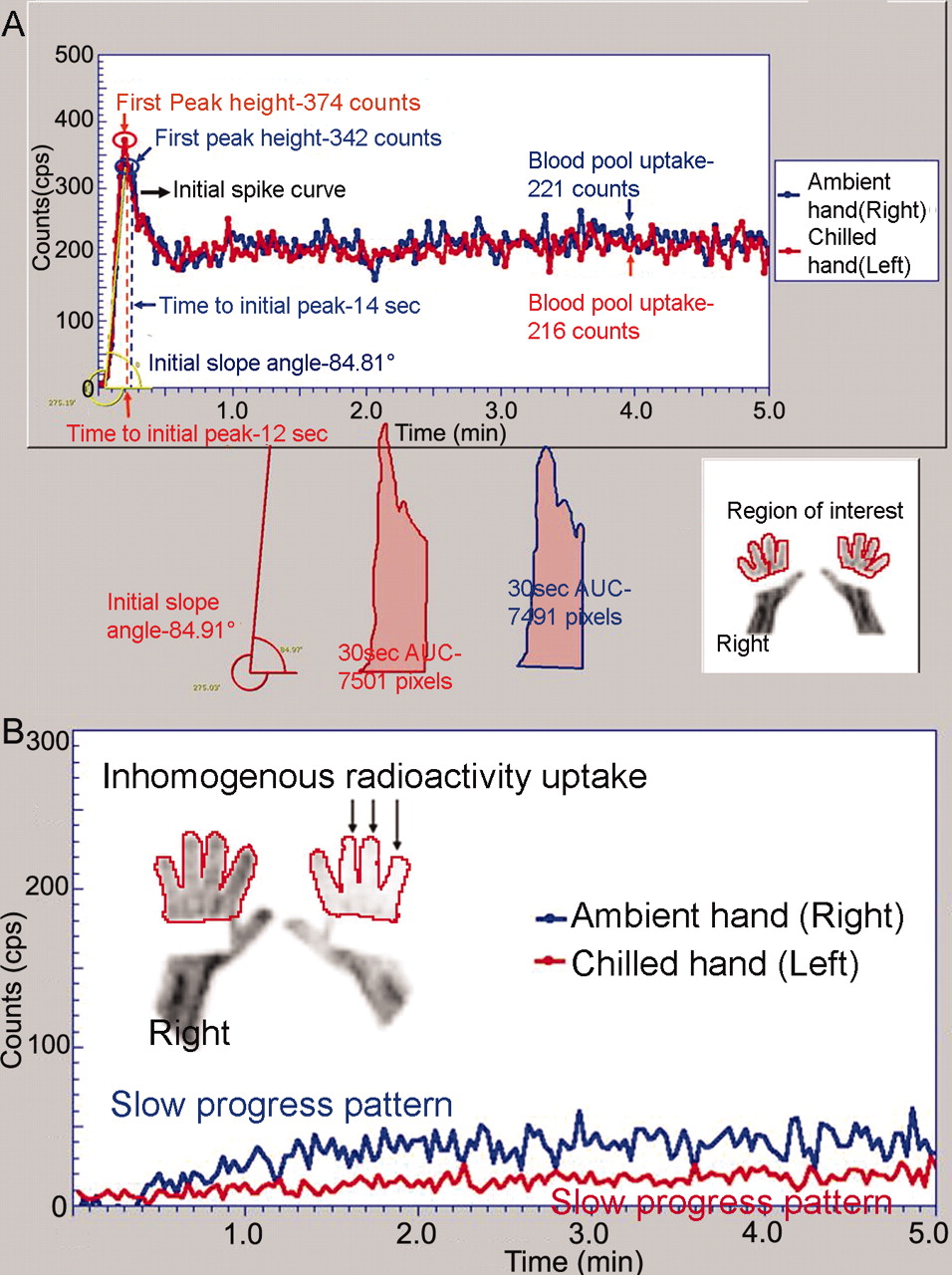
99mTc-HDP blood flow scintigraphy in a control (A) and a patient with Raynaud’s phenomenon (B). The red radioactivity curve represents the chilled hand, the blue curve the ambient hand. A shows the initial spike curve in the controls, with nearly the same initial slope, first peak height, 30-second AUC, and blood pool uptake in both hands. B shows the specific slow progress pattern without the initial spike curve in both hands, and the presence of inhomogeneous radioactivity uptake in the left third to fifth fingers in a patient with Raynaud’s phenomenon.
The 4 quantitative chilled to ambient hand ratios were lower in the RP patients than in the controls, derived from the 99mTc-HDP radioactivity curve (Table 2). The chilled to ambient hand ratio of the initial slope was significantly lower in the patients with RP (0.28 ± 0.18) than controls (0.78 ± 0.20) (p < 0.001). The chilled to ambient hand ratio of the first peak height, 30-second AUC, and blood pool uptake was also lower in the patients with RP than in controls (0.28 ± 0.18 vs 0.79 ± 0.20; 0.35 ± 0.20 vs 0.78 ± 0.19; 0.52 ± 0.18 vs 0.84 ± 0.10; p < 0.001 for each measure). ROC curves were constructed by comparing the sensitivity and specificity of 4 ratios and their accuracy was measured by the AUC-ROC (Table 3). The AUC of the initial slope ratio was the most significant of the 4 ratios (0.968; 95% confidence interval 0.941, 0.995). The AUC of the remaining 3 measures were over 0.93 separately, reflecting the accuracy of the measures in differentiating RP and controls. Figure 3 shows the ROC curve of the 4 ratios. From the ROC curves, we computed the optimal cutoff value, corresponding with the maximum sum of sensitivity and specificity. The optimal cutoff value of the initial slope ratio < 0.51 comes close to maximizing both sensitivity and specificity. With this optimal cutoff value, the sensitivity was 91.2% and the specificity 93.3% for the diagnosis of RP (Table 4). For the remaining ratios — first peak height ratio at threshold < 0.58, the sensitivity was 91.2% and the specificity 86.7%; 30-second AUC ratio at threshold < 0.57, sensitivity 86% and specificity 91.7%; and blood pool uptake ratio at threshold < 0.76, sensitivity 93% and specificity 80% (Table 2).
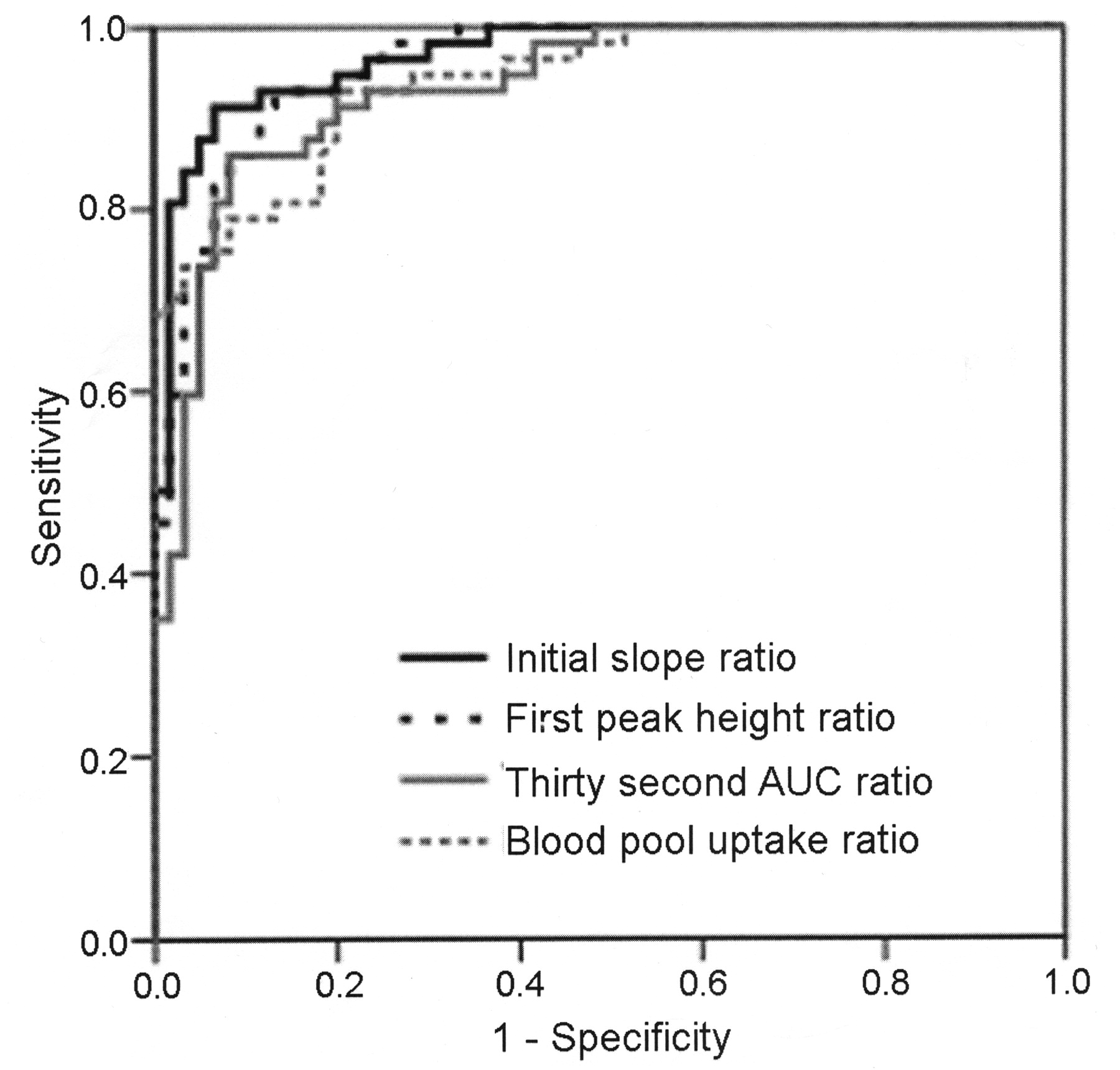
ROC curve of the 4 ratios of chilled to ambient hand.
Comparison of the chilled to ambient hand ratios derived from the 99mTc-HDP radioactivity curve of patients with Raynaud’s phenomenon (RP) and controls. Values are mean ± SD.
AUC-ROC curves of the 4 chilled to ambient hand ratios derived from the 99mTc-HDP radioactivity curve of patients with Raynaud’s phenomenon and controls.
Sensitivity and specificity of the initial slope ratio derived from the 99mTc-HDP radioactivity curve of patients with Raynaud’s phenomenon and controls.
The 4 quantitative ratios did not differ significantly between patients with primary Raynaud’s disease and secondary Raynaud’s syndrome.
Table 5 shows that the loss of the initial spike curve, the presence of the slow progress pattern of the radioactivity curve, and the inhomogeneous radioactivity uptake in the blood pool hand image were characteristic findings in the scintigraphy of the patients with RP (p < 0.001). These findings could be seen most frequently in the chilled hand, then in the ambient hand of the patients with RP, in the chilled hand of the control patients, and least frequently in the ambient hand of the control patients. These characteristic findings did not differ significantly between patients with primary Raynaud’s disease and secondary Raynaud’s syndrome.
Comparison of the presence of the 3 characteristics of 99mTc-HDP blood flow scintigraphy in the chilled and ambient hands of patients with Raynaud’s phenomenon (RP) and controls. Values are expressed as number of patients or controls (%).
There were 5 patients with SSc who underwent followup scintigraphy after treatment. The RP was improved in 3 patients, aggravated in one, and unchanged in one patient. Figure 4 shows an example of an improvement in 5 patients with SSc; Figure 4A represents pretreatment and Figure 4B posttreatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Followup 99mTc-HDP blood flow scintigraphy in a patient with SSc, who presented with severe symptoms of Raynaud’s phenomenon (RP), and showed the slow progression curve pattern specific for RP in the chilled hand (A). The symptoms improved greatly after 2 years of treatment, and at that time the initial spike curve appeared in the chilled hand, with a pattern similar to that observed in normal individuals (B).
None of the 4 chilled to ambient hand ratios of the scintigraphy was significantly related to the nailfold capillaroscopy scleroderma pattern or the presence of scleroderma-specific antibodies.
DISCUSSION
We evaluated the use of 99mTc-HDP digital blood flow scintigraphy after one-hand chilling to diagnose RP. Several studies have used radioisotopes to evaluate RP, including 99mTc-pertechnetate10, 99mTc-sestamibi11, and 99mTc-diethylenetriaminepentaacetic acid (DTPA) human serum albumin12,13. Sarikaya, et al asserted that only 99mTc-sestamibi was a perfusion radiopharmaceutical that could be used to study ischemia at the cellular level11. 99mTc-HDP is absorbed mostly into the bony surface 3–4 hours after intravenous injection, but initially it enters the circulation and can reveal changes in the microcirculation within the first few minutes after administration14. 99mTc-sestamibi is more expensive than 99mTc-HDP. In addition, Sarikaya, et al investigated only the percentage decrease in perfusion for 60 minutes after one-hand chilling. We tested several variables to quantify the effects of the bolus radioisotope injection, the amount of 30-second blood flow, reversibility of arteriolar spasm, and the venous blood pool after 4 minutes.
The morphologic characteristics of scintigraphy (initial spike curve, slow progress pattern, and the inhomogeneous radioactivity uptake) in our study could be a reflection of the RP. Based on the study of Porter, et al8, the average vascular spasm recovery time was 10 minutes in the control individuals and 35 minutes in patients with RP. So 15 minutes after chilling, the vascular spasm in the chilled hand would have recovered in controls, but not in patients with RP. After the recovery of vascular spasm, the isotopes would circulate freely in the blood vessels without being scattered for the first few minutes, then they would be scattered and distributed to the tissues. So the radioactivity curve within the ROI would increase quickly in the first few minutes after injection, and could result in the initial spike pattern. But during the prerecovery vasospasm, the isotopes would have difficulty in circulating in the vessels; then the radioactivity curve would increase slowly, and reveal the slow-progress pattern. In some regions with severe vasoconstriction, few isotopes would pass, and an inhomogeneous radioactivity curve would appear in the scintigraphy. This hypothesis could explain the order of the characteristic scintigraphic findings among the chilled and ambient hands of the RP and control subjects in Table 5. For example, the slow-progress pattern could be seen most frequently in the chilled hand then in the ambient hand of the patients with RP, then in the chilled hand of the controls, and least frequently in the ambient hand of the controls.
Beacham, et al proposed that a conditioning thermal environment should be neither vasoconstrictive nor vasodilatory, and that a temperature range of 22°C–24°C is appropriate17. Porter, et al rested patients at 24°C ± 1°C for 30 minutes8, and Sarikaya, et al did so at 22°C–25°C for more than 15 minutes before cold exposure11. We used constant conditions to ensure that the scintigraphy reflected either clinical improvement or aggravation of RP.
Csiki, et al semiquantitatively analyzed cumulative radioisotope-uptake images 3 minutes after intravenous injection of 99mTc-DTPA18. Their method included radioisotope uptake in the arterioles and capillaries, which are important in RP, in the veins, and even in the perivascular tissues. They did not obtain musculoskeletal images.
There are some limitations in our study. The number of patients with primary Raynaud’s disease was relatively small compared to other groups. Suter, et al reported that RP was a common condition, found in 2.2% of women and 1.5% of men in a community study3, but in our study, the sex ratio (female/male) of patients with RP was much higher (0.74/0.26). We enrolled subjects who presented to the university hospital, so we could not overcome the selection bias of data of the university hospital. We did not evaluate disease severity measures such as visual activity scores or digital scarring, or the treatment response of RP. We wanted to distinguish between primary and secondary RP with this scintigraphy as a secondary objective, but we could not achieve this goal.
Our study, to our knowledge, is the first quantitative study presenting cutoff values, ROC curves, and characteristic scintigraphic morphology (the initial spike and slow-progress pattern) and on a large scale, with more than 100 people enrolled to diagnose RP. This is the first study comparing chilled to ambient hand ratios in the same individual. Our procedure provided both an estimation of blood flow and bone scintigraphy using a single radioisotope injection in patients with connective tissue disease. It also has the merit of noninvasiveness. A large-scale prospective multicenter study is needed to confirm these results.
99mTc-HDP scintigraphy after one-hand chilling showed high sensitivity and specificity in diagnosing Raynaud’s phenomenon. When the chilled to ambient hand ratio of the initial slope of the activity curve was less than 0.51, the sensitivity was 91.2% and the specificity was 93.3%. The loss of the initial spike curve, the slow progress of the radioactivity curve pattern, and an inhomogeneous radioactivity uptake in either hand were additional characteristic findings of patients with RP. Our results may help to diagnose RP more accurately.
Acknowledgments
We are grateful to Mi Young Lee, the nurse for rheumatology, who assisted with nailfold capillaroscopy, and Chang Ho Kim, Bong Soo Kim, and Hyun Sook Hwang, the nuclear medicine technologists, who operated instruments and software for the scintigraphy.
Footnotes
-
Supported by an Inha University Research Grant (INHA-36122-1), Republic of Korea.
- Accepted for publication March 5, 2009.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.