

Abstract
Objective. To study longterm outcomes of 60 patients with palindromic rheumatism (PR) diagnosed in 1967–1984.
Methods. A cohort of patients with PR was identified in Jyväskylä Central Hospital in 1967–84, and reexamined in 1984–86. In 2006, medical records of the patients were reviewed to analyze the proportion of patients who had developed chronic rheumatoid arthritis (RA), had joint replacement surgery, or had died. Patients’ health status was reviewed by mail questionnaires including functional status on the Health Assessment Questionnaire (HAQ), pain, and the number of painful joints.
Results. Forty patients developed chronic RA over the observation period of over 20 years, among whom 38 patients within 10 years and 2 patients after 10 years. Twenty-four patients had died by 2006, 17 (42%) in the RA group and 7 (35%) in the non-RA group. Nine patients, all in the RA group (23%), had received 1 or more joint replacements. The mean HAQ score was 0.57 in the non-RA survivors (mean age 70 yrs), compared to 0.89 in the RA group (mean age 66 yrs) (p = 0.020, adjusted for age). Pain scores and the number of painful joints were similar between the groups.
Conclusion. Two-thirds of the patients with PR developed chronic arthritis. The risk to develop chronic arthritis remained over 10 years. The RA group was characterized with functional declines and having joint replacements as longterm outcomes of the disease.
Palindromic rheumatism (PR) is an idiopathic recurrent arthritis syndrome characterized by episodic attacks in joints and/or periarticular tissue without residual joint damage1. Typically, a PR attack occurs suddenly without any precipitating events or warning symptoms. The attack may appear in any joint, but finger joints, wrists, and knees are most commonly affected2. An attack may also be polyarticular although monoarticular attacks predominate. Most attacks are painful. The affected joint is stiff with decreased function; it may be swollen, warm, and sometimes also red. Patients may have fever and other systemic symptoms. Attacks are usually short, from hours up to 1 week. The frequency is variable. Abnormal clinical, laboratory, or radiological changes are not found between the attacks.
The etiopathogenesis of PR remains unknown, but genetic factors may predispose to its development3–5. Further, rheumatoid factor (RF) and anticyclic citrullinated peptide antibodies (anti-CCP) are more common in patients who progress to develop chronic rheumatoid arthritis (RA)2–8. By contrast, therapy with methotrexate may prevent the development of chronic arthritis9.
Proposed diagnostic criteria for PR include: (1) recurrent attacks of sudden-onset mono or polyarthritis or of periarticular tissue inflammation, lasting from a few hours to 1 week; (2) verification of at least 1 attack by a physician; (3) subsequent attacks in at least 3 different joints; (4) exclusion of other forms of arthritis2. The list of diseases that may mimic PR is long and includes common rheumatic conditions such as crystal arthropathies, reactive arthritis, and other seronegative spondylarthropathies as well as more uncommon diseases such as intermittent hydrarthrosis, Bechet’s disease, relapsing polychondritis, sarcoidosis and Whipple’s disease7.
Little information is available regarding the longterm outcomes of PR. Therefore, we studied longterm outcomes of a cohort of patients with PR who were identified at Jyväskylä Central Hospital in 1967–84.
MATERIALS AND METHODS
In early 1980s, a cohort of 60 patients with PR was identified in Jyväskylä Central Hospital, diagnosed between 1967–84, and re-examined in 1984–862. By that time, 35 patients had developed chronic RA. In some cases, seroconversion to RF positivity preceded the chronicity2. All patients received antirheumatic therapy with disease modifying antirheumatic drugs (DMARD), except 2 patients who had few mild attacks and were treated with nonsteroidal antiinflammatory drugs (NSAID) only.
In 2006, medical records of the patients were reviewed to analyze health conditions including diagnoses of other connective tissue diseases and outcomes. The review was focused specifically on the proportion of patients who developed chronic RA lasting more than 6 weeks, had joint replacement surgery, or had died. Data concerning the duration of the use of DMARD over the first 10 years after diagnosis also was collected.
Questionnaires were mailed to the patients to review current health status including functional status on the Health Assessment Questionnaire (HAQ) and pain on a 0–100 mm visual analog scale (VAS). Self-reported joint pain was queried according to the Rheumatoid Arthritis Disease Activity Index (RADAI) format including 16 joints or joint areas10 and reported as a number of painful joints or joint areas with any reported level of pain. Central Finland Health Care District Ethics Committee approved the study.
Statistical methods
Measures of health status and longterm outcomes were compared between the patients who had developed clinical chronic RA versus other patients (non-RA). Descriptive data are presented as means with standard deviation (SD), medians with interquartile range (IQR), and percentages. Student’s t-test, chi-squared test, Mann-Whitney test, and a linear regression model were used for statistical comparisons. Kaplan-Meier statistics were applied to illustrate the cumulative probability to develop chronic arthritis after diagnosis of PR.
RESULTS
Among 60 patients, 40 developed chronic RA by 2006. Almost all (38/40) patients developed chronic RA during the first 10 years after diagnosis of PR, and 2 other patients developed chronic RA after 13 and 11 years. Twenty patients did not proceed to RA and did not seek help from the rheumatology clinic for arthritis (non-RA group). One of these patients had a concomitant diagnosis of Wegener’s granulomatosis, and 2 were later diagnosed with polymyalgia rheumatica and temporal arteritis. Figure 1 illustrates the cumulative probability of chronic RA over 20 years of followup.
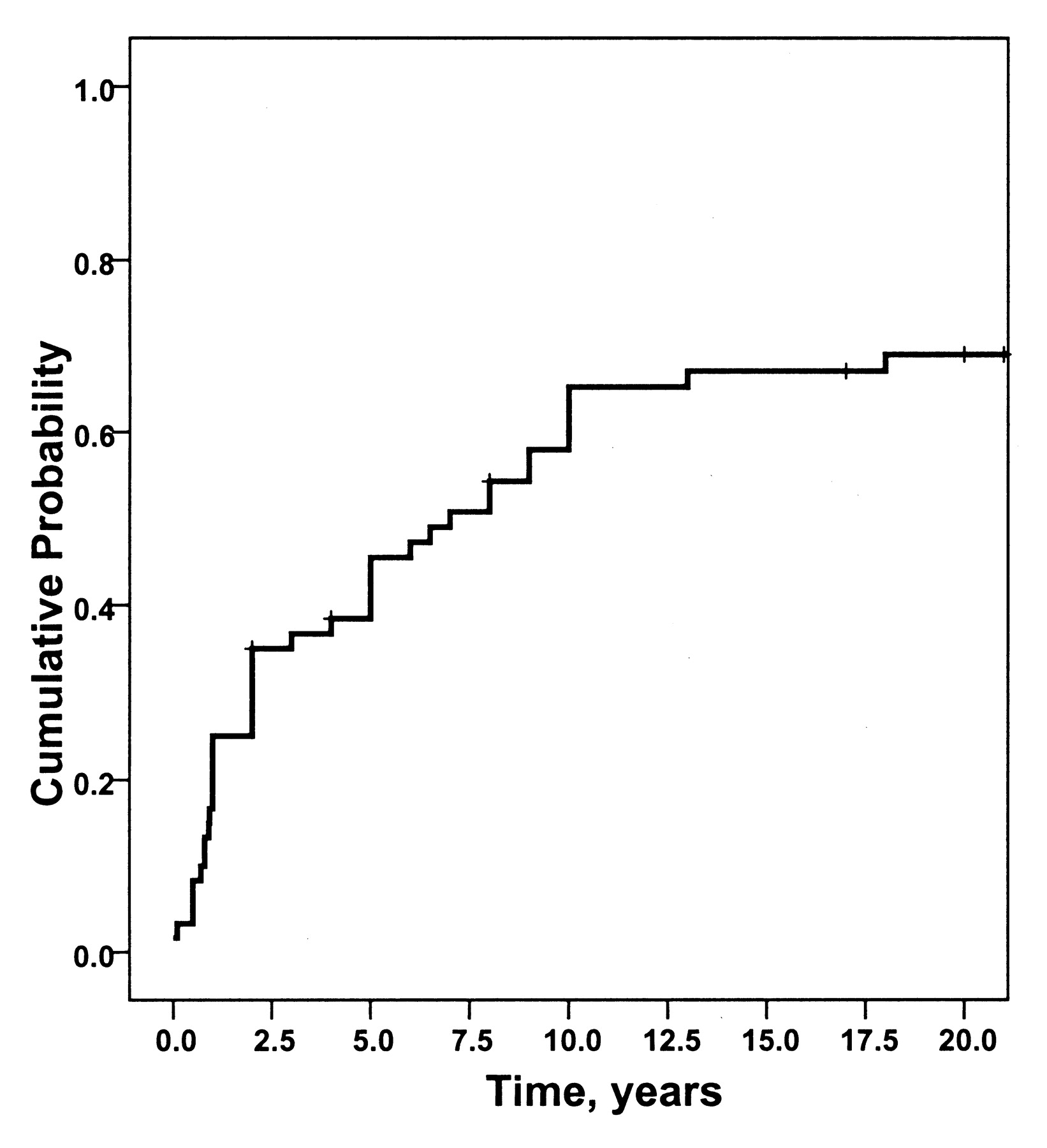
Kaplan-Meier probability to develop chronic rheumatoid arthritis in 60 patients who presented with palindromic rheumatism in 1967–84.
At the time of diagnosis of PR, mean (SD) age was 49 (11) years. Positive RF was more frequent in the patients who developed chronic RA (77%) but was nonetheless seen in 50% of the non-RA group (p = 0.036) (Table 1).
Baseline characteristics and followup data of the 60 patients who presented with palindromic rheumatism (PR) in 1967–84.
Twenty-four patients had died by 2006, 17 (43%) in the RA group and 7 (35%) in the non-RA group (Table 1). Nine patients, all in the RA group (23%) (Table 1), had received 1–4 total joint replacements including 8 knee, 8 hip, and 1 ankle prosthesis. Three of the hip replacements were due to a hip fracture. During the first 10 years, patients in the RA group had taken DMARD for a median (IQR) of 7.3 (3.6, 9.3) years, and in the non-RA group 3.4 (0.2, 8.1) years (p = 0.031).
At the time of review, the mean (SD) age of the surviving patients was 70.4 years in the non-RA group and 66.0 years in RA group (Table 2). Twelve of the 13 survivors in the non-RA group and 21 of the 23 in the RA group responded to the questionnaire. The mean HAQ score was 0.57 in the non-RA group and 0.89 in the RA group (p = 0.020, adjusted for age). Pain scores were 43 versus 42 in non-RA and RA groups, respectively (Table 2). The number of painful joints on RADAI was 8.0 in the non-RA group and 9.4 in the RA group (p = 0.49).
Current health status of 33 of 36 surviving patients who presented with palindromic rheumatism in 1967–84.
DISCUSSION
To our knowledge, this is the first report regarding longterm (20+ yrs) outcomes of patients diagnosed with PR. Two-thirds of these patients developed chronic arthritis, almost all within 10 years after the diagnosis of PR, while 2 patients developed chronic RA later. In the study of Gonzalez-Lopez, et al11, one-third of patients with PR developed RA over a mean followup of 4.8 years. In another study, 27 of 43 patients (63%) developed chronic inflammatory arthritis during a mean followup of 7 years12.
Positive RF was found in 77% of those who developed chronic RA and in 50% of those did not. Although these between-group differences are statistically significant, at an individual level, if 50% of non-RA patients have positive RF, the test has limited clinical prognostic value.
In this relatively small group of patients, mortality was only slightly higher in patients with RA compared to the non-RA group. However, longterm outcomes in terms of joint replacements differed between the groups: none of the non-RA patients versus 23% of patients with RA had joint replacements. This finding indicates that longterm outcomes of patients who present with PR but proceeded to chronic RA appear as severe as longterm outcomes of RA in general over the last 2 decades13.
Current self-reported data indicated that patients who did not develop chronic RA had pain and joint pain at similar levels as patients with chronic RA (Table 2). Functional capacity was statistically significantly poorer in patients with RA. Aging is an important determinant of the HAQ14 and a comparatively high mean HAQ value of 0.57 in the PR group may reflect aging. We have previously shown that musculoskeletal symptoms are prevalent in the elderly general non-RA population15.
In this study, patients who did not develop chronic arthritis had less DMARD use compared to the RA group. Gonzalez-Lopez, et al11 showed that the treatment with DMARD postpones the risk to develop chronic arthritis. This could not be analyzed in our study because all but 2 patients were treated with DMARD. In fact, PR may represent “pre-rheumatoid arthritis”16, and it remains to be shown whether currently used DMARD including methotrexate could prevent the development of PR to chronic arthritis in some individuals.
Limitations of our study include a retrospective nature of the identification of the patients. Therefore, it is possible that some patients with PR during 1967–84 may have been missed. Only a prospective review and followup of all new patients referred to a rheumatology clinic over a longer period of time would provide a valid estimate of a proportion of patients who proceed from PR to RA.
In conclusion, two-thirds of patients with PR developed chronic arthritis in our study. The risk to develop chronic arthritis remained over 10 years. Longterm outcomes were worse in patients who develop chronic arthritis, in terms of functional capacity and the need for joint replacements.
Footnotes
- Accepted for publication April 3, 2009.








{kind=link}