Article Text

Statistics from Altmetric.com
Enthesitis, the inflammation involving the insertion of tendons, ligaments and joint capsule is a characteristic sign and hallmark of several rheumatic diseases in both adult and paediatric patients. The change in the perception of enthesitis (ie, its growing significance as a clinicopathological entity) is best reflected in the new European League Against Rheumatism (EULAR) recommendations for psoriatic arthritis, which recommend antitumour necrosis factor therapy for patients with active enthesitis and/or dactylitis and insufficient response to non-steroidal anti-inflammatory drugs or local steroid injections.1 It is also one of three entry criteria (the other two being arthritis and dactylitis) for the new Assessment of SpondyloArthritis Society classification criteria for peripheral spondylarthritis.2 Broadly, enthesitis can be evaluated either clinically or by one of several imaging modalities that have been validated to various extents for the assessment thereof.
A recent systematic literature review that examined the US definition of enthesitis found large variability in the definitions utilised to outline enthesitis.3 Indeed, the appropriate definition of enthesitis and of its components remains an issue that is crucial for the evaluation of enthesitis with any given imaging modality. As of yet, we have no single examining modality that is capable of evaluating all of these components.
Clinical examination may aid in the detection of enthesitis when palpation is used to trigger pain or tenderness. However, it only allows the detection of soft tissue swelling, including tendon thickening and accompanying bursitis, two key features of enthesitis, while failing to provide information on typical bony changes, ie, bone erosions, enthesophytes and calcifications. Clinical evaluation has been shown to underestimate enthesitis involvement compared with imaging modalities.3,–,6 Contrary to clinical evaluation, conventional radiography is useful for assessing bony changes, as described above, but does not permit the evaluation of soft tissue changes. MRI and ultrasound have clear advantages over both clinical examination and conventional radiography, in that they are capable of providing information with respect to both bony changes and soft tissue processes.
MRI is increasingly investigated for its use in assessing enthesitis mainly in ankylosing spondylitis, in which it is capable of detecting diffuse bone oedema associated with surrounding soft tissue oedema in the region adjacent to enthesis.7 MRI is the imaging modality of choice for assessing bone marrow oedema; however, this may occur in a number of distinct diseases,8,–,11 histopathological correlation is moderate,9 and results from several studies have questioned its specificity as a strictly pathological phenomenon.11,–,13 When soft tissue involvement occurs in a synovial joint, synovitis may mask some, if not all, MRI features of enthesitis.14 Interestingly, a recent investigation revealed that bone marrow oedema was the most specific finding on non-contrast MRI of the hands and wrists in rheumatoid arthritis.15 However, MRI cannot be considered as a gold standard as it lacks sensitivity and specificity for peripheral enthesitis,16,–,18 due to the anatomical build-up of the entheses, which is unfavourable for visualisation using MRI due to the low water content of the fibrocartilage component of the enthesis.
Ultrasound is an imaging tool that has been increasingly utilised in the past two decades for the assessment of enthesitis.3 4 19,–,24 Ultrasound is capable of demonstrating and evaluating both soft tissue and bony changes, and additionally may also be used to assess the vascularisation and blood flow in the enthesis by colour or power Doppler.25 26 A recent systematic literature review that examined the ultrasound definition of enthesitis found evidence supporting face, content validity and reliability for the evaluation of enthesitis.3 This review concluded that ultrasound demonstrated face and content validity, but that criterion and construct validity may not be properly evaluated lacking a gold standard comparator.
However, with increased sensitivity comes the price of reduced specificity. Previous studies have shown that certain components of enthesitis such as bony changes, tendon thickening, etc. cannot be adequately distinguished from entheseal involvement due to both mechanical and degenerative processes.19 27 The detection of subclinical enthesitis in clinically asymptomatic regions in patients with psoriatic arthritis28 29 highlights the discrepancy between clinical symptoms (eg, pain or tenderness) and imaging phenomena interpreted as a pathological findings. It also raises awareness to the possibility of inappropriate labelling of otherwise healthy individuals as patients and of erroneous diagnosis based on certain imaging phenomena, which can, in certain cases, be considered components of enthesitis, but that may be detected in the absence of an inflammatory involvement of the entheses.
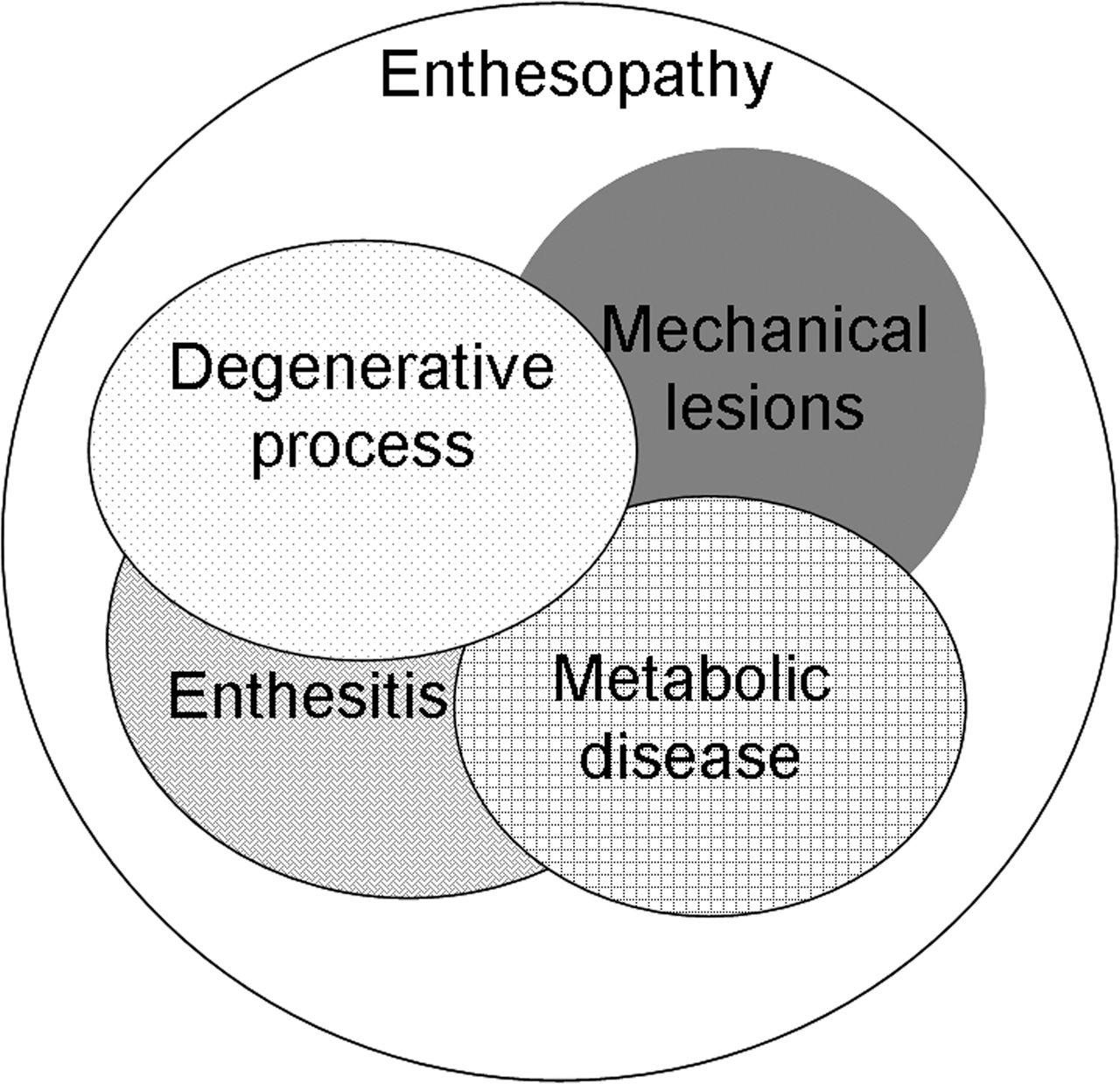
Feydy and colleagues30 report the results of a comparative study of MRI and power Doppler ultrasound of the heel in patients with spondylarthritis with and without heel pain and in controls. In their article the authors use the term enthesopathy, rather than enthesitis, because the term enthesitis remains undefined in the context of ultrasound. This underscores the importance of terminology, with enthesopathy corresponding to a group term encompassing all forms of entheseal involvement, which may be caused by different aetiologies (figure 1). Within this group the term enthesitis refers to entheseal involvement in the context of an inflammatory rheumatic disease. The Outcome Measures in Rheumatoid Arthritis Clinical Trials (OMERACT) Ultrasound Group consensus definition for enthesopathy requires the presence of tendon or ligament pathology, manifested as either loss of normal echostructure and/or thickening seen in two planes.31 Doppler signal and bony changes are included as optional findings. The recent systematic review on the ultrasound evaluation of enthesitis found that enthesitis was most commonly characterised by increased thickness and hypoechogenicity (94% and 83% of studies, respectively) of the tendon in the studies included.3

{kind=link}
Aetiological classification of enthesopathy.
Feydy and colleagues30 divide the components of enthesopathy according to the imaging modalities utilised into two groups, that of early and chronic changes, responding broadly to soft tissue and bony changes. This classification is similar to that used in the Glasgow ultrasound enthesitis scoring system score, the most widely used patient-level scoring system for enthesitis, which groups inflammatory and damage signs.4
Both MRI and ultrasound, but the latter in particular, are ‘plagued’ by artefacts. The authors appropriately address this issue, especially with regard to the interpretation of the power Doppler signal, seen by many as an important sign distinguishing between enthesitis, as entheseal involvement in the framework of an inflammatory condition rather than tendon insertion pathology related to mechanical damage.25 26 Similarly, bursitis associated with the enthesis might be an additional sign that facilitates the distinction between aetiologies. Such issues, however, need to be addressed in further studies because of the contradictory results of the available studies.
A consensus ultrasound definition on enthesitis would be crucial to conduct much needed and important studies on enthesitis. Such studies, which aim to provide an appropriate definition with respect to any imaging modality, should ideally be multicentre studies in which the average age of patients is relatively young to ensure the scarcity of tendon damage and changes due to mechanical or metabolic causes. Having younger patients is also important if one wants to look for early signs of disease—ie, soft tissue changes that are more likely to help in distinguishing inflammatory versus mechanical tendon insertion involvement. Gender distribution may also have considerable effects on the results of such a study, due to the increased prevalence of ankylosing spondylitis in men compared with women—a phenomenon not observed in heel pain caused by mechanical injury.
It is important to use validated instruments and to utilise standard reference values, the latter should, however, be adapted to the study population, which might differ considerably from the original population on which these were developed. When considering clinical examination it is important whether only swelling and/or tenderness are considered.4 27
In order to evaluate the capacity of ultrasound, MRI or indeed other imaging techniques to differentiate between enthesitis and other forms of enthesopathy, a control group consisting of healthy age and sex-matched individuals is required. Additional groups of patients with enthesopathy due to causes other than inflammatory rheumatic disease also need to be included. When evaluating the utility of imaging modalities with respect to specific regions or single entheses of special interest, such as the calcaneal insertion of the Achilles tendon/plantar aponeurosis, this necessitates groups of patients with heel pain of different aetiology, for example, heel pain in the framework of enthesitis versus heel pain caused by mechanical injury.
Despite considerable advances made recently in the use of imaging modalities for the evaluation of entheses, differentiation between the different manifestations of enthesopathy only remains reliably possible in the context of available clinical information.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed.