Article Text

Statistics from Altmetric.com
Recently, some reports showed the increased expression of CD40 ligand in autoimmune diseases. CD40 ligand can be expressed in a soluble form.1,2 Soluble CD40 ligand (sCD40L) is present in supernatants of in vitro activated T cells in 15 kDa and 18 kDa forms, and these forms are the products of enzymatic cleavage at a metalloproteinase sensitive site in the membrane proximal region of the extracellular domain of the molecule.1 Their abnormalities have been demonstrated in various kinds of diseases such as chronic lymphocytic leukaemia2 or systemic lupus erythematosus.1 But, there has been no report demonstrating the serum levels of sCD40L in patients with eosinophilic fasciitis (EF). In this study we determined the serum levels of sCD40L in patients with EF, and investigated their clinical significance in this disease, in order to evaluate whether sCD40L might be a useful marker for this disease.
METHODS AND RESULTS
Eleven patients (disease duration 1–8 months) with a classic clinical picture of EF, who had received no treatment, were included in this study. All the patients had a recent history of increased skin induration. Skin biopsies including deep subcutaneous tissue and fascia showed markedly indurated and thickened fascia in all cases. Additionally, the thickened fascia contained accumulation of collagen and intense inflammatory cell infiltrates comprising lymphocytes, macrophages, and eosinophils. Clinical manifestations and laboratory findings of each patient were obtained from the medical records. All the laboratory findings were obtained at the time of serum sampling. We also collected control serum samples from 20 healthy volunteers matched for age and sex. Levels of sCD40L were measured with a specific enzyme linked immunosorbent assay (ELISA) kit (Bender MedSystems, Vienna, Austria), according to the manufacturer’s instructions. Values greater than the mean plus 2SD for normal control subjects were regarded as raised. Additionally, serum IgG was evaluated by a turbidimetric immunoassay as described previously.3 Statistical analysis was carried out with Student’s t test for the comparison of means, and Fisher’s exact probability test for the analysis of frequency. Values of p<0.05 were considered significant.
Figure 1 shows the serum sCD40L levels in patients with EF and in the healthy control subjects. The serum sCD40L levels in patients with EF were significantly higher than those in the healthy controls (mean (SD) 0.29 (0.16) ng/ml v 0.13 (0.08) ng/ml, p<0.01). When the cut off value was set at 0.29 ng/ml (mean + 2SD for the controls), raised serum sCD40L levels were seen in 5/11 (45%) patients with EF.
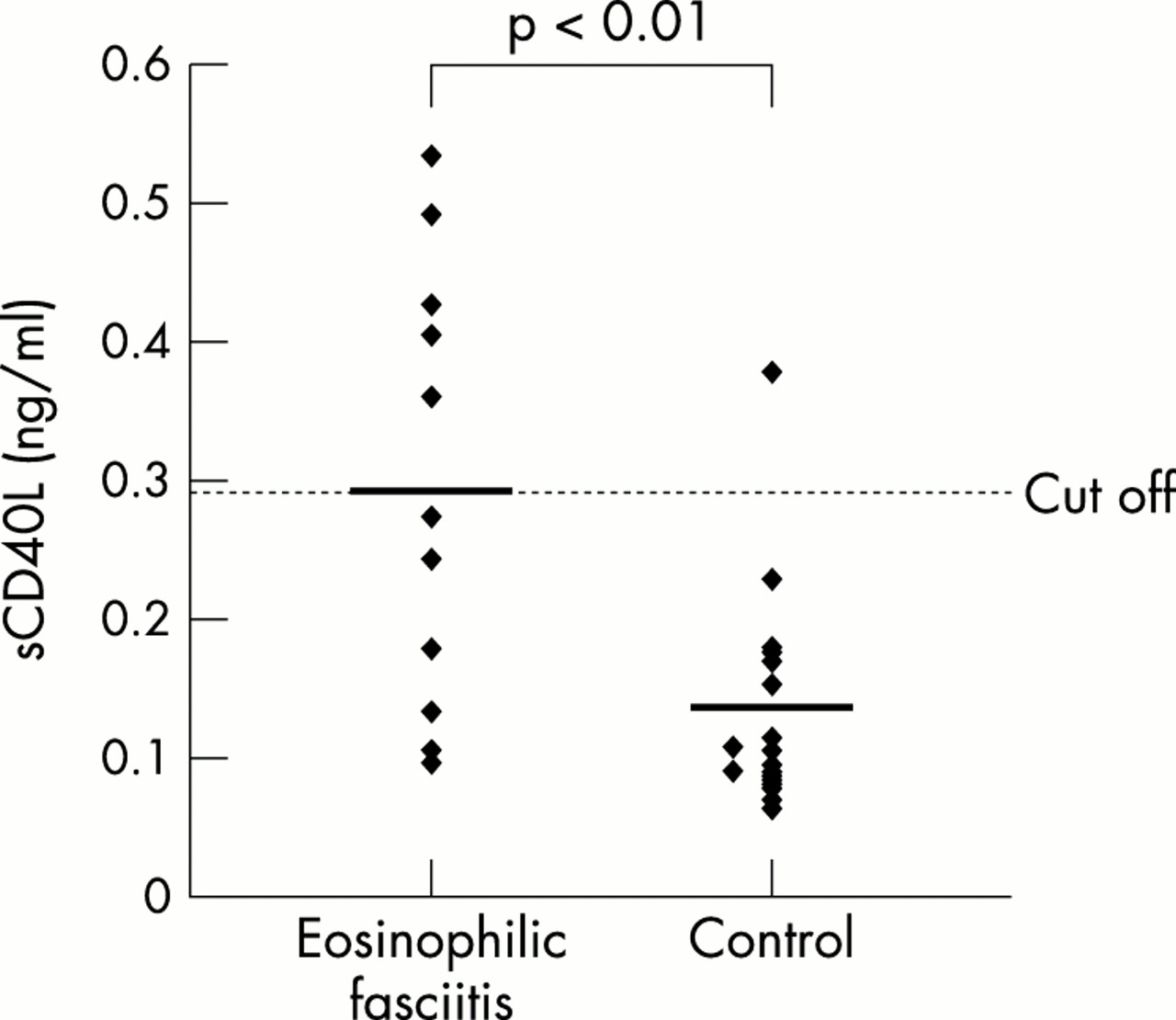
Serum soluble CD40 ligand (sCD40L) levels determined with specific ELISAs in serum samples from patients with EF and healthy control subjects. Bars show means. The horizontal dotted line represents 2SD above the mean value of healthy controls. p Values were determined by Student’s t test.
Serum sCD40L levels correlated significantly with serum IgG levels (r=0.75, p<0.05). On the other hand, serum sCD40L levels were not significantly correlated with serum gammaglobulin, peripheral cell count of eosinophils, erythrocyte sedimentation rate, or serum levels of aldolase. Additionally, three of the five patients with raised serum sCD40L levels were examined longitudinally before and after corticosteroid treatment for two months to three years. Their clinical manifestations and laboratory abnormalities improved with treatment. Serum sCD40L levels became normal in all three patients (fig 2).

{kind=link}
{kind=link}
Longitudinal study of serum soluble CD40 ligand (sCD40L) levels in patients with EF.
DISCUSSION
As described above, expression of sCD40L in patients with several connective tissue diseases has already been evaluated and shown to be increased. Berner et al reported that increased expression of CD40 ligand on CD4+ T cells in rheumatoid arthritis indicated prolonged and increased activation of CD4+ T lymphocytes and was associated with active disease and, possibly, an unfavourable prognosis.4 Valentini et al found that expression of CD40 ligand in activated CD4+ T lymphocytes was increased in patients with systemic sclerosis.5 On the other hand, Vakkalanka et al reported that the mean concentration of serum sCD40L was statistically significantly higher in patients with systemic lupus erythematosus (SLE) than in disease controls or healthy subjects, and segregation of patients with SLE by severe, moderate, or mild extent of disease showed a relationship between disease severity and sCD40L concentration.1 These findings suggest that CD40 ligand or sCD40L are associated with clinical features of these diseases. In our study, serum levels of sCD40L in patients with EF were significantly higher than those in healthy controls. sCD40L is present in supernatants of in vitro activated T cells.1 In patients with EF, activated T cells were thought to be increased because of the presence of raised interleukin 5 and interleukin 10.6 Thus, our results may reflect such a condition. Additionally, serum levels of sCD40L correlated significantly with serum IgG levels in patients with EF, and serum sCD40L levels normalised after treatment in patients with raised sCD40L levels. As well as peripheral cell counts of eosinophils, erythrocyte sedimentation rate or serum levels of aldolase, hypergammaglobulinaemia is reported to be one of the markers of disease activity,7,8 which occurs in 75% of patients and is usually due to a polyclonal increase in IgG.9 Thus, our results suggest that sCD40L is also good marker of EF, reflecting the effects of treatment. However, only 5/11 patients showed raised levels of sCD40L. Thus, the usefulness of sCD40L as a marker of disease activity was not completely substantiated in this study. Additionally, serum sCD40L levels did not correlate with gammaglobulin despite significant correlation with IgG, possibly owing to the small number of patients studied. Moreover, we performed the longitudinal study in only three patients with raised sCD40L levels because other serum samples were not available, so the longitudinal data may be incomplete. Additionally, there is a possibility that corticosteroid treatment, independently of disease, can reduce sCD40L levels. Further studies are needed to clarify the significance of the role of sCD40L in this disease.