

To the Editor:
The controversies surrounding fibromyalgia (FM) and the absolute mess the diagnostic label of “fibromyalgia” has created were recently reviewed1⇓–3. Unfortunately, not one of the articles addresses the fundamental problem that exists within the construct of the FM diagnosis: the fallacy of pain from nowhere. While the unifying theme across the 3 articles is that FM is a dead-end diagnosis begging for definition and context, they fail to address the fact that absolutely nobody has actually identified the source of the pain that patients suffer. Clearly, abnormalities in pain-processing with central sensitization to external pain stimulation have been well documented in FM, and it has been widely accepted in standard reviews and textbooks, without argument, that it is from here that FM pain arises4⇓⇓⇓–8. However, there is absolutely no evidence that central sensitization actually causes spontaneous, non-externally stimulated pain. The implication that the pain of FM arises out of a central sensitization syndrome, despite the knowledge that central sensitization is a modification response to actively induced pain and not a source of pain itself9,10, is a true failure of medical science. Central sensitization does not cause pain. It simply modulates pain from a defined, active pain source. Further, there is absolutely no evidence that primary FM is a true central pain syndrome with pain originating from abnormalities of the central nervous system, such as are seen in brain and spinal cord vascular lesions, traumatic injury, tumors, inflammation, and infection; multiple sclerosis; syringomyelia and syringobulbia; epilepsy; and Parkinson’s disease11.
Incredibly, after nearly 200 years of observation and description, FM remains an unexplained syndrome characterized, and accepted by healthcare providers, as a disorder of pain from nowhere. We know precious little about it4⇓⇓⇓–8. We do not know the cause, mechanism, or relationship of the myriad FM symptoms, including pain, stiffness, fatigue, sleep disturbances, cognitive impairment, and psychological distress. The trigger for FM is unknown despite the array of disparate processes reported with the onset of FM. The mechanism of how FM develops is unknown.
We do know that individuals with FM demonstrate central sensitization-driven abnormal pain-processing to extrinsically applied stimuli with features of pain amplification and magnification, wind-up, and referred pain. Clinically, patients have varying degrees and distributions of extrinsically induced tenderness in the form of hyperalgesia or allodynia that actually correlate strongly with psychological distress, generalized distress, sleep difficulties, and depression, but not with the perceived pain itself. We also know that most studies regarding treatment of FM demonstrate only some degree of benefit, in the 30% improvement range or less, for only some symptoms, for only some patients, and usually in the short term. Rarely do patients get a high degree of benefit, such as a 50% reduction in symptoms, especially the pain component12. Finally, we know that, overall, the prognosis for patients with FM is dismal and that overall, patients do not get better4⇓⇓⇓–8.
How did we get here? As described in my recently published book, The Missing Pieces of the Fibromyalgia Puzzle13, I propose that everything went wrong in the world of FM with the publication of the American College of Rheumatology (ACR) 1990 criteria for the classification of FM14. While the intent was to develop criteria to define patients for research purposes, the criteria were quickly subverted to become diagnostic criteria, a purpose for which they were never developed. Herein lies the problem. The ACR criteria study itself refutes the diagnostic validity of the criteria. Based on the derived sensitivity and specificity data, and using a 2% population prevalence of FM, the positive predictive value of widespread pain and painful tenderness in at least 11/18 FM points to diagnose FM is 8.8/100. Out of 100 individuals with widespread pain and at least 11/18 painfully tender FM points, 8.8 have FM, and 91.2 do not. The ACR classification criteria do not diagnose FM.
If in fact the ACR classification criteria do not diagnose FM, then it is reasonable to ask what do patients with widespread pain as defined by the ACR classification criteria and at least 11/18 painfully tender FM points really have, and where does their pain come from? To answer this question, I undertook a detailed and thorough clinical study of 92 patients with widespread pain and tenderness to identify all the clinical features associated with FM, with a particular emphasis on the musculoskeletal, soft tissue, and pain threshold assessment. The details are published in my book13. The conclusion of the study identified that all patients had: (1) primary generalized osteoarthritis predominantly involving the neck and back, with associated degenerative disc disease and a variable combination of tendinitis, bursitis, and fasciitis; and (2) tenderness with increased nociception. All patients had a true source of nociceptive pain, manifested by primary generalized osteoarthritis predominantly involving the cervical spine and lumbar spine with associated degenerative disc disease, and variable combinations of involvement of the thoracic spine with associated degenerative disc disease, thumb carpometacarpal joints, thumb first metacarpophalangeal joints, finger distal interphalangeal and proximal interphalangeal (PIP) joints, knee and patellofemoral joints, toe metatarsophalangeal and PIP joints, and other specific joint sites as well as variable combinations of periarticular symptoms and findings including trochanteric bursitis, plantar fasciitis, subacromial bursitis/supraspinatus tendinitis, pes anserine bursitis, flexor nodule painful tenderness, deep Achilles bursitis, epicondylitis, de Quervain’s tenosynovitis, Achilles insertion tendinitis, and finger flexor tenosynovitis.
Based on the observation that patients with widespread pain and tenderness have true musculoskeletal sources of pain, I developed the 2-component Polypain Model as shown in Figure 1. Polypain is an acronym for polyregional pain and increased nociception. The Polypain Model comports with and fully consolidates the observed abnormalities of pain-processing in FM by identifying the nociceptive pain processes that central sensitization acts upon in FM. The model identifies the independent contribution of primary generalized osteoarthritis predominantly involving the neck and back with associated degenerative disc disease and the variable combination of tendinitis, bursitis, and fasciitis to the overall perceived pain in FM. The Polypain Model explains how the pain sources themselves, sleep disruption, and psychological factors affect pain thresholds through pain-processing and central sensitization. Most importantly, the model provides an integrated and unified framework to more appropriately understand and ultimately measure the contribution of the pain sources and the factors affecting pain thresholds via pain-processing and central sensitization to the overall perception of pain reported by the patient with FM.
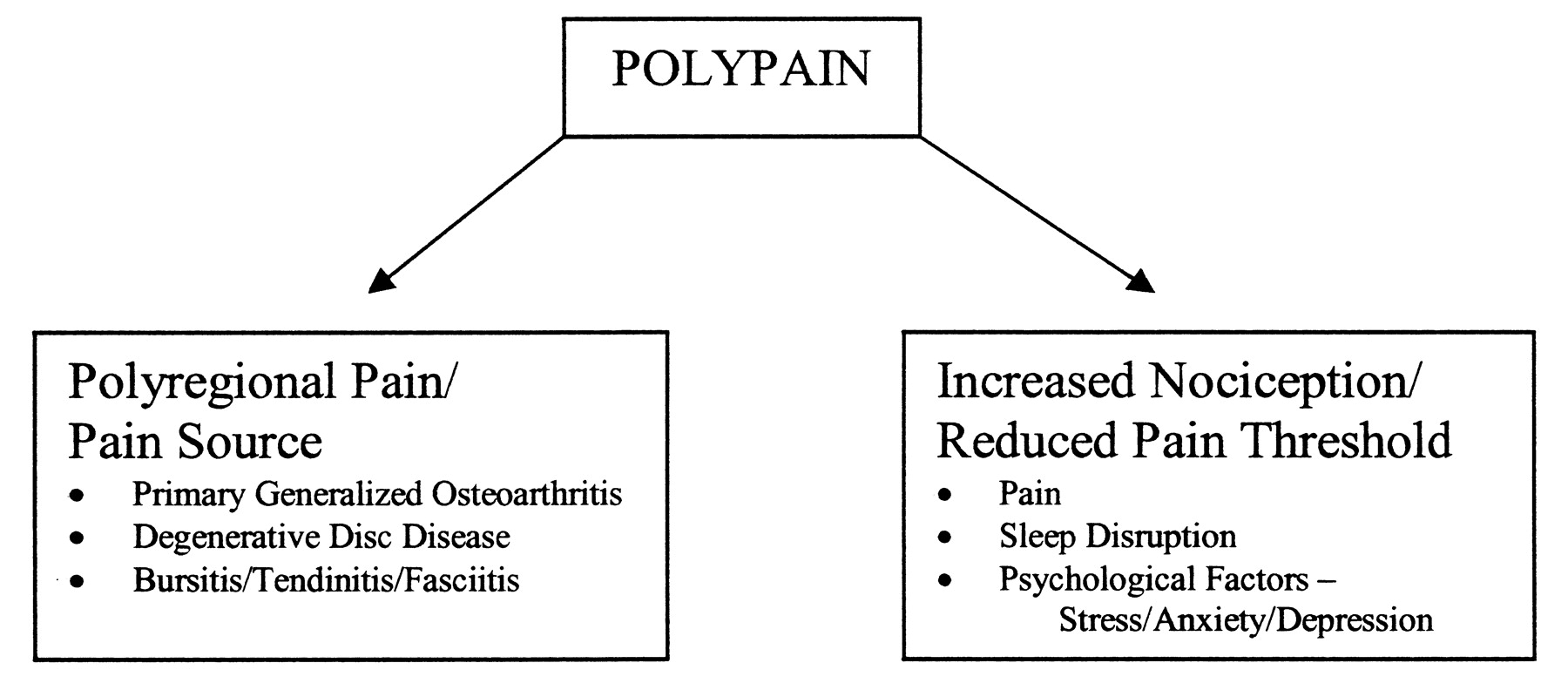
The Polypain Model. (Sarkozi J. The missing pieces of the fibromyalgia puzzle. Santa Ana: Sagecoast Publishing; 2009. Reprinted with permission.)
The recognition that FM polypain is indeed a musculoskeletal disease whose presentation is modified by factors modulating pain message greatly expands the ability to more rationally and effectively treat FM beyond the current pharmacological interventions limited to one-dimensional central sensitization. Further, the ability to stratify and classify patients based on the specific components that cause pain and modulate the pain message provides the opportunity to develop more specific and targeted treatment strategies based upon the specific contributors to the perceived pain and to create more homogeneous patient subsets for purposes of study.
Thus, FM polypain is all about osteoarthritis, degenerative disc disease, tendinitis, bursitis, and fasciitis. These are unquestionably rheumatologic disease conditions that should always be diagnosed and managed by a rheumatologist. In the face of this, the recommendation by Shir and Fitzcharles for rheumatologists to abandon their care of patients with FM1 should itself be abandoned. Moreover, the Polypain Model should reinvigorate rheumatologists to better define themselves as the most qualified specialists to diagnose, treat, and otherwise manage the musculoskeletal and pain components of chronic widespread musculoskeletal pain. To further enhance the central role rheumatologists play in FM polypain, it is vital to reassert and expand the role of rheumatologists in managing the preeminent component of chronic musculoskeletal pain: the pain and its source.








{kind=link}