Article Text

Abstract
Objective The impact of gender on the response and tolerance to abatacept was assessed in a large prospective cohort during 2 years of follow-up.
Methods From the 1017 patients included in the Orencia and Rheumatoid Arthritis registry, disease activity was assessed at baseline, 6, 12 and 24 months. The relationship between the European League Against Rheumatism (EULAR) response, Disease Activity Score 28 (DAS28) remission, rate of adverse events and gender was explored in multivariate analysis.
Results 990 patients, 79.3%female, with at least one follow-up visit were analysed. At baseline, women had longer disease duration, higher disease activity and more often received antitumour necrosis factor (TNF) drugs. The remission was not different between men and women during the follow-up after adjustment on age, disease duration and activity, rheumatoid factor and anti-cyclic citrullinated pyeptide (CCP) positivity, and current disease-modifying antirheumatic drugs (DMARDs), previous TNF blockers and corticosteroids use. The proportion of men and women achieving EULAR good-or-moderate response at any endpoints was similar (52.4% vs 55.5%), as well as time to achieving EULAR response (5.4±4.9 vs 5.6±5.2 months). Moderate EULAR response was more frequent in women at 6 months (OR=1.80, p=0.02) but was no longer significant at 12 or 24 months. During the follow-up, the DAS28, the tender joint count score and the patient global assessment remained higher in women (p=0.001, 0.04 and 0.06, respectively). Drug retention and safety were comparable.
Conclusion In this large daily practice cohort of established rheumatoid arthritis treated with abatacept, women achieved similar remission and EULAR response than men despite higher disease activity and tender joint count during the treatment course.
- rheumatoid arthritis
- dmards (biologic)
- treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
More severe disease, worse functional outcome and less sustained remission in women raise the issue of gender-sensitive treatment strategies.
Treatment response to tumour necrosis factor blockers was found lower in women, conflicting data that were obtained with rituximab.
What does this study add?
This study assesses the impact of gender on the response and tolerance to abatacept treatment in current practice during 2 years of follow-up.
How might this impact on clinical practice?
In this large daily practice cohort of established rheumatoid arthritis treated with abatacept, women achieved similar remission and European League Against Rheumatism response than men despite higher disease activity and tender joint count during the treatment course.
Introduction
Sex and gender differences in rheumatoid arthritis (RA) are first supported by epidemiological evidence, women being affected three times more often than men,1 but are also reported in RA outcomes as well as in treatment responses. Biological factors, particularly hormones, may be the reason for the sex differences, with an inductive role of female hormones at the onset of the disease and a protective role of androgens. In addition, gender in a complex interplay with sex must be considered to explore differences in disease manifestations, outcome and management. Separating the influence of sex and gender is difficult as sex can modify behaviours, and gender behaviour can impact biological factors and thereby health. Gender differences associated with behaviour or lifestyle may include environmental or nutritional factors, and differences in the use of drugs.2 3 More severe disease, worse functional outcome and less sustained remission in women4–8 raise the issue of gender-sensitive treatment strategies. Data from the national biologics registers are useful to investigate differences between men and women in treatment response. Treatment response to tumour necrosis factor (TNF) blockers was found lower in women in the British and Danish registers.4 9 Conflicting data with rituximab have been obtained from the French and British registers.10 11 In patients from The Danish Registry for Biologic Therapies (DANBIO) registry treated with abatacept or tocilizumab,12 the sex was not a predictive factor for remission or drug survival, and no data beyond 6 months of follow-up have been published with abatacept in the French register.13
The Orencia and Rheumatoid Arthritis (ORA) is a French national registry founded in 2008 by the ‘Club Rhumatismes Inflammatoires’ and the ‘French Society of Rheumatology’ that records efficacy and safety data on patients with RA treated with abatacept.14 Therefore, from this large prospective observational cohort of patients with RA treated with abatacept in ‘real life’, we aimed to assess the impact of gender on the response and tolerance to treatment during 2 years of follow-up.
Methods
The ORA registry is a French nationwide, multicentre, prospective cohort study investigating the tolerance and efficacy of intravenous abatacept in patients treated for RA.13 The methodology of the registry has been previously reported.13 The registry was approved by the French authorities (‘Comité Consultatif sur le Traitement de l’information en matière de Recherche dans le domaine de la Santé’ and ‘Commission Nationale de l’Informatique et des Libertés’). All the patients gave informed consent for participation. This registry recruited adult patients receiving abatacept for RA from 82 centres between 2008 and 2010. Centres were informed that including patients in this observational registry would not interfere with their current practice or involve additional laboratory testing. Characteristics of the patients (age, gender, disease duration, swollen joint count (SJC), tender joint count (TJC), Visual Analogue Scale for patients’ global assessment), clinical Disease Activity Scores 28 (DAS28-ESR), biological parameters anti-cyclic citrullinated pyeptide (anti-CCP), rheumatoid factor, erthyrocyte sedimentation rate (ESR) and C reactive protein (CRP)), current DMARDs, previous TNF blockers, steroid use, and infections were recorded at baseline (at the time of the patient’s first exposure to the drug) and then every 6 months. The efficacy of abatacept was assessed by the remission rate, defined as a DAS28-ESR <2.6 and the percentage of European League Against Rheumatism (EULAR) responses (good, moderate, good or moderate versus non-response) according to the EULAR criteria during the follow-up (6, 12 and 24 months).
Statistical analysis
The statistical analysis was performed using Stata V.12 software. The primary outcome was the EULAR good-or-moderate response; exploratory analyses were performed for remission and retention rates. Tests were two-sided and a p value <5% was considered significant. The baseline characteristics of the study population were reported as mean (SD) or median and IQR according to statistical distribution for quantitative variables and as frequencies (associated percentages) for categorical parameters. Comparisons of these baseline characteristics between male and female patients were analysed using the χ2 (or Fisher’s exact test when necessary) for categorical variables and Student’s t-test (or Kruskal-Wallis test when normality assessed by the Shapiro-Wilk test was not verified). The relationship between the EULAR response, DAS28 remission, rate of adverse events (at 6, 12 and 24 months) and gender was explored in multivariate analysis using a random-effects model taking subject as random effect, with adjustment on age, disease duration, rheumatoid factor (RF) or anti-CCP positivity, current DMARDs or previous TNF blockers, corticoids use, and RA activity. Interaction between gender and time was tested. To avoid bias due to loss to follow-up, treatment discontinuation for inefficacy was considered as a non-response/non-remission for the visit and during the follow-up, and missing data (at 6, 12 and 24 months) were imputed using last observation carry forward. Results were expressed as the OR with 95% CI. We carried out analyses of treatment discontinuation (for adverse event and inefficacy) using survival methods to take into account the time to event. Longitudinal changes in the DAS score and its components were also analysed by random effects, taking subject as random effect and testing interaction between sex and time-point evaluation.
Results
Gender differences at baseline
Baseline comparisons between men and women are presented table 1. Among the 1017 patients enrolled in the ORA registry, 990 had at least one follow-up visit and were included in the analysis. Seven hundred and eighty-four were women (79.2%) with a mean age of 57.4±14.2 years. Women had longer disease duration (p<0.001) and higher disease activity (p<0.001) at baseline. Rheumatoid factor and anti-CCP positivity were observed in a similar way between women and men. Cardiovascular risk factors, smoking and extra-articular manifestations were more frequent in men. No differences for the use of DMARDs or steroids were observed, but women more often previously received TNF blockers (p=0.05).
Baseline characteristics of the 990 patients analysed
Efficacy of abatacept
Although men appeared to have better remission rate in univariate analyses, the DAS28 remission rate did not significantly differ between men and women during the follow-up after adjustment on age, disease duration, rheumatoid factor or anti-CCP positivity, current DMARDs, previous TNF blockers and glucocorticoids use, and disease activity (table 2).
Univariate and multivariate analyses of gender difference in abatacept response after 6, 12 and 24 months of follow-up
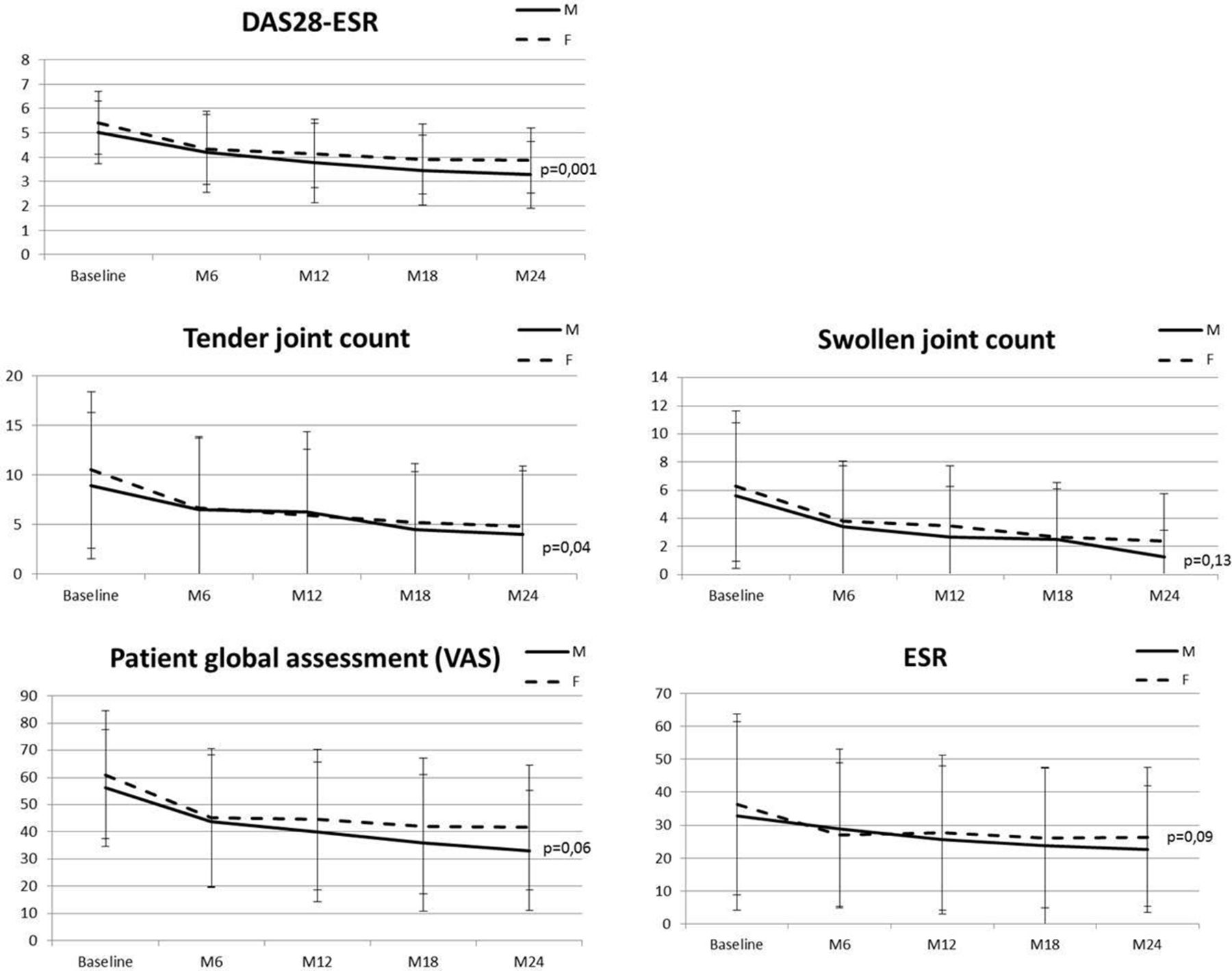
The proportion of patients achieving EULAR good-or-moderate response at any endpoints did not differ between men and women (52.4% vs 55.5%, p=0.42). Time to achieving EULAR good-or-moderate response was similar in women and men (5.4±4.9 vs 5.6±5.2 months, p=0.67). Moderate EULAR response was more frequent in women at 6 months but was no longer significant at 12 or 24 months (table 2). During the follow-up the DAS28-ESR (p=0.001), the TJC (p=0.04) and the patient global assessment (p=0.06) remained higher in women, whereas SJC and ESR did not differ between men and women at any endpoints (figure 1).
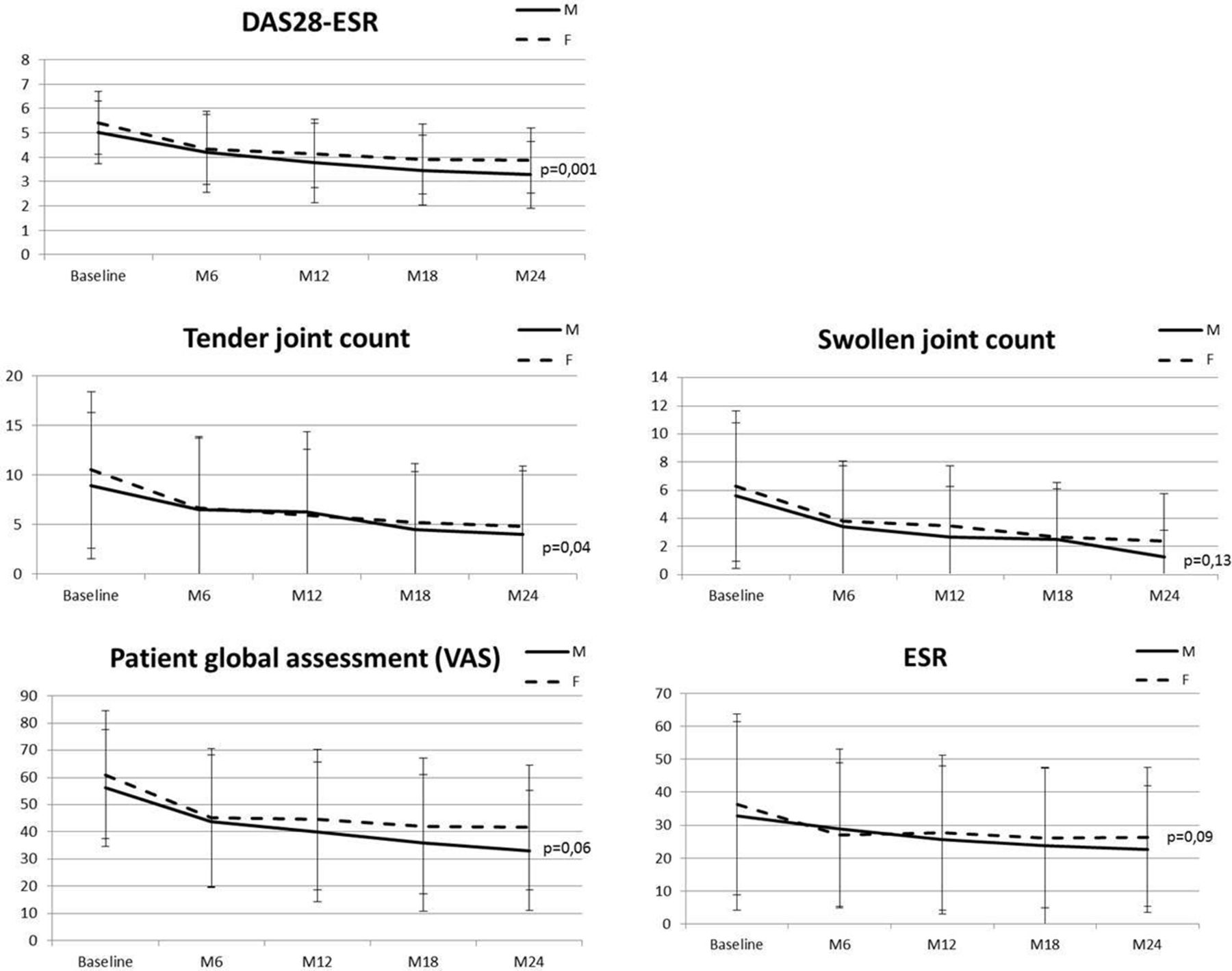
Change in DAS28-ESR score and components during treatment with abatacept stratified by sex. Each point represents a mean DAS score. Vertical bars represent SD. DAS28, Disease Activity Score 28; ESR, erythrocyte sedimentation rate; VAS, Visual Analogue Scale.
Drug retention rate and safety
Treatment with abatacept was maintained in 86.9%, 72.5% and 52.8% of men and 91.1%, 72.8% and 55.8% of women at the 6-month, 12-month and 24-month follow-up visits, respectively (figure 2). During the follow-up, 73.1% of women and 69.4% of men stopped the treatment at least one time (p=0.3), because of inefficacy in 69.1% of men and 64% of women (p=0.24), and adverse events in 14% and 15%, respectively (p=0.76). Serious infections occurred in the same way in men and women (5.5 vs 4.2/100 patient-years, p=0.3) during the 2 years of follow-up. Cancer occurred in 10 men and 17 women (2.4 vs 1.1/100 patient-years, p=0.06) and death in 4 men and 1 woman.

{kind=link}
{kind=link}
Retention rate of abatacept treatment stratified by sex (M, male; F, female).
Discussion
In this large study of patients with RA treated in real life with abatacept, we were not able to demonstrate any differences for remission rates or EULAR response during the 2 years of follow-up between men and women, except for the moderate EULAR response being better in women after 6 months of treatment. However, differences in disease expression between men and women were observed. Despite similar improvement in disease activity score with treatment, women had greater absolute activity at baseline and during follow-up, which may be explained by higher TJC. Thus, the only DAS28 component that significantly differed during the longitudinal analysis was the TJC. Previous studies in RA have shown higher disease activity in women as measured by the DAS28, TJC score and patient global assessment,15–17 contrasting with similar radiographical progression.4 16 Gender differences in pain perception and assessment reported in RA as well as in spondyloarthritis18 19 may explain this dissociation.
Gender was further analysed as a predictor of remission in several studies. Remission rates were found lower in women whether patients received conventional DMARDs or biologics.4 10 20–23 Thus, in an observational study including 142 patients with recent-onset RA treated with DMARDs, remission was more frequently achieved in men than in women after 5 years of follow-up.20 The Swedish Better Anti-Rheumatic FarmacoTherapy (BARFOT) cohort including 698 patients with early RA reported similar findings after 2 and 5 years of treatment, mainly with conventional DMARDs.8 15 In long-standing RA from the British Society for Rheumatology Biologics Register, remission with TNF blockers was achieved less frequently for women, but EULAR response did not differ.9 Similar results were observed with rituximab in the French registry after 2 years of follow-up,10 and less improvement in DAS28 after 6 months of follow-up was noted in the British registry.11 Interestingly, the gender difference for the response to biologics seems to be focused on the remission as defined by the absolute DAS28 score and also depends on the disease duration. Poorer response with TNF blockers was observed in women only in early RA during the 4 years of follow-up, whereas no difference was observed after adjustment on disease duration and disease activity in established RA of more than 2 years’ duration.4 As observed with TNF blockers, we noted that the gender difference for the remission rates in established RA treated with abatacept did not persist when adjusted for disease activity and disease duration higher in women.
Several limitations of our study should be noted. First, we could not analyse the severity of the disease, notably the functional impairment and disability status as the Health Assessment Questionnaire (HAQ) and radiographs were not available in the ORA registry. As it is an observational study reflecting routine clinical practice, missing data for some variables is another possible limitation of our analysis.
In conclusion, in this large daily practice cohort of patients with established RA treated with abatacept, women achieved similar remission and EULAR response than men despite higher disease activity and TJC score during the treatment course. Drug retention rate and safety were comparable between the two genders. Gender differences for treatment response and remission should now be focused on in early RA.
Acknowledgments
We thank Euraxi Pharma for the help of their clinical research associates and all the investigators of the ORA registry, the French Society of Rheumatology, E Boccard (BMS), the 14 research study nurses (A Bourgeois, E Braychenko, F Carmet, MH Da Silva, S Delmas, D Guinement, R Lefebure, C Lehning, N Minot, FMA Ouattara, V Pinosa, M Reau, H Thibault and E Wallet), and L Dongmo and V Martin (Euraxi Pharma) for their contributions.
This work was presented at conferences and published as a conference abstract: EULAR 2015, French Congress of Rheumatology 2015.
References
Footnotes
Funding No specific funding was received from any funding bodies in the public, commercial or not-for-profit sectors to carry out the work described in this manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The registry was approved by the French authorities (’Comité Consultatif sur le Traitement de l’information en matière de Recherche dans le domaine de la Santé' (CCTIRS) and ’Commission Nationale de l’Informatique et des Libertés' (CNIL)). The ethical committees of all participating centres approved the ORA registry.
Provenance and peer review Not commissioned; externally peer reviewed.