Article Text

Statistics from Altmetric.com
- DMARDs (biologic)
- Health services research
- Rheumatoid Arthritis
- Psoriatic Arthritis
- Ankylosing Spondylitis
Biological agents revolutionised the treatment of chronic inflammatory diseases such as rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriatic arthritis (PsA) as well as Crohn's disease (CD), ulcerative colitis (UC) and psoriasis. RA studies highlighted that uptake of biologic drugs varies strongly across Europe and the income of a country is considered as a major determinant factor for usage.1–3 Putrik et al4 ,5 found that access to biologics in RA—expressed as a composite score of availability, affordability and acceptability—showed a strong positive correlation with gross domestic product (GDP)/capita (r=0.86) in Europe. Much less is known on this topic in AS, PsA and the other three inflammatory diseases.
We analysed real-world biologic usage data and their relationships with GDP/capita in the six inflammatory conditions in Bulgaria, the Czech Republic, Hungary, Poland, Romania and Slovakia. According to our previous literature search, there is no precise and comparable country-specific prevalence data in this region.6–8 Therefore, we estimated the biologic treatment rates per 100 000 inhabitants.
Considering the total of six diagnoses, we found only moderate positive correlation (r=0.34, p=0.506) between biologic usage and GDP/capita levels (figure 1). An approximately eightfold difference in treatment rate was observed between Hungary and Poland despite their almost identical GDP/capita. Similar treatment rates were found in Romania and the Czech Republic, in contrast to the over twice as high GDP/capita of the latter.

Total number of patients treated with biologics in six inflammatory conditions*/100 000 inhabitants by countries’ per capita GDP. Notes: *rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, Crohn's disease, ulcerative colitis and psoriasis. The size of circles represents the absolute total number of patients in the six chronic inflammatory conditions. Data sources: patient numbers,6–8 per capita GDP (2013): WorldBank Databank. http://data.worldbank.org/indicator/NY.GDP.PCAP.CD/countries?display=default. Accessed 26 June 2015. Population data: Eurostat (2013) Eurostat Statistics Database, 2013. http://epp.eurostat.ec.europa.eu/portal/page/portal/statistics/search_database. Accessed 26 June 2015. BGR, Bulgaria; CZE, Czech Republic; GDP, gross domestic product; HUN, Hungary; POL, Poland; ROM, Romania; SVK, Slovakia.
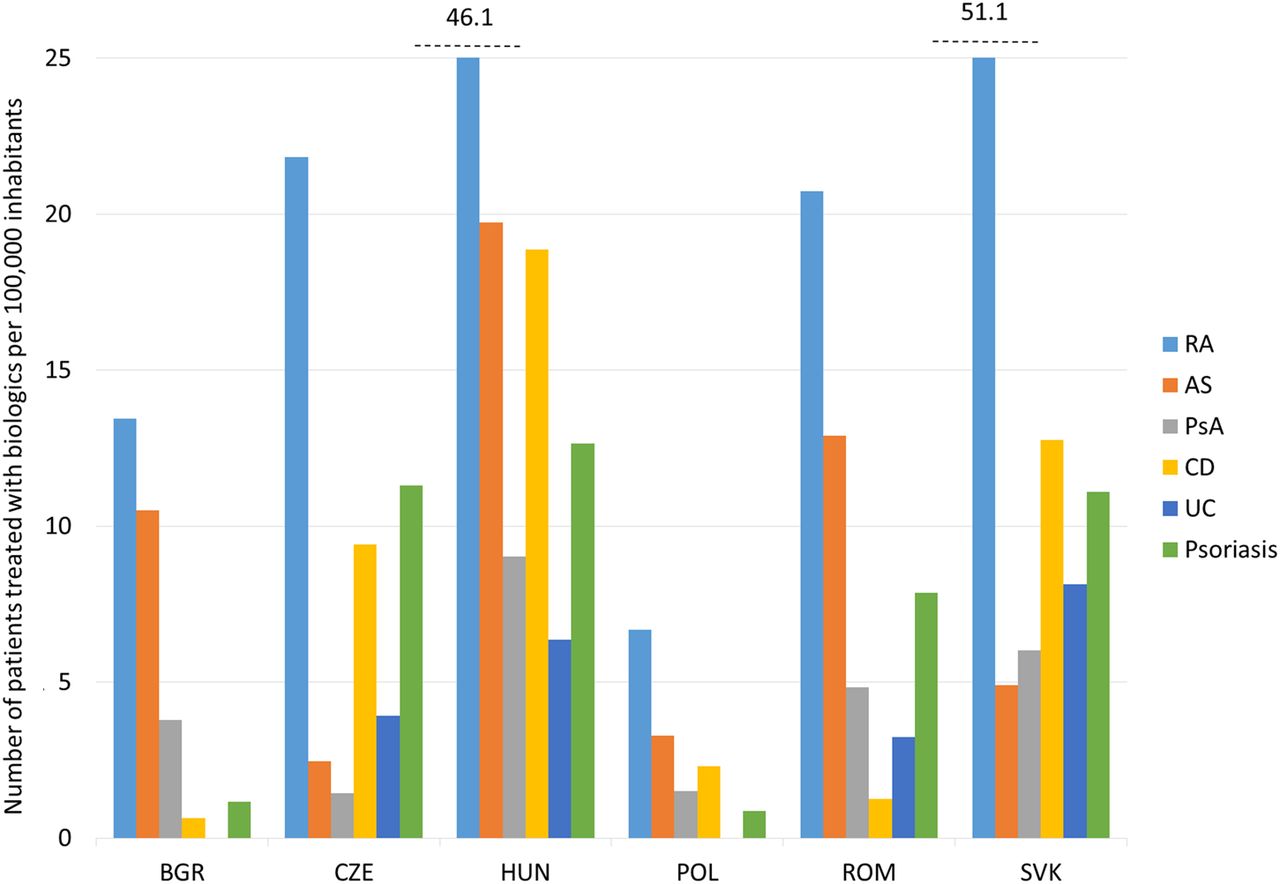
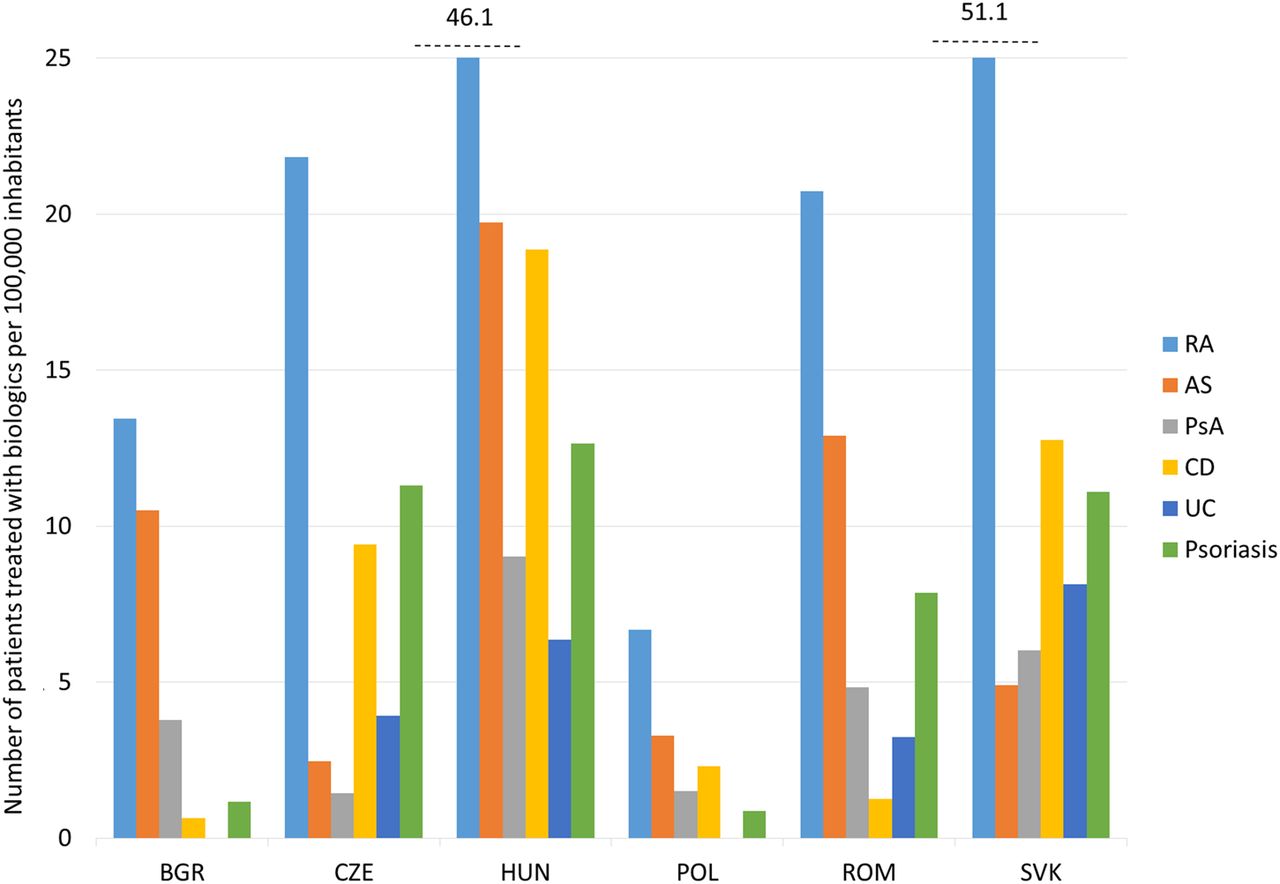
Analysis by diagnosis revealed the highest cross-country difference in treatment rates in CD (30-fold), followed by psoriasis (15-fold) (figure 2) Although the same rheumatology centres are entitled to prescribe biologics for all the three rheumatic conditions, the difference in treatment rates between countries is higher in RA and AS (equally eightfold) than in PsA (sixfold).
{kind=link}
{kind=link}
Total number of patients treated with biologics in six inflammatory conditions*/100 000 inhabitants. Notes: *rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriatic arthritis (PsA), Crohn's disease (CD), ulcerative colitis (UC) and psoriasis. Data sources: patient numbers,6–8 per capita GDP (2013): WorldBank Databank. http://data.worldbank.org/indicator/NY.GDP.PCAP.CD/countries?display=default. Accessed 26 June 2015. Population data: Eurostat (2013) Eurostat Statistics Database, 2013. http://epp.eurostat.ec.europa.eu/portal/page/portal/statistics/search_database. Accessed 26 June 2015. BGR, Bulgaria; CZE, Czech Republic; GDP, gross domestic product; HUN, Hungary; POL, Poland; ROM, Romania; SVK, Slovakia.
Putrik et al4 found that clinical eligibility criteria for treatment with reimbursed biologics in RA were less restrictive in Slovakia, the most restrictive in Bulgaria, Hungary and Poland, while the Czech Republic and Romania were in between. Using the composite score (range 0–9), they rated Slovakia and the Czech Republic as countries with the best access to biologics (7), followed by Hungary (4), Poland and Romania (3) and Bulgaria (2).5 In contrast, the treatment rate was the highest in Slovakia, followed by Hungary, the Czech Republic, Romania, Bulgaria and the lowest was in Poland (figure 2). The GDP/capita is the highest in the Czech Republic and Slovakia, it is slightly lower in Hungary and Poland but almost twice as high as in Romania and Bulgaria (figure 1).
It is worthy to note that Putrik et al5 made comparisons of countries with much broader differences in GDP. In this study, GDPs are more clustered and this might blunt the effect. Biological usage of six inflammatory conditions were grouped together (figure 1) and we found very large differences between diseases (figure 2) that makes the interpretation of overall factors leading to prescription of biologics more complex. Our results, however, confirm that there is a clear gap between the theoretical access for biological treatment and real-world drug usage. Further investigation is needed on the determinants of inequity. Variations in GDP/capita, prices and cost effectiveness of biologics do not explain alone the differences either between countries or between diseases.6–9 We assume that disease-related disability and achievable health gain with biologics in these conditions are not known, or not used or are valued differently in these countries. Overall, inequity in access to biologics is apparent and can be observed in rheumatology. Although our analyses were performed in Central and Eastern Europe, we assume that similar inequities might occur in other European regions as well.
Footnotes
Contributors The study was planned by LG and MP. Data analysis and conducting the study were performed by FR, VB and PB. GyP and ZSz contributed significantly to the interpretation of data and critically revised the content. The manuscript was drafted by LG, FR and MP. All authors reviewed and approved the final version of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data from the study are available.