

Abstract
Objective. Juvenile idiopathic arthritis (JIA) may result in disability, which is caused primarily by degeneration of the osteocartilaginous structures, due to the synovial inflammatory process. It is essential to closely monitor structural damage during the disease course. We aimed to compare ultrasound (US) measurements of joint cartilage thickness in 5 joints in children with JIA to our findings in an age- and sex-related healthy cohort regarding disease duration, joint activity, JIA subtype, age, and sex.
Methods. We clinically examined joint activity in 95 patients with JIA and collected parent and physician global assessments. Joint cartilage thickness was assessed by greyscale US in knee, ankle, wrist, metacarpophalangeal, and proximal interphalangeal (PIP) joints. Measurements were compared to reference values of a healthy cohort from a previous study. Medical records were reviewed for JIA subtype, treatment, and disease duration.
Results. Joint cartilage thickness was decreased in the knee, wrist, and second PIP joint in children with JIA compared with the healthy cohort (p < 0.001 for all). Patients with oligoarticular JIA had thicker cartilage than patients with polyarticular and systemic JIA. We also found decreased joint cartilage thickness in joints not previously affected by arthritis in children with JIA compared to the same joint in the healthy cohort. We found decreasing cartilage thickness with age and thicker cartilage in boys than in girls.
Conclusion. Children with JIA have reduced cartilage thickness compared with children who do not have JIA, and children with polyarticular and systemic JIA have thinner cartilage than children with oligoarticular JIA.
Juvenile idiopathic arthritis (JIA) is the most common rheumatic disease in childhood; it can result in musculoskeletal pain, joint stiffness, and joint swelling, leading to disability. Functional disability in JIA is primarily caused by degeneration of the osteocartilaginous structures, due to the chronic inflammatory process in the synovium1. To evaluate therapeutic efficacy, it is therefore essential to closely monitor structural damage during the disease course.
Over the past decade, musculoskeletal ultrasound (US) has become an established diagnostic method in adult rheumatology2,3, and within recent years it has been used increasingly often in pediatric rheumatology4. US is of particular benefit in the assessment of early signs of arthritis, such as joint effusion and synovial thickening5. Using the color Doppler or power Doppler technique, it is possible to detect hyperemia in the synovial microcirculation as a part of the inflammatory changes in the joint; these changes cannot be observed by magnetic resonance imaging (MRI) unless contrast is used6,7. Further, US-guided joint injections have improved the accuracy of intraarticular corticosteroid injection (IACI) treatment8,9. US is also relatively inexpensive, does not require radiation, is well accepted even by small children, can be viewed at bedside, and enables the physician to view different anatomic locations in the same session10.
High-frequency US can be used to easily visualize the joint cartilage as an anechoic structure, because cartilage has high water content. In previous studies, we validated the assessment of joint cartilage thickness by US in a pediatric setting. We found a low intraobserver and interobserver variability11 and a good level of agreement, with no significant systematic joint size-related differences in cartilage thickness measurements between MRI and US12. Based on a large cohort of healthy children aged 7–16 years, we established age-related and sex-related normal reference values for cartilage thickness of the knee, ankle, wrist, second metacarpophalangeal (MCP), and second proximal interphalangeal (PIP) joints13. Our aim was to assess the cartilage thickness of selected large and small joints in children with JIA with regard to subtypes, disease duration, and disease activity, and to compare these measurements with age-related and sex-related healthy reference intervals.
MATERIALS AND METHODS
Children diagnosed with JIA according to the 2001 revised International League of Associations for Rheumatology classification14 aged 5–15 years and followed at the pediatric rheumatologic department at Aarhus University Hospital Skejby, Denmark, were invited to participate in the study. Inclusion criteria were systemic JIA, persistent and extended oligoarticular JIA, and rheumatoid factor (RF)-positive or RF-negative polyarticular JIA. Informed consent was received from the parents. Patients were excluded if they had received IACI within 1 month prior to examination or had a history of previous joint surgery. The study was approved by the local ethics committee.
We invited 155 patients to participate in the project at least 1 month prior to the examination date. The US examinations were performed on the same day as the clinical examination. Healthy children (n = 394) examined in a previous study served as a control group13. Demographic data are given in Table 1.
Demographic data of study population. Estimates are given as median (interquartile range) unless otherwise stated.
Duration of disease was determined by reviewing the patients’ medical records. Disease onset was defined as the first sign of disease activity confirmed by a physician. We divided the children into 3 subgroups of disease duration: (1) 0–12 months, (2) 13–60 months, and (3) 61–191 months. Further, we counted the number of IACI administered in each joint and recorded the time since the last injection. We compared affected versus contralateral unaffected joints within the same patient, enabling paired comparison of anatomically similar joints. Joint activity was assessed on the same day as US examination by an experienced pediatric rheumatologist and was defined as swelling within a joint, or limitation in the range of joint movement with joint pain or tenderness. The number of affected joints at any time during the disease course was recorded. In each patient with JIA, we established a juvenile arthritis disease activity score (JADAS) consisting of the active joint count of the 10 joints that were scanned by US, erythrocyte sedimentation rate, parent’s global assessment, and physician’s global assessment15.
US examination
A Hitachi EUB 7500 scanner with a 6–14 MHz linear transducer (EUP-L65) was used for the US measurements. All US examinations were performed by the same observer throughout the study (DØP). The patients were examined as described, using the same US settings [European League Against Rheumatism (EULAR) standards] described in a healthy age-matched and sex-matched cohort11,12,13. This ensured consensus with respect to the measurements of cartilage thickness. The clinical examination was done by an investigator other than the one who did the US measurements. The US scans were performed with the observer blinded to the clinical information regarding JIA subtype, arthritis activity, disease duration, and treatment. The images were saved and stored anonymously on a hard drive using a 9-digit code; thus, the cartilage thickness measurements were done with the investigators blinded with respect to age, sex, and disease activity status. The pressure of the probe was adjusted to a level just below visible deformation on the anatomical structure. We did greyscale examinations of distal femoral cartilage (knee joint), anterior talar cartilage (ankle joint), proximal dorsal scaphoid bone cartilage (wrist joint), distal second metacarpal cartilage (second MCP joint), and distal cartilage of the second proximal interphalangeal bone (second PIP joint). Outcome measures were cartilage thickness in mm. All examinations were measured perpendicular to the bone surface and without the “white band,” which marks the change in tissue density16. This was done to compare measures with the previous study13, in which the white band was not included. Our experience is that the thickness of the white band is 0.2 mm with few outliers (range 0.1–0.3 mm, unpublished data).
Standard scans of hyaline cartilage thickness are based on the guidelines recommended by EULAR17.
Knee joint
The child was placed in a supine position and a suprapatellar transverse scan was done with the knee in maximal flexion. Cartilage thickness was measured perpendicular to the midline of the intercondylar notch.
Ankle joint
The child remained in a supine position, with the plantar surface of the foot placed on the surface of the examination bed, with the knee in 90° flexion. The probe was placed longitudinally across the tibiotalar joint space between the first and second metatarsal bone. The anterior demarcation of the cartilage on the medial part of the dome of talus was identified. From this point, a distance of 5 mm in a proximal direction was measured out, and the cartilage thickness was measured perpendicular to the bone surface.
Wrist
This measurement was done with the child in a supine position and the arm lying alongside the body with the wrist stretched. The wrist cartilage thickness was measured on a dorsal longitudinal scan of the articulation surface of the radial and scaphoid bones.
Second MCP and second PIP joints
Cartilage thickness measurements of the second MCP and second PIP joints were obtained with a longitudinal scan of the dorsal second MCP and second PIP joints with the joints in 90° flexion. Cartilage thickness was measured in the midline perpendicular to the bone surface.
All measurements of cartilage thickness were made twice. The average thickness of each joint was used in the calculations.
Statistics
Comparisons of cartilage thickness within and between groups were done by linear regression controlled for age and sex and adjusted for clustered data (right/left extremities), because we know from our previous study that cartilage thickness decreases with age and that boys have thicker cartilage than girls. Data from the knee, ankle, and PIP joints were normally distributed, whereas data from the wrist and MCP joints were mildly skewed. We transformed all data to a logistic scale, which improved the wrist and MCP data but skewed the others. P values did not change regardless of transformed data, so we analyzed all cartilage thickness data as though it were normally distributed. We used the Stata 11 software package (StataCorp LP). Measurements of cartilage thickness are given as means (± SD), and comparisons are given as estimated differences with 95% CI. Further, we calculated z-scores of each joint compared to a healthy reference value for sex and age. The z-scores are presented as boxplots.
Paired t-test was used when comparing involved versus noninvolved joints within the same patient. P ≤ 0.05 was considered to be statistically significant.
RESULTS
Of the 155 children with JIA aged between 5 and 15 years who were invited to participate in the study, 52 patients declined, 3 had unclassified arthritis, and 5 canceled their scheduled examination because of illness. As a result, we included 95 children in the study. The median age was 11.3 years (range 5–15 years), with 68 girls and 27 boys. The demographic and anthropometric data are described in Table 1. The distribution of sex varied among the subtypes of JIA, whereas we found no significant variation in child age, height, and weight among the subtypes. The JIA cohort included 14 systemic, 8 RF-positive, and 23 RF-negative patients with polyarticular JIA, and 18 patients with extended and 32 with persistent oligoarticular JIA.
In total, we investigated 942 joints with US: 187 knee joints, 188 ankle joints, 188 wrist joints, 189 second MCP joints, and 190 second PIP joints. The 3 missing knee joints, 1 of the missing ankle joints, and the single missing second PIP joint were lost because of mistakes saving data. The last missing ankle joint and the 2 missing wrist joints were lost because of poor image quality. From a previous study, 394 healthy schoolchildren aged 6–16 years, 215 boys and 179 girls, served as a control group13. Thus, the JIA cohort and the healthy control group were comparable in age, height, and weight but not in sex distribution (Table 1).
When age was controlled for, the mean cartilage thickness of the joints investigated was significantly greater in boys than in girls, except for the second PIP joints. In all joints, cartilage thickness decreased with increasing age regardless of sex.
JIA versus controls: comparison of subtypes
Controlling for age and sex, the mean cartilage thickness measured in the total JIA cohort was significantly lower in the knee, wrist, and second PIP joints compared with the healthy control group (Table 2). Comparing the subtypes of JIA, we found that the mean cartilage thickness measured in the knee was significantly decreased in patients with polyarticular (p = 0.03) and systemic (p = 0.02) JIA compared to the oligoarticular subgroup (Figure 1). For the ankle, wrist, second MCP, and second PIP, we found no significant differences in mean cartilage thickness among the various subtypes, although there was a tendency toward decreased cartilage thickness in children with RF-positive polyarticular JIA compared to the other subtypes. Z-scores for each subtype confirmed that cartilage thickness was decreased in children with JIA compared to healthy children in the knee, wrist, and second PIP joints (Figure 2).

Boxplots show cartilage thickness of 5 joints in 4 juvenile idiopathic arthritis subtypes and an age-matched and sex-matched healthy cohort. Lines in boxes denote median, and whiskers are 5th and 95th percentile. MCP: metacarpophalangeal; PIP: proximal interphalangeal; Oligo: oligoarticular; Poly: polyarticular; RF: rheumatoid factor.
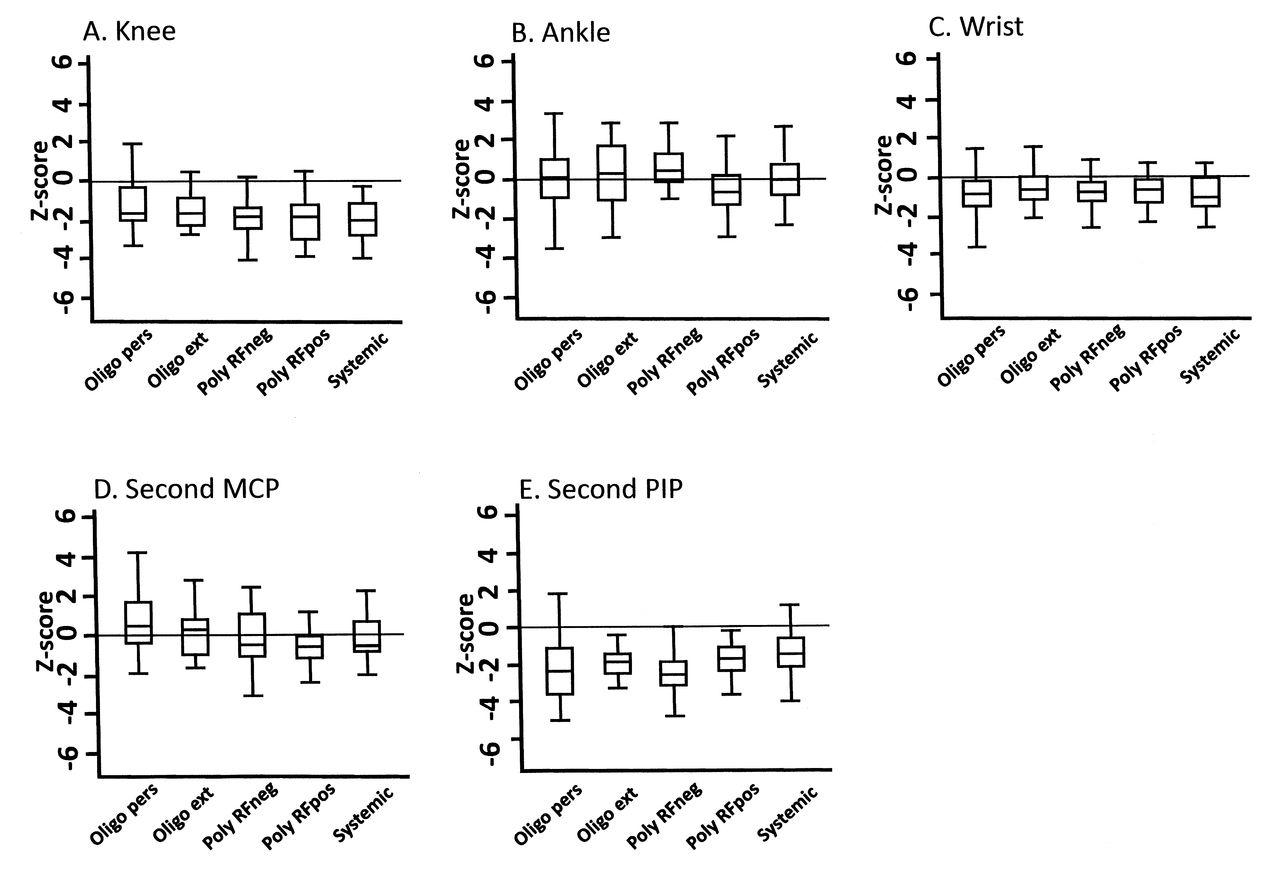
Z-scores for cartilage thickness in 5 joints. Horizontal lines represent healthy age-matched and sex-matched reference values. MCP: metacarpophalangeal; PIP: proximal interphalangeal; Oligo: oligoarticular; Poly: polyarticular; RF: rheumatoid factor; pers: persistent; ext: extended.
Measurements of joint cartilage in 5 joints. Patients with juvenile idiopathic arthritis (JIA) are compared to healthy controls. Values are in mm.
Previously affected versus unaffected joints
We compared joints with no previous history of active arthritis to those with previous arthritis involvement within the same patient. Although the mean cartilage thickness in affected knee, MCP, and PIP was slightly decreased, the difference was not statistically significant (Table 3). When we compared patients with JIA who had neither or both joints involved to the healthy cohort, we found significantly thicker cartilage in the healthy children in the knee, wrist, and PIP joints. In all joints not previously affected in patients with JIA, we still measured lower cartilage thickness in the knee (p < 0.001), wrist (p = 0.003), and second PIP (p < 0.001) joints, but not in the ankle or second MCP joint, compared to healthy controls (data not shown).
Difference in cartilage thickness between affected and unaffected joints within the same patient with juvenile idiopathic arthritis. Measures in mm are given as mean (± SD) unless otherwise stated.
Intraarticular corticosteroid injection
Eighty-one percent of the patients had been administered IACI at least once throughout the history of their JIA. In the knee, ankle, and wrists, the steroid injections were repeated up to 11, 8, and 7 times, respectively (Figure 3). Multiple IACI in the knee, ankle, or wrist did not appear to change the mean cartilage thickness. Because of the small number of patients who received IACI in the second MCP and second PIP joints, these results were not included. Time since last steroid injection in a specific joint did not show any correlation with cartilage thickness when we controlled for age, sex, and adjustment of clustered data (Figure 4).
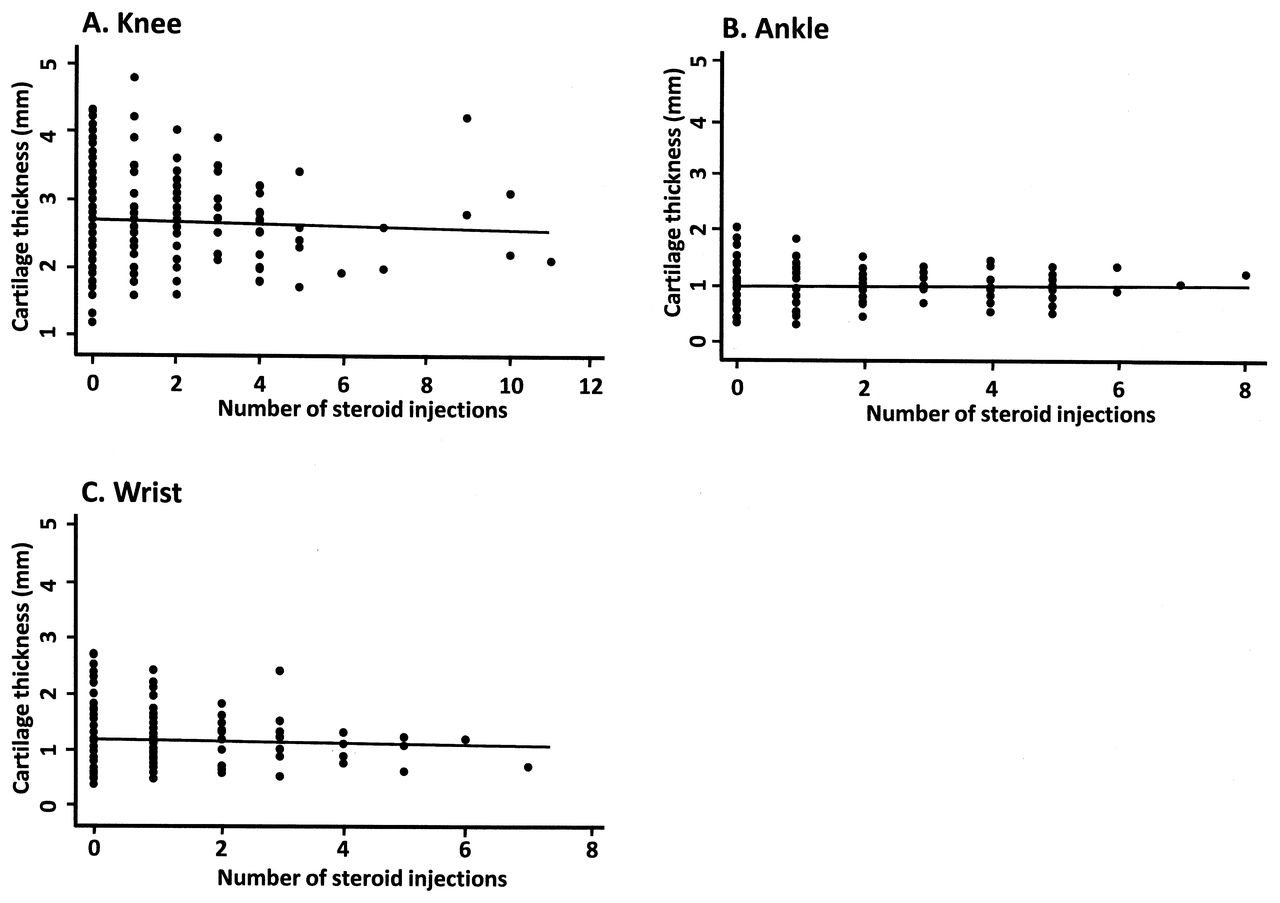
Number of intraarticular corticosteroid injections correlated to joint cartilage thickness in 3 joints. Second MCP and second PIP joints had too few values to plot. Lines represent fitted values for correlation.
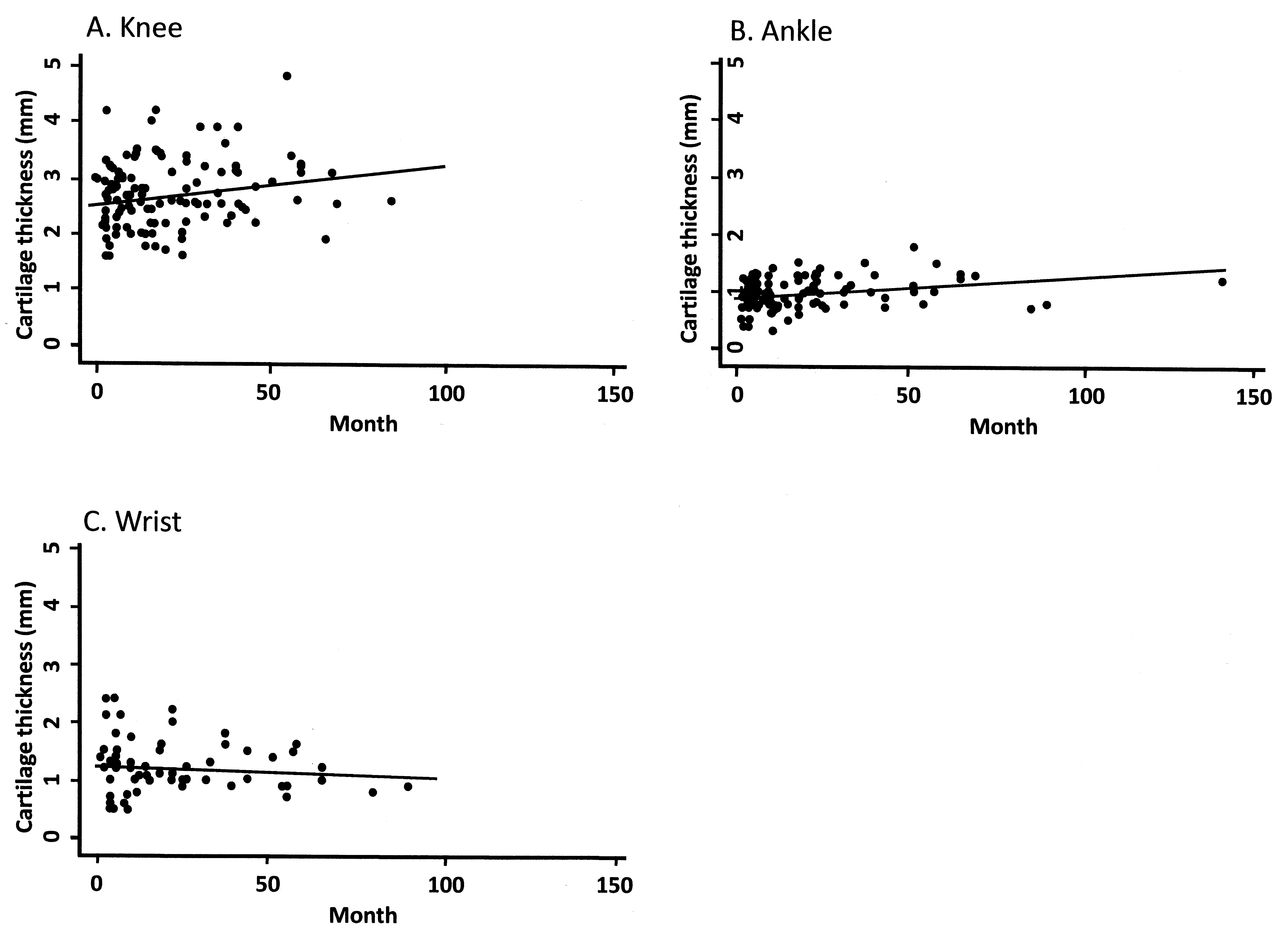
Months since last intraarticular corticosteroid injections in 3 joints correlated to cartilage thickness. Lines represent fitted values for correlation.
Disease duration
Except for the wrist and second MCP joint, we found decreased cartilage thickness in the group with disease duration < 1 year compared to the groups with disease durations > 12 months. We found significantly higher JADAS scores in the groups with the shortest and longest disease duration compared with the group with intermediate disease duration (Table 4).
Joint cartilage thickness and JADAS10 score between disease duration groups.
DISCUSSION
Joint cartilage degradation may be a result of the inflammatory articular process seen in JIA, because joint space narrowing, more than subchondral erosion, is a result of longterm disease activity18. Using high-frequency greyscale US, articular cartilage is easily visible as an anechoic or hypoechoic structure covering the subchondral bone11,12,13. By US joint examination of healthy children, we and others have previously demonstrated that the cartilage thickness is dependent on age and sex13,19. Thus, cartilage thickness gradually declined during the child’s growth, and independent of age, boys had thicker articular cartilage than girls13. In the present cross-sectional study of children with JIA, we found that these children had decreased joint cartilage thickness in the knee, wrist, and second PIP joints compared to healthy children when controlling for age and sex, whereas the cartilage thickness in the ankle and second MCP joint was not different from that of healthy controls. As in the controls, the cartilage thickness measured for all joints decreased with age in both girls and boys with JIA.
The patients were examined exactly as described, using the same US settings (EULAR standards) as in an earlier study in a healthy age-matched and sex-matched cohort11,12,13. We examined 5 different joints that are often involved in JIA. Although these joints are accessible by US, the ankle and wrist joints are more complex and therefore more difficult to scan12. In healthy children, we previously described a good intraobserver and interobserver agreement when measuring joint cartilage thickness, although a high variation coefficient was observed for the wrist joint11,12.
When we compared the joint cartilage of the knee among different subtypes of JIA, patients with systemic JIA and patients with polyarticular JIA had significantly decreased cartilage thickness. This may be due to a more aggressive disease course in these subtypes, compared to children with oligoarticular JIA, who are often regarded as having a milder disease course20. The decreased cartilage thickness measured in all joints in patients with polyarticular JIA who are RF-positive further supports the role of chronic inflammation in cartilage degradation, because RF-positive polyarticular JIA often has a persistently active disease course20,21,22.
The difference in cartilage thickness found between the patients with JIA and the controls might result from the inflammatory process in the synovial membrane during active arthritis. Thus, we compared the cartilage thickness in joints with a history of active arthritis to the contralateral joint without previous arthritis involvement. We found slightly decreased cartilage thickness in the knees and second MCP joints that had a history of active arthritis compared with the uninvolved contralateral joints, respectively. This was not the case for the ankles, wrists, and second PIP joints, a difference that might be due to the low number of observations.
Interestingly, regardless of whether the knees, wrists, and second PIP joints were ever previously affected, we found significantly decreased cartilage thickness compared to similar joints from healthy controls.
IACI is frequently used in the treatment of JIA. IACI of the knee joint in oligoarticular JIA results in full remission lasting more than 6 months in 82%23 and may be the only treatment needed in cases of oligoarticular JIA24. Treatment with glucocorticosteroids may have a significant effect on articular cartilage, as described by Céleste, et al25, who found a negative influence on cartilage synthesis after injection of triamcinolone acetonide into the knee joints of horses. They also found a negative effect on the contralateral joint used as a control. In patients with JIA, however, Huppertz, et al26 found long-lasting suppression of synovial inflammation and pannus with no toxic effects on joint cartilage, as shown by contrast-enhanced MRI in children treated with articular injections of triamcinolone hexacetonide. We found no association between the number of repeated intraarticular steroid injections and cartilage thickness in specific joints, even in joints injected more than 10 times. This may argue against the concept that corticosteroids per se accelerate the degeneration of cartilage of the diarthrodial joint. We found no significant change in cartilage thickness regardless of the timespan since the last IACI. Indeed, there appeared to be a slight increase in cartilage thickness with increased time since last injection in the knee and ankle. Hence, the question of a negative effect on joint cartilage from corticosteroid treatment is still being debated.
It may be expected that if degradation of articular cartilage is causally related to joint inflammation, a longer disease course would result in the most pronounced degradation. Surprisingly, however, we found that the group with the shortest history of disease had the lowest cartilage thickness. In our study, disease duration was defined as the time from disease onset to time of US investigation, and thus the time of active disease was not calculated. We found a significantly higher disease activity score in the group with the shortest disease duration, which may indicate that the degradation of cartilage was related to the disease activity more than to the length of time since disease onset.
Although our group previously showed good interobserver and intraobserver variability when measuring cartilage thickness by US11, it could be argued that a limitation of our study was that the US measurements were done by 1 observer who measured joint cartilage thickness in healthy children and 1 who did the measurements in the patients with JIA. However, the patients were examined with exactly the same setup as described11,12,13, and the joint cartilage thickness assessed on the stored US images was measured with the investigator blinded to clinical information about JIA subtype, disease activity, age, and sex.
Another possible limitation is that the degradation of cartilage may not appear uniformly27; that is, the degradation of cartilage might affect the joint more severely to either side of the scanned point. For the knee joint, we chose the midline of the intercondylar notch in spite of our knowledge that a possible degradation could occur more medially, as in patients with osteoarthritis28. Thus, unlike MRI, US cannot visualize the entire cartilage surface, which was a limitation of our study. The thickness of the white band is affected by the gain setting, meaning that the higher gain results in a thicker white band; however, it is also affected by the insonation angle and the focus. By excluding the white band from the cartilage measurements, an unsystematic error is introduced16. We are careful to measure the cartilage thickness orthogonally, because overestimation of the cartilage thickness may be caused by oblique insonation of the cartilage11,12,13. Panghaal, et al19 suggested a coronal medial approach to measure femoral and tibial epiphyseal cartilage. This may overcome the difficulties for children with JIA in flexing a joint with active arthritis. However, with that method the assessment of cartilage thickness may become imprecise because the insonation angle is oblique.
Our study was cross-sectional, which is acceptable in this context because we wanted to compare cartilage thickness among different JIA categories. It would be useful in the future to do a consecutive followup study, which would allow more thorough investigation of the influence of disease activity and treatment responses on cartilage thickness, and following newly diagnosed patients from baseline until acceptable treatment or complete remission is achieved.
We found decreased joint cartilage thickness in children with JIA compared to children without JIA. When controlled for age and sex, children with polyarticular and systemic JIA had decreased cartilage thickness compared to children diagnosed with oligoarticular JIA. There may be several reasons for the decline in cartilage thickness in the JIA groups, but the inflammatory process itself may play an important role, rather than the possible harm of glucocorticoid treatment.
Footnotes
-
Supported by the Danish Arthritis Association.
- Accepted for publication May 21, 2013.








{kind=link}
{kind=link}
{kind=link}
{kind=link}