Article Text

Statistics from Altmetric.com
Psoriatic arthritis (PsA) is now recognised as a potentially severe form of arthritis associated with skin and nail involvement. Targeted biological treatments have been introduced to treat it and, in many cases, are administered in combination with disease-modifying antirheumatic drugs (DMARD) such as methotrexate and ciclosporin.1 Previous randomised clinical trials of anti-tumour necrosis factor alpha drugs have failed to demonstrate that PsA patients receiving concomitant methotrexate show any greater clinical improvement than those receiving monotherapy.2,–,4 However, the Norwegian DMARD register5 and Kristensen et al6 found that the absence of concomitant methotrexate was a predictor of premature treatment discontinuation in patients with PsA. D'Angelo et al7 have reported that the addition of ciclosporin to etanercept seems to be a safe and effective treatment for PsA patients with uncontrolled cutaneous disease.
The primary objective of this open-label, randomised clinical trial was to compare the efficacy and tolerability of the combination of etanercept and ciclosporin with the efficacy and tolerability of etanercept and methotrexate in a cohort of 41 patients with moderate/severe PsA after 6 months' follow-up.
The study involved 41 PsA patients fulfilling the classification criteria for PsA,8 with prevalently peripheral arthritis9 who were resistant to at least one DMARD. The study design included a 4-week washout period, after which all of the patients subcutaneously received etanercept at a dose of 50 mg once a week for 6 months in combination with methotrexate (7.5–15 mg/week) or ciclosporin (3 mg/kg per day). None of the patients received steroids during the study.
All of the patients gave their written informed consent to the study, which was approved by the local ethics committee.
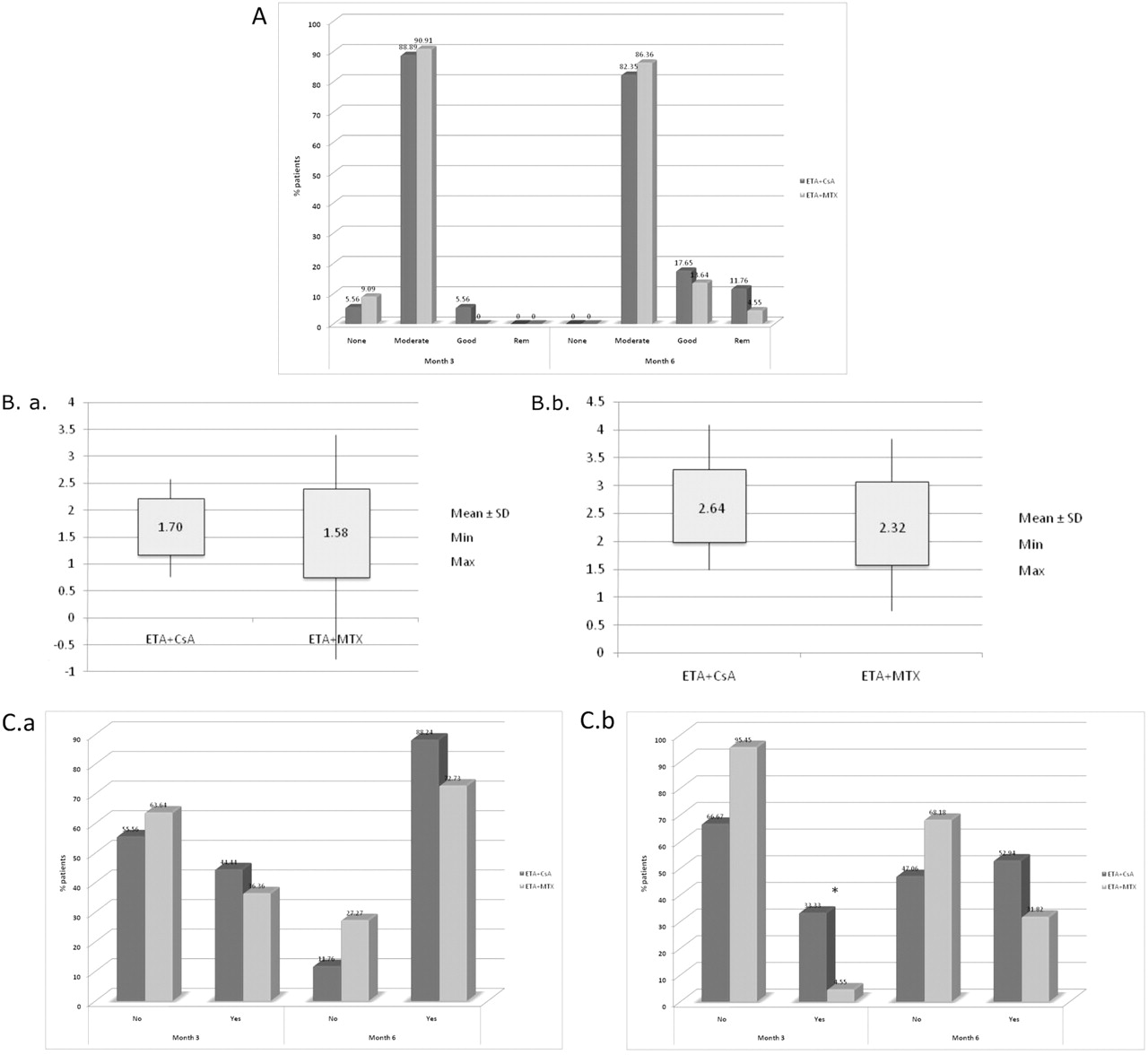
Table 1 shows that the two treatment groups were homogeneous in terms of age, gender and disease duration. Both groups showed a clinical response on the basis of the mean decrease in the 28-joint disease activity index (DAS28) after 3 months (etanercept plus ciclosporin 1.70±0.52 vs etanercept plus methotrexate 1.58±0.82, p=0.56) and 6 months (etanercept plus ciclosporin 2.64±0.66 vs etanercept plus methotrexate 2.32±0.74, p=0.22) (figure 1A). At the 6-month follow-up evaluation, two of the patients in the etanercept plus ciclosporin group and one in the etanercept plus methotrexate group had DAS28 scores of 2.6 or less and were considered to be in remission. A good clinical European League Against Rheumatism response according to DAS28 was observed in one patient in the etanercept plus +ciclosporin group and none in the etanercept plus methotrexate group after 3 months, and in three patients in both groups after 6 months. Three patients failed to achieve a clinical response after 3 months (one in the etanercept plus ciclosporin group and two in the etanercept plus methotrexate group) (figure 1B). The psoriatic area and severity index (PASI) 50 and PASI 75 scores were achieved after 6 months by 88% and 53%, respectively, of the patients in the etanercept plus ciclosporin group, and 73% and 32%, respectively, of the patients in the etanercept plus methotrexate group (p<0.05) (figure 1C).

{kind=link}
(A) European League Against Rheumatism response rates 3 and 6 months after; (B.a) Disease activity score in 28 joints (DAS28)–erythrocyte sedimentation rate (ESR) changes (month 3); (B.b) DAS28–ESR changes (month 6); (C.a) psoriatic area and severity index (PASI) 50 response rates 3–6 months; (C.b) PASI 75 response rates 3–6 months.
Baseline characteristics of the study population
There was no significant difference in serious adverse events between the two treatment groups, except for hypertension, which was statistically more frequent in the etanercept plus ciclosporin group and led to the drop out of one patient and the start of antihypertensive treatment in three who did not discontinue the ciclosporin treatment. None of the patients treated with etanercept plus methotrexate showed a significant increase in liver enzymes; two patients treated with etanercept plus ciclosporin reported an increase in the creatinine value although within the normal range. One patient in the etanercept plus ciclosporin group was lost to follow-up.
The results of this study show that etanercept plus ciclosporin was as effective as etanercept plus methotrexate in terms of DAS28 scores in patients with moderate/severe PsA and peripheral arthritis, but it was more efficacious in reducing psoriatic skin involvement. However, further studies of larger patient series and with a longer follow-up are necessary to confirm our findings.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the local ethics committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.