Article Text

Statistics from Altmetric.com
Since the introduction of tumour necrosis factor (TNF) antagonists for the treatment of ankylosing spondylitis (AS) the majority of patients can be successfully treated. However, individual patients have persistent disease activity. We report on a 36-year-old male patient with HLA-B27-positive AS. No peripheral arthritis or extra-articular manifestation was documented. After insufficient response to standard treatment with non-steroidal anti-inflammatory drugs (NSAIDs), sulfasalazine, methotrexate and all three available TNF antagonists (infliximab, etanercept and adalimumab), the last of these even in an intensified dose of 40 mg weekly, a rescue treatment with the interleukin 6 (IL-6) antagonist tocilizumab (TCZ; Roche Pharma, Roche Pharma, Grenzach-Wyhlen, Germany) was initiated.
TCZ was administered intravenously with 8 mg/kg bodyweight every 4 weeks. Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) served as clinical response measure. For functional assessment the Bath Ankylosing Spondylitis Functional Index (BASFI) and the Bath Ankylosing Spondylitis Metrology Index (BASMI) were applied. For global assessment, considering as well the inflammatory markers, the Ankylosing Spondylitis Assessment Study (ASAS) criteria1 as well as the new Ankylosing Spondylitis Disease Activity Score (ASDAS) C2 were evaluated. Spinal inflammation was monitored by whole-spine MRI before, after 6 weeks and after 18 weeks of treatment. For safety reasons laboratory liver and kidney function, cholesterol/triglycerides and differential blood count were evaluated every 4 weeks.
After 4 weeks the patient already reported less pain and morning stiffness. At week 26 morning stiffness was halved from 60 to 30 min and BASDAI reduced from 6.1 to 3.6. Erythrocyte sedimentation rate and C-reactive protein had normalised (baseline: 1.8 mg/dl and 21 mm/h; week 26: 0.02 mg dl and 4 mm/h). Even the functional status slightly improved as shown by a reduction of the BASMI from 7 to 6 and BASFI from 6.6 to 5.2. The NSAID use could be reduced from 150 mg indometacin/day to 50 mg/day. According to the ASAS criteria the patient easily achieved an ASAS20 and nearly an ASAS50 response. Using the ASDAS C a reduction from 5.8 to 1.5 at week 26 underlines this improvement (figure 1).
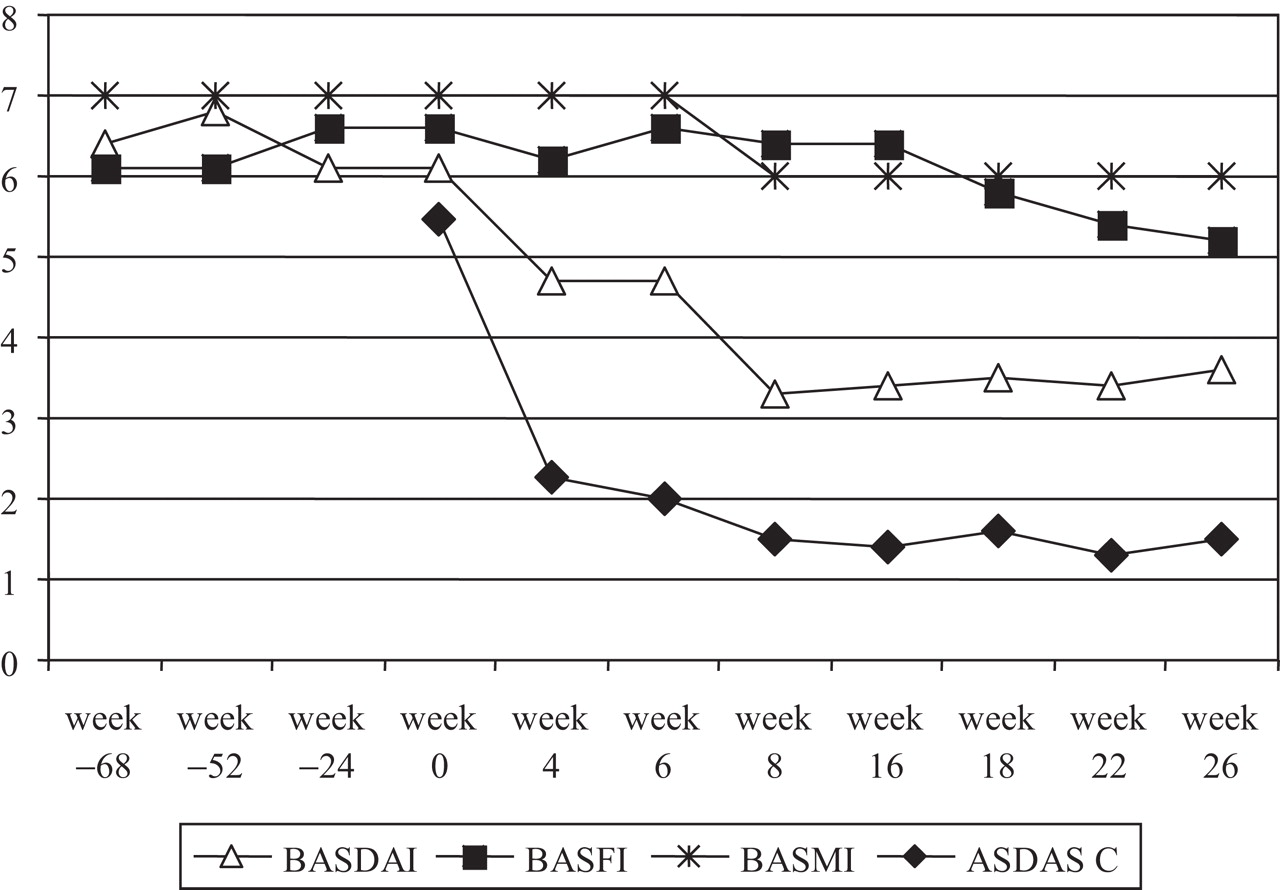
BASDAI, BASFI, BASMI and ASDAS C during anti-tumour necrosis factor treatment (week –68/–52) and TCZ treatment showing a reduction of disease activity only under TCZ. ASDAS C, Ankylosing Spondylitis Disease Activity Score; BASDAI, Bath Ankylosing Disease Activity Index; BASFI, Bath Ankylosing Spondylitis Functional Index; BASMI, Bath Ankylosing Spondylitis Metrology Index; TCZ, tocilizumab.
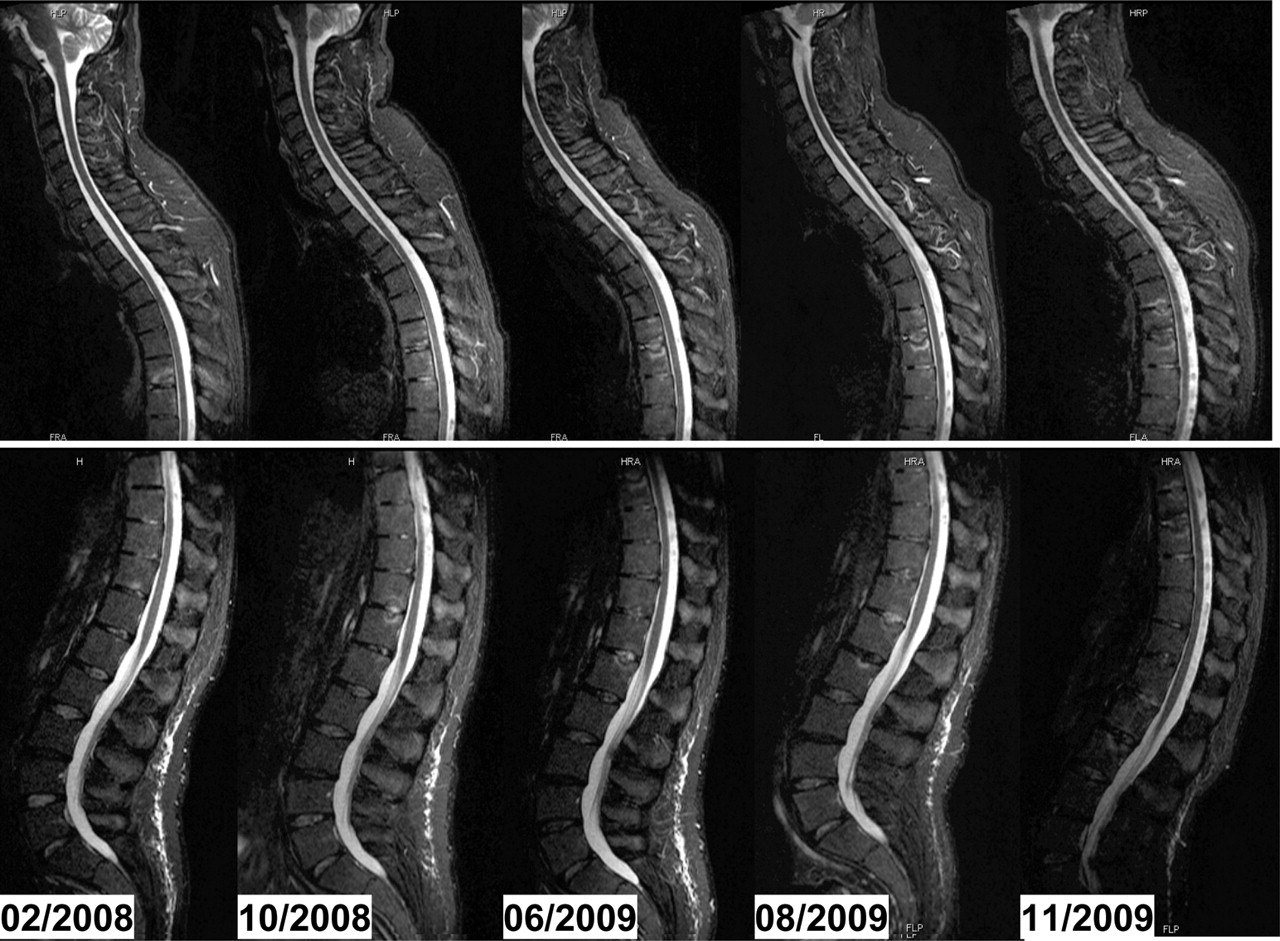
Despite the good clinical response, MRI of the spine did not improve over the 18-week follow-up, with persistent bone marrow oedema and new inflammatory lesions (figure 2). According to the Ankylosing Spondylitis Spine MRI-Score for acute changes,3 stable disease was assessed (score 13/12/14 in weeks 0, 6 and 18, respectively). TCZ was very well tolerated; cholesterol increased only little and remained stable (baseline: 180 mg/dl, week 18: 219 mg/dl).
{kind=link}
{kind=link}
MRI (fat-saturated short τ inversion recovery (STIR) sequences) of the whole spine during anti-tumour necrosis factor treatment (02/2008–05/2009) and with tocilizumab treatment (06/2009–11/2009) showing continuing inflammation during both treatment strategies. ASspiMRI-a-Score: 13/11/13/12/14. ASspiMRI-a-Score, Ankylosing Spondylitis Spine MRI-Score for acute changes.
This is the first report of treatment for AS with TCZ. Although MRI results did not improve, clinical and serological activity has considerably decreased. Up to now we have a follow-up period of 6 months with continuing response. Of course, the possibility of a placebo effect cannot be excluded, but is unlikely as there is a marked and lasting clinical response, which could not be achieved with three previous TNF antagonists. The patient had had persistent serological inflammation with severe back pain, morning stiffness and spondylitis documented by MRI. We decided to use TCZ in this recalcitrant case because of its known fast efficacy in rheumatoid arthritis4 and its intensive influence on acute phase reactants. As amyloidosis is one of the main factors influencing life expectancy in patients with AS, reduction of inflammation was one of the primary aims of the treatment. In a small cohort IL-6 was found to be increased in four of five patients with AS in biopsy samples from sacroiliac joints.5 For the alternative biological agents approved for other rheumatic diseases—namely, rituximab and abatacept, reports are controversial6 7 or no data are currently available.
The further course of inflammation visible on MRI remains to be awaited, possibly, improvement on MRI lags behind clinical and serological response. TCZ is a promising agent for the treatment of AS and inadequate response to TNF antagonists.
Footnotes
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Competing interests None.
-
Patient consent Obtained.