Article Text

Abstract
Objective To determine the duration of clinical benefit among patients with psoriatic arthritis (PsA) discontinuing tumour necrosis factor inhibitor (TNFi) therapy while in low disease activity (LDA), and to identify patient characteristics associated with prolonged clinical benefit.
Methods We performed an observational cohort study assessing patients with PsA from the Consortium of Rheumatology Researchers of North America (CORRONA) registry who had discontinued TNFi after achieving LDA, defined as clinical disease activity index (CDAI) score ≤10 and physician's global assessment (PGA) of skin psoriasis ≤20/100. Kaplan–Meier method was used to estimate the duration of clinical benefit.
Results Of the 5945 patients with PsA in CORRONA, 302 patients had discontinued TNFi (n=325) while in LDA and had follow-up data available. At time of discontinuation, mean PsA duration was 9.8 years, mean CDAI was 3.9, and mean duration of TNFi use was 1.5 years; 52.6% of patients had discontinued their first TNFi. Median time to loss of benefit was 29.2 months. 179 (55.1%) patients had persistent benefit at their previous clinic visit. An increased risk of losing clinical benefit was seen among patients with higher disease activity at discontinuation (CDAI≥3.2 vs <3.2; HR 1.43 (p=0.32)) and among smokers (HR 1.78 (p=0.027)).
Conclusions Patients with PsA who achieve LDA may maintain clinical benefit after discontinuation of TNFi therapy.
- Psoriatic Arthritis
- Anti-TNF
- Disease Activity
- Treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
There is a paucity of data addressing withdrawal of biological therapy in psoriatic arthritis (PsA). Whether tumour necrosis factor inhibitor (TNFi) can be withdrawn in PsA in patients who have achieved low disease activity (LDA) or remission with sustained clinical benefit remains unknown.
What does this study add?
This study provides evidence that some patients with PsA achieving LDA may maintain clinical benefit after discontinuation of TNFi therapy.
How might this impact on clinical practice?
It may be possible to discontinue TNFi therapy after achieving LDA, while maintaining sustained clinical benefit. This could have important treatment implications, particularly in light of the heavy economic burden and potentially serious adverse effects that may be associated with TNFi.
Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory disease with heterogeneous clinical manifestations. Tumour necrosis factor inhibitors (TNFi) effectively treat all domains of disease activity in PsA.1 Aggressive treatment strategies, particularly involving the use of TNFi, have revolutionised the treatment of PsA resulting in low disease activity (LDA) and remission becoming viable treatment goals.2 ,3 Indeed, intensive treatment strategies in early disease have been shown to result in better clinical outcomes in PsA.4
Owing to factors such as economic burden, concern for drug toxicity, and patient preferences, there has been increasing interest in the possibility that TNFi treatment may be reduced or discontinued in patients achieving remission or LDA, with maintenance of clinical benefits. There is some evidence for discontinuation of biological therapies in rheumatoid arthritis (RA) with persistent clinical benefit.5 ,6 Whether TNFi can be withdrawn in PsA with sustained clinical benefit remains unknown.
The objectives of this study were to determine the duration of sustained clinical benefit among patients with PsA who had discontinued TNFi while in LDA, and also to identify patient characteristics and disease-related factors that may be associated with prolonged clinical benefit after TNFi discontinuation.
Patients and methods
The Consortium of Rheumatology Researchers of North America (CORRONA) registry is a large, independent, multisite, prospective observational cohort of patients with RA and PsA.7 We assessed patients with physician-diagnosed PsA from 2008 to 2013 who had discontinued TNFi after achieving LDA. Of the 5945 patients with PsA in the CORRONA registry, there were a total of 496 TNFi discontinuations in LDA. We identified 302 eligible patients with PsA, who had: discontinued TNFi (n=325) while in LDA; did not have an escalation of therapy; and had follow-up data available for analysis. Patients were excluded if, at time of discontinuation, they had a switch or addition of any biological or non-biological disease-modifying antirheumatic drug (DMARD) (n=53) or if they had an increase in dose of concomitant non-biological DMARD or prednisone at time of TNFi discontinuation (n=93). There were 25 patients who had no follow-up visit after TNFi discontinuation. The decision to discontinue therapy was made individually by the patients and their treating physicians; there was no prespecified protocol for discontinuation of therapy. All patients in the CORRONA registry provided written, informed consent for participation in this study.
LDA was defined as clinical disease activity index (CDAI) ≤10 and physician's global assessment (PGA) of skin psoriasis ≤20/100. Patients were considered to have lost clinical benefit if they had: (1) an increase in CDAI to >10; (2) an increase in skin assessment to >20; or (3) escalation of therapy with either an increase in concomitant DMARD or prednisone doses, or initiation of prednisone, non-biological DMARD, or biological agent. Clinical data were collected at baseline (ie, time of TNFi discontinuation) and at loss of clinical benefit or the previous clinic visit. The CDAI used in the CORRONA registry is based on a 28-joint count. Skin assessment was based on physician global skin disease activity (100 mm visual analogue scale (VAS).
Statistical analyses
Descriptive statistics are presented as means±SD for continuous variables, and frequency and percentages for categorical variables. p Values <0.05 were considered statistically significant. Kaplan-Meier method was used to estimate the median time to loss of clinical benefit. Both univariable and multivariable Cox proportional hazard analyses were used to evaluate characteristics associated with duration of clinical benefit. Factors that were significant at the 20% level (p value <0.20) in the univariable analysis were further evaluated in the multivariable model.
Results
Of the 5945 patients with PsA in the CORRONA database, there were 325 discontinuations of TNFi therapy while in LDA in 302 patients who had follow-up data available. The mean age was 52.6±13.1 years, 51.9% were women, and mean body mass index (BMI) was 30.1±6.5 (table 1). At discontinuation, the mean duration of PsA was 9.8±8.1 years, mean CDAI was 3.9±2.8, mean modified disease activity score (mDAS) was 2.4±0.6, and PGA of skin psoriasis was 6.7±6.1%.
Population characteristics at time of TNFi discontinuation (N=325)
Among the patients assessed, 52.6% of patients had discontinued their first TNFi and 31.1% had discontinued their second TNFi. The mean duration of TNFi use prior to discontinuation was 1.5±1.6 years. Concomitant medications at the time of TNFi discontinuation were recorded: 53.5% of patients were treated with TNFi monotherapy, 42.2% were on background methotrexate (MTX); and 5.2% took concomitant low-dose prednisone.
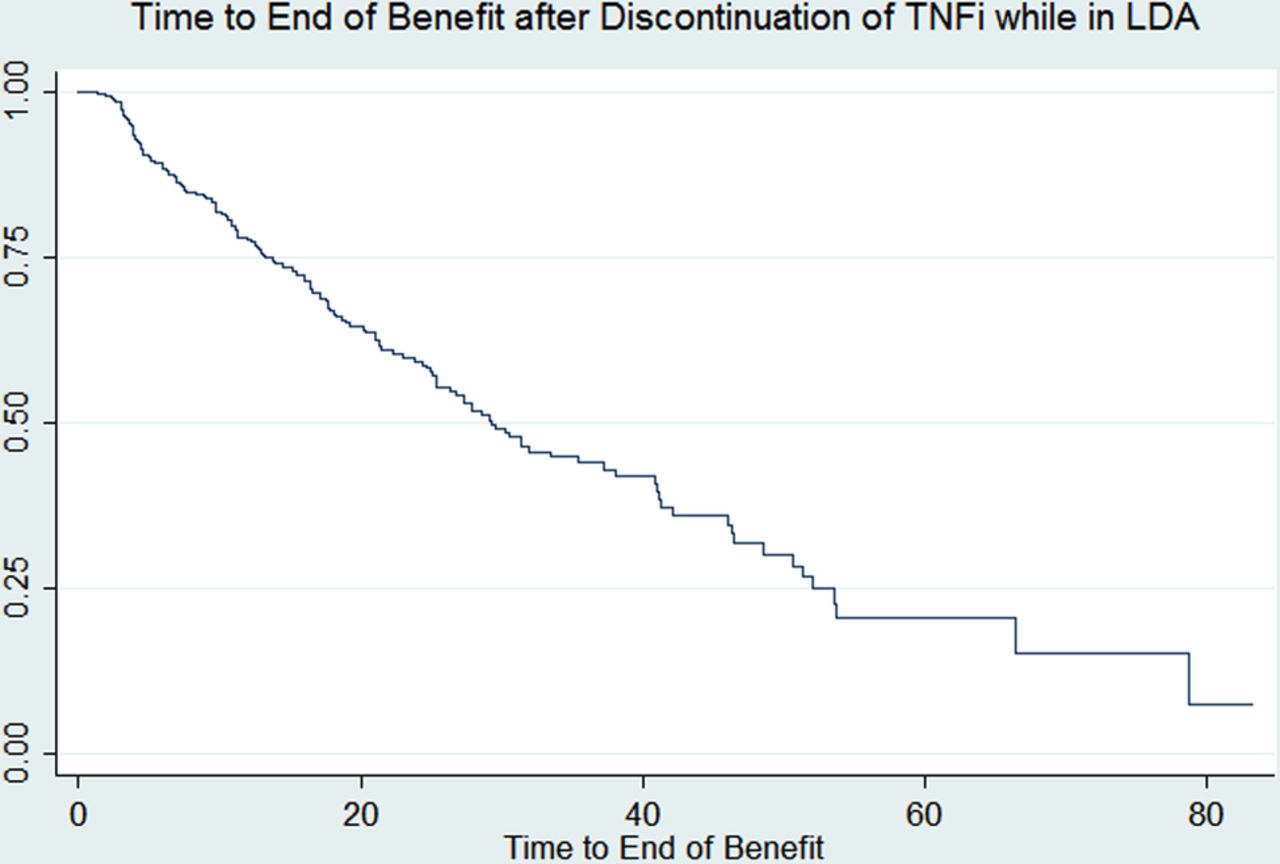
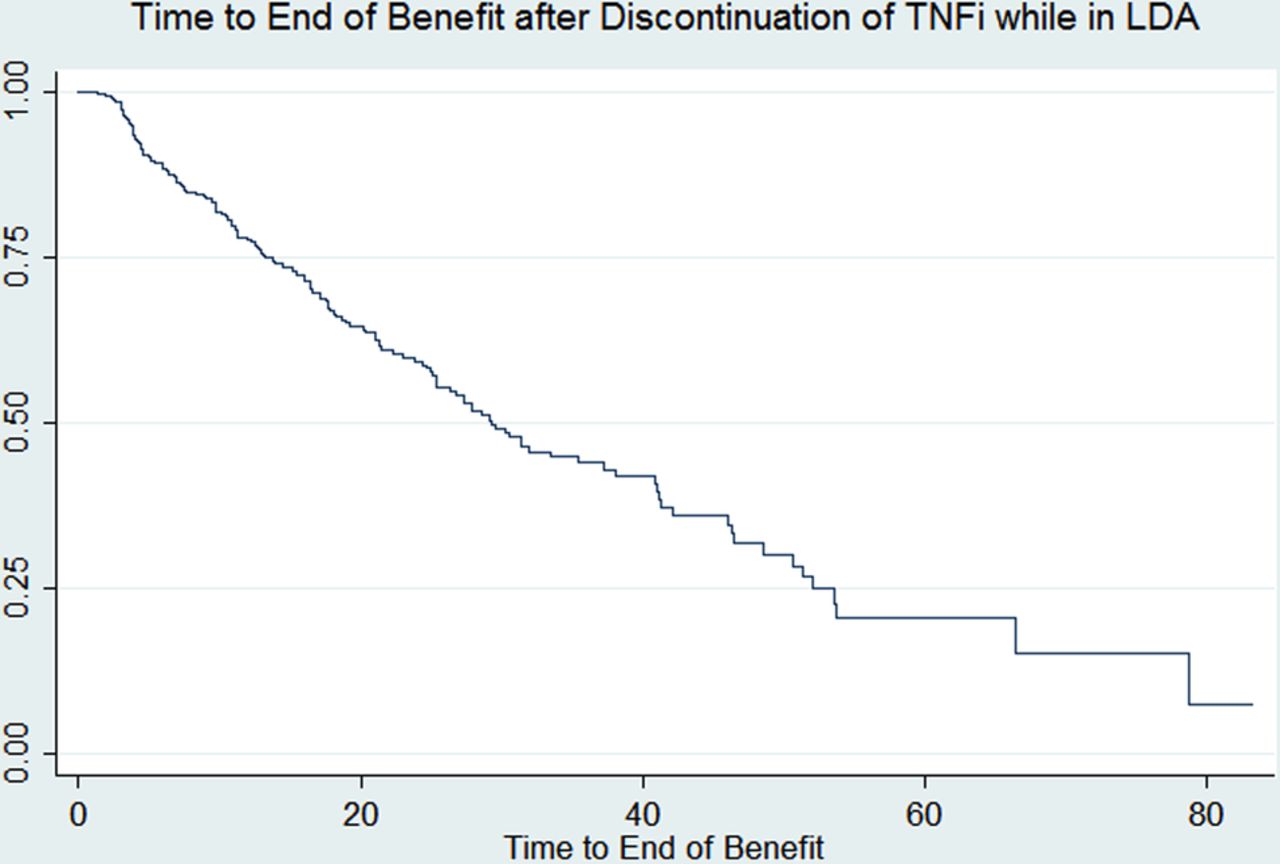
After withdrawal of TNFi treatment, 146 (44.9%) patients lost clinical benefit due to: increased CDAI (31.5%); worsening skin disease (15.8%); non-biological DMARD initiation or dose escalation (32.2%); TNFi initiation or restart (6.8%); or prednisone initiation or dose escalation (9.6%) (table 2). Kaplan–Meier survival estimate of median time to loss of clinical benefit was 29.2 months (figure 1). At last clinic visit, 179 (55.1%) patients had persistent clinical benefit off TNFi therapy.
Distribution of events among patients with loss of clinical benefit (N=146)
{kind=link}
Kaplan–Meier survival curve showing time to loss of clinical benefit after TNFi discontinuation (N=325). LDA, low disease activity; TNFi, tumour necrosis factor inhibitor.
Patients with higher disease activity at the time of TNFi discontinuation had increased risk of losing clinical benefit HR: CDAI ≥3.2 versus <3.2, HR 1.43 (p=0.032); moderate versus low mDAS, HR 1.65 (p=0.017); patient global assessment >5 versus <5/10, HR 1.7 (p=0.007) (table 3). Current smokers had significantly higher risk for loss of clinical benefit (smokers versus non-smokers), HR 1.78 (p=0.027) in univariable and multivariable analysis. In the multivariable model, current smoking was associated with higher risk of losing clinical benefit HR 1.76, 95% CI (1.13 to 2.27) while CDAI >3.2 versus <3.2 also appeared to convey increased risk for loss of clinical benefit HR 1.42 (0.99 to 2.03). Age and gender did not alter this risk in the multivariable model. The number of prior TNFi used and overweight or obese status did not significantly affect loss of clinical benefit in our cohort.
Univariable Cox proportional hazard analysis of factors related to loss of clinical benefit after TNFi discontinuation (n=325) while in LDA
Discussion
Advances in highly effective therapies have led to improved clinical outcomes in PsA, making LDA and remission achievable goals. Since TNFi are associated with both a high financial burden and an increased risk of potentially life-threatening adverse events, the need for maintenance therapy with these biological agents has been challenged. As a result, there is increasing interest into whether TNFi could be reduced or discontinued while maintaining clinical benefit in patients with PsA who have achieved good clinical outcomes on these medications.
There is a paucity of data looking at tapering strategies—through either dose reduction or drug discontinuation—for TNFi in PsA, and the results are not straightforward. In a single-centre, prospective study of the 76 patients with PsA treated with adalimumab, 88.6% of patients maintained remission after halving the dose of TNFi therapy over a follow-up period of 28.9 months.8 Thus sustained remission through decreasing the dose of TNFi appears possible. The results with drug discontinuation are less certain. In a small study of 26 patients, stopping conventional and biological DMARDs resulted in a high incidence of early disease recurrence (76.9%), suggesting that drug-free remission was not possible.9 In contrast, a prospective study of 236 patients with PsA with peripheral joint involvement, showed that remission was possible in 24% of patients after the interruption of therapy and was significantly more common in patients who received TNFi than traditional DMARDs.10 It should be noted that relapse did occur in 49% of patients after 12±2.4 months of treatment discontinuation, although these patients were not maintained on non-biological DMARDs.
Data from our cohort suggests TNFi discontinuation in patients with PsA with LDA can be associated with sustained clinical benefit (median 29.2 months). While 146 (44.9%) patients lost clinical benefit, only 10 (6.8%) were restarted on TNFi, while the others were managed with non-biological DMARDs and prednisone. Thus, this strategy could have a significant impact on decreasing the economic burden and limiting the risks associated with prolonged TNFi exposure.
Predictors of sustained remission after TNFi discontinuation have not yet been confirmed.11 It looks from our cohort that smokers and patients with worse disease activity at the time of discontinuation of TNFi fare worse. In contrast, disease duration, the number of prior TNFi used, and BMI did not seem to affect the outcome. Further studies will be required to identify predictors of prolonged remission after discontinuation of TNFi.
A potential limitation of our study is that the reason for discontinuation of TNFi in the study population is not known. We excluded patients who had any escalation of therapy (ie, switch or addition of any other biological or non-biological DMARD, or increase in dose of concomitant non-biological DMARD or prednisone) at the time of discontinuation, but we cannot account for reasons for discontinuation other than LDA (eg, adverse events, financial burden, etc). A second limitation of this study is our use of CDAI with a 28-joint count. The CDAI is a composite disease activity index developed for RA, but frequently extrapolated to and validated in PsA; however, it does not include the ankles and feet, which are commonly affected in PsA.
In summary, patients with PsA who achieve LDA on treatment may maintain persistent clinical benefit after the discontinuation of TNFi. Patients with higher disease activity at the time of discontinuation and smokers may have less success at stopping TNFi therapy. Whether biological therapy can be reduced or discontinued in the long term requires further study in controlled withdrawal trials.
Footnotes
Funding This study was funded by Corrona, LLC.
Competing interests None declared.
Ethics approval IRB.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.