Article Text

Statistics from Altmetric.com
Psoriatic arthritis is a complex heterogeneous disease manifesting with skin disease and a number of musculoskeletal abnormalities including arthritis, enthesitis, dactylitis and spondylitis. While not all of these manifestations are present in every patient, assessment of disease activity should account for these domains. To combine these domains into one composite score has been challenging but several have been developed. The Psoriatic Arthritis Disease Activity Score (PASDAS) was developed as part of an international Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) exercise.1 This measure includes physician-reported and patient-reported outcome measures combined into a composite index. The PASDAS requires the patient to complete a visual analogue scale and the short form 36 (SF36). The latter consists of 36 questions covering domains of physical and mental health. A shorter, 12 question version, has been developed—the SF12.2 Since the burden of completing patient-reported outcomes may be substantial, the substitution of the SF12 for the SF36 would reduce this burden, and may facilitate use of this measure in practice. We have re-analysed the data from the GRAPPA Composite disease Exercise (GRACE)1 to investigate if substitution of the physical component subscale derived from the SF12 substantially alters scores on the PASDAS. The GRACE study was a large observational study of 503 patients with psoriatic arthritis (PsA) with data collected at 32 centres affiliated worldwide with GRAPPA. A large range of clinical data and patient-reported outcomes were collected at baseline, 3 months, 6 months and 12 months. At each visit, treatment changes were noted: treatment escalation was used as a surrogate for an active disease state.
The two versions of the physical component subscale of the SF36 (physical component score 36 (PCS36) and PCS12) were compared by calculating the difference between the scores and expressing this as a mean and SD. Both calculated versions of the physical component subscale (one derived from the SF36 and one from the SF12) were used in calculating two versions of the PASDAS: PASDAS36 and PASDAS12. These two versions were compared by calculating the difference in scores and by expressing the difference in terms of a Bland-Altman plot.
In total there were 1077 paired observations of PCS12 and PCS36. The mean (SD, min and max) for PCS36 was 39.14 (11.61, 9.75–63.50) and for PCS12 40.42 (10.96, 14.44–62.19). The mean difference between the scores was –1.26, SD 3.37, min −13.33, max 10.21. Figure 1 displays the relationship between the two scores: the Pearson's correlation coefficient was 0.96.

Scatter plot of scores for the PCS-SF12 and PCS-SF36. SF36, short form 36.
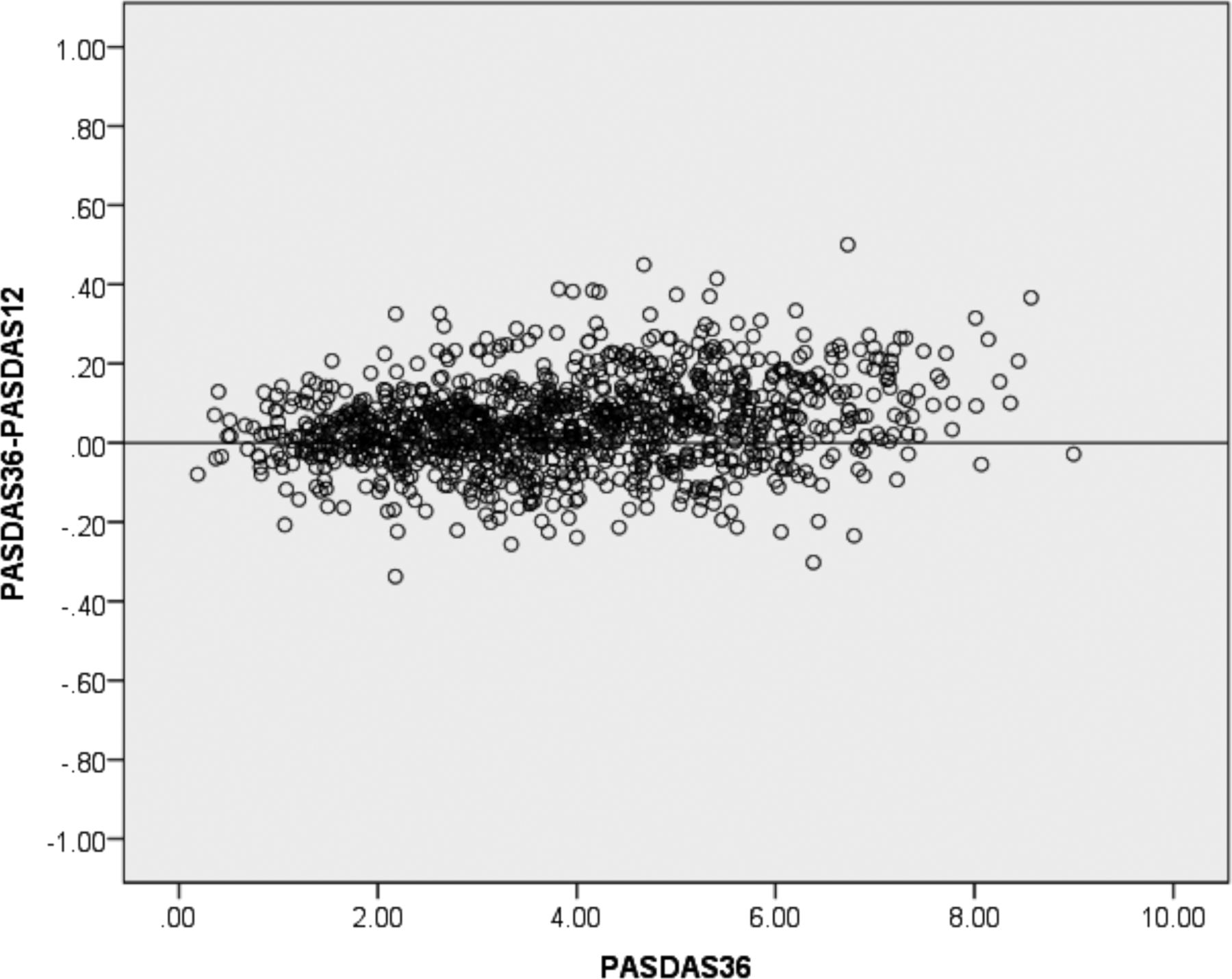
The mean (SD, min and max) scores for PASDAS36 and PASDAS12 were 3.91 (1.69, 0.19–9.00) and 3.86 (1.67, 0.27–9.03), respectively. Pearson's correlation was 0.99. The mean difference between scores was 0.47, SD 0.11, min 0.34, max 0.50. The Bland-Altman plot is given in figure 2.

{kind=link}
{kind=link}
Bland-Altman plot. Horizontal axis is PASDAS calculated using PCS-SF36. Vertical axis is the difference between the scores for each patient: PASDAS calculated using the PCS-SF36 and PASDAS calculated using the PCS-SF12. SF36, short form 36.
Despite the proliferation of new PsA-specific composite outcome measures and the recommendation for a treat-to-target approach3 we know anecdotally that this is currently not routinely performed.4 The Minimal Disease Activity criteria5 offer simplicity and brevity but remain a binary outcome and cannot function as a disease activity measure. The PASDAS, along with others, offers both a target and a disease activity state assessment across important clinical domains. Assessment of these domains requires clinical evaluation, in addition to several patient-reported measures. Of the disease activity measures currently proposed, the PASDAS is the only one derived from real life patient data. The PASDAS currently requires the patient to complete the full SF36. This report demonstrates that the shorter SF12 can function as a valid substitute for the SF36 in the calculation of the PASDAS.
Footnotes
Contributors Both authors contributed equally to this letter.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.