Article Text

Statistics from Altmetric.com
Adalimumab is an effective treatment for rheumatoid arthritis. However, a substantial proportion of patients with rheumatoid arthritis either do not respond or lose their initial response.1 We report a patient who initially responded to adalimumab treatment, but in whom disease activity increased as treatment continued. We believe that this lack of response to adalimumab is probably caused by the formation of human anti-human antibodies (HAHAs).
A 69-year-old woman with rheumatoid arthritis (diagnosed in 1991) and progressive joint destruction had active disease despite treatment with methotrexate 10 mg weekly and prednisone 7.5 mg/day. Therefore, treatment with adalimumab, 40 mg every other week, was started, in combination with methotrexate 10 mg weekly.
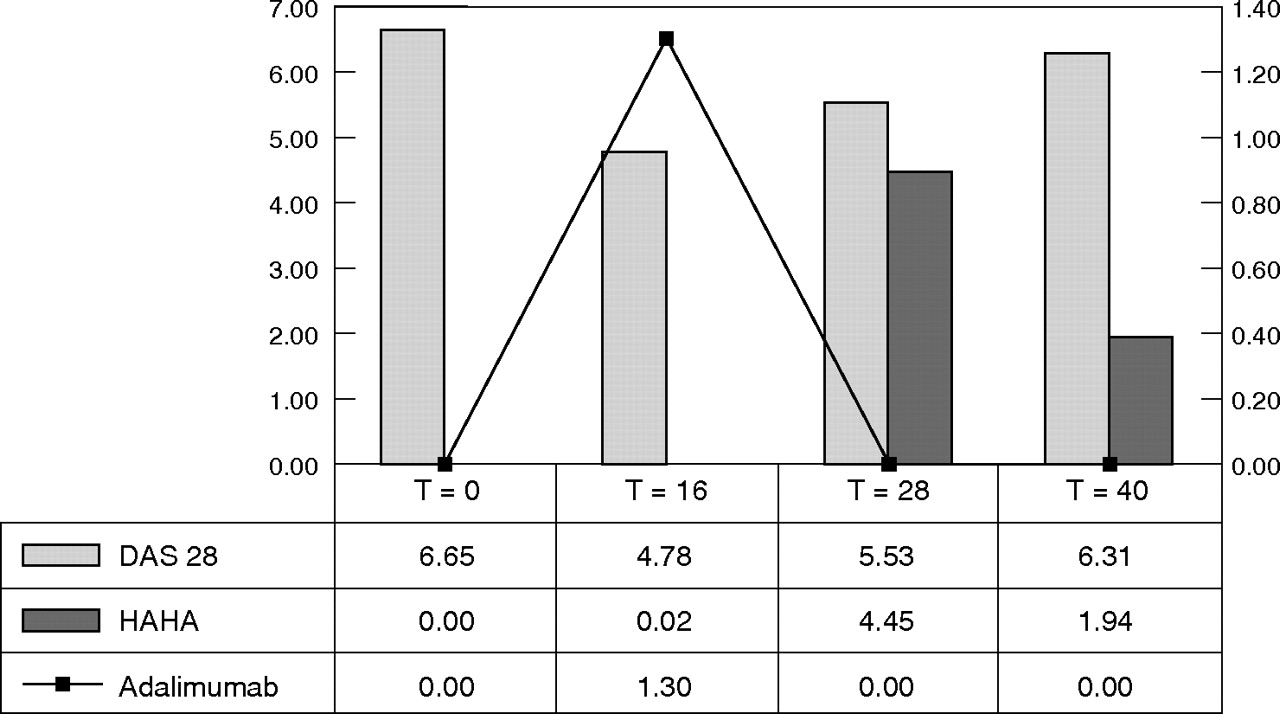
After 16 weeks of adalimumab treatment, the patient’s Disease Activity Score 28 had decreased from 6.65 to 4.78 (table 1).2 According to the Eular response criteria, this qualifies as a (moderate) responder.
Development of disease activity parameters
At week 20, treatment with adalimumab and methotrexate was stopped for 8 and 4 weeks, respectively, for the patient to undergo total knee replacement surgery. Despite restarting adalimumab and methotrexate, disease activity remained high for the subsequent weeks. Hence, from week 35 onwards adalimumab 40 mg was given weekly instead of every other week, but disease activity nevertheless remained high. Therefore, treatment with etanercept was started and this change resulted in a substantial improvement of disease activity. Serum trough levels of adalimumab were measured by enzyme-linked immunosorbent assay, similar to that described for infliximab elsewhere (fig 1).3
{kind=link}
Course of Disease Activity Score (DAS) in relationship to serum adalimumab levels (µg/ml) and serum levels of antibodies (AU/cl). HAHA, human anti-human antibodies.
Serum levels of HAHAs were detected by a newly developed radioimmunoassay, a specific assay measuring high avid antibodies against adalimumab, similar to that described for rituximab.4
HAHAs were present after cessation of treatment for the planned surgical procedure, whereas serum levels of adalimumab were undetectable (fig 1). As levels of HAHAs increased, levels of adalimumab dropped and disease activity increased.
Our patient developed HAHAs to adalimumab despite the fact that adalimumab is a human monoclonal antibody. Infliximab is a chimeric antibody and can induce an immunogenic reaction in the form of human antichimeric antibodies. The development of HACAs to infliximab is associated with a reduced response to treatment,5 and so far such relationships have not been described for adalimumab.
In our patient, the anti-rheumatic drug-free period may have influenced the development of HAHAs. The absence of the protective role of methotrexate may have stimulated the formation of HAHAs. Another possibility is that continuous high levels of adalimumab induced immunotolerance, and when adalimumab treatment was discontinued, serum levels dropped and HAHAs developed.
A substantial number of patients with rheumatoid arthritis have persistent disease activity despite treatment with adalimumab. As shown by our patient, the formation of HAHAs to adalimumab may be an explanation for failure of adalimumab treatment. Treatment with another tumour necrosis blocking factor may be an option in such cases.
Footnotes
-
Competing interests: None.
-
Informed consent was obtained for publication of the patient’s details described in this report.
Ethical approval: Ethics committee approval was secured for the study reported by the Stichting Slotervaartziekenhuis, Medisch Ethische Toetsingscommissie, Amsterdam.