

Abstract
Objective. To test the efficacies of a strategy for preventing tuberculosis (TB) in Indian patients with inflammatory rheumatic diseases (IRD) treated with tumor necrosis factor-α (TNF-α) inhibitor.
Methods. The screening strategy included tuberculosis skin test (TST), QuantiFERON-TB Gold (QTG) test, standard chest radiograph, and contrast enhanced-computerized tomography of the chest (CT).
Results. Among 53 patients screened, 17 (32%) had ≥ 1 test positive, with 5 (9.4%) patients having TB infection (clinical, CT, biopsy). The remaining 12 patients showed latent TB; 1 additional patient with negative screening tests was diagnosed with latent TB retrospectively for he developed TB disease within a few weeks of receiving infliximab. The remaining 35 patients tested negative with all tests. The combination of 4 screening tests gave a sensitivity of 0.83, specificity of 0.74, positive predictive value (PPV) 0.29, and negative predictive value (NPV) 0.97. Only 22 patients could afford treatment with TNF-α inhibitors; 19 of them were negative in the screening tests. Three patients who were positive on TST and/or QTG received prophylactic treatment with TNF-α inhibitor. Since implementation of the screening strategy, only 1 of 22 (4.5%) patients given TNF-α inhibitor developed probable TB disease.
Conclusion. With the use of these 4 TB screening tests in India, where TB is highly prevalent, TB could be excluded with a high degree of certainty (NPV 0.97). However, as even this combination of tests has only moderate sensitivity and specificity and poor PPV for detecting TB, vigilance may be advisable even if only one of the tests is positive.
- TUBERCULOSIS INFECTION
- LATENT TUBERCULOSIS INFECTION
- TUMOR NECROSIS FACTOR-α INHIBITOR
- INFLAMMATORY RHEUMATIC DISEASES
- INDIA
- SCREENING STRATEGY
Patients with inflammatory rheumatic disease (IRD) treated with tumor necrosis factor-α (TNFα) inhibitors have an increased risk of Mycobacterium tuberculosis (TB) infection, the magnitude of which could vary with the agent, dose, dose schedule, and the background load (high, medium, or low burden regions) of TB1. Most clinical studies have reported TB occurring in patients receiving the anti-TNF monoclonal antibody infliximab within a relatively short period after receiving the drug (12–21 weeks). This is consistent with reactivation of latent TB infection. This is in contrast to cases with the soluble TNF-α receptor etanercept that have reported a median time to onset 3–5 times longer, consistent with de novo reinfection with M. tuberculosis2,3. With increasing use of these drugs and the emerging problem of TB, several countries have developed national guidelines for testing for latent TB infection before TNF-α inhibitor therapy is initiated, as discussed in a recent review4.
India is a “high TB burden” country; in 2004 TB prevalence was estimated to be 2.9 million cases (269 per 100,000), of which smear-positive pulmonary TB disease numbered 0.8 million (76 per 100,000)5. Nontuberculosis mycobacterial infection isolation rates in India have been reported ranging from 0.5% to 8.6%6–8. Despite such a high TB burden, there is no national guideline for latent TB screening of patients being considered for TNF-α inhibitor treatment.
Infliximab, one of the TNF-α inhibitors, was released in India in 2002. Over the next 2 years 2 authors (ANM, SK) treated 22 patients with IRD with infliximab with no predefined strategy for screening of latent TB infection. IRD included rheumatoid arthritis (RA; n = 11), ankylosing spondylitis (AS; n = 7), psoriatic arthritis (n = 2), and Behçet’s disease (n = 2). Four patients (18.2%) developed severe extraarticular TB within 6 months (patients were included in a report from 2 rheumatology clinics in Delhi9); 2 required prolonged periods of therapy with 6 to 9 anti-TB drugs for disease control. However, no deaths occurred among them. Because of high frequency of TB among these patients, use of TNF-α inhibitors was temporarily curtailed.
Taking into account the published guidelines and in particular the Spanish recommendations10, and in consultation with local TB experts, it was decided to screen all intent-to-treat patients with TNF-α inhibitors for latent TB infection with a well defined strategy (see below). We present an audit of results of the occurrence of TB disease after the implementation of this strategy.
MATERIALS AND METHODS
Latent TB screening strategy
The following screening strategy was implemented: (1) Tuberculosis skin test (TST) using the Mantoux method with 10 tuberculin units (TU) purified protein derivative (PPD) RT23. This tuberculin dose is commonly used in India for performing Mantoux test in cases of chronic illness with some degree of immunocompromised state11. The test was read for maximum transverse diameter of induration between 48 and 72 hours. A cutoff of ≥ 10 mm, as recommended by the American Thoracic Society and the US Centers for Disease Control and Prevention (CDC; endorsed by the Council of the Infectious Diseases Society of America), was adopted considering that the subjects were from a high-prevalence country and they had a clinical condition, that is, an IRD12. (2) An interferon-γ release assay (IGRA)13, the QuantiFERON-TB Gold (QTG) test, was performed with a commercial kit (Cellestis Limited, Carnegie, Victoria, Australia), according to the manufacturer’s instructions. (3) A standard chest radiograph, posteroanterior view. (4) Contrast enhanced computerized tomography (CT) of the chest. CT scan was included to ensure that no patient starting anti-TNF treatment was overlooked for latent TB infection.
Treatment of latent TB infection or TB disease and administration of TNF-α inhibitors
Patients with active TB disease detected on chest radiograph or CT or on histopathology were treated according to the national guidelines for treatment of TB disease with slight modification. The 4-drug regimen included isonicotinic acid hydrazine (INH) plus rifampicin plus pyrazinamide plus ethambutol for 2 months, followed by INH plus rifampicin for 4 months. A total of 6 months of treatment was given before administering TNF-α inhibitor drugs. Patients positive for latent TB infection on screening and who were able to arrange finances for taking TNF-α inhibitors were given 2 drugs (INH plus rifampicin) for 2 months before they started TNF-α inhibitor. Both groups of patients, i.e., those with TB disease and those with latent TB infection, were then maintained on INH plus rifampicin throughout the period of TNF-α inhibitor treatment and another 2 months beyond the last dose of TNF-α inhibitor. The decision to treat latent TB infection with INH plus rifampicin was based upon the Tuberculosis Trial Consortium report of a comparison of INH plus long-acting rifampicin against INH monotherapy14,15; and the prevailing practice in India for preventing emergence of resistance to INH. Recent data on evidence-based treatment of latent TB infection supports this regimen16. They were also maintained on the INH plus rifampicin combination throughout the period of TNF-α inhibitor treatment and for 2 months after the last dose. This practice differed from those in other countries, but was considered prudent for the high TB conditions in India.
Infliximab was given at the dose of 5 mg/kg body weight for all the diseases, except that patients with RA were given 3 mg/kg body weight. Following the prevalent practice in India a loading-dose of infliximab was not given. This practice was adopted following a report that reactivation of latent TB infection can be almost completely prevented by avoiding the loading dose of infliximab17. Subsequent doses were given depending upon the clinical response and affordability, without any predetermined schedule. Etanercept was given at a fixed dose of 50 mg subcutaneously every week. The duration of treatment with etanercept was variable, depending upon affordability, usually only for 2–3 months or intermittently when patients could arrange the finances.
RESULTS
Demographic data
A total of 67 intent-to-treat patients with IRD were screened using this strategy. Finally, only 53 patients completed all the 4 tests. The median age was 41 years (range 26–68 yrs) and included 30 men and 23 women. These included cases of RA (n = 13), ankylosing spondylitis-spondyloarthritis (AS-SpA; n = 27), sarcoidosis (n = 5, Lofgren presentation in 3), and miscellaneous conditions (n = 8) that consisted of ankle TB (n = 2), Poncet’s arthritis (TB-reactive arthritis; n = 2), and 1 patient each with biomechanical low-back pain (suspected to be AS at presentation; Sjögren’s syndrome, resistant dermatomyositis, and resistant adult-onset Still’s disease). There were 17 patients (mostly AS) who had taken only “alternative” systems of medicine and intermittent nonsteroidal antiinflammatory drugs. Nine of these had been given pamidronate plus methylprednisolone infusions monthly for 6 months, a regimen often given to patients with AS in India if unable to afford anti-TNF-α treatment18. This was followed by thalidomide for at least 4 months. Upon failure with this form of treatment they were then offered anti-TNF treatment. There were 19 patients who in the past had taken suboptimal doses of methotrexate (7.5 mg per week, or sulfasalazine and occasionally hydroxychloroquine for a few weeks to a few months). When they achieved no relief they had switched to alternative medicines. Another 17 patients (mostly non-AS patients) were under our care for some time before they were considered for anti-TNF treatment, taking methotrexate 20 mg weekly, with hydroxychloroquine in addition to intermittent (weekly) doses of prednisolone 15–20 mg.
Screening tests for TB; sensitivity and specificity
All 4 TB screening tests were available from 53 patients, with at least 1 positive test in 17 (32%) cases. Five patients (9.4%) were diagnosed with TB disease clinically, in whom 3 diagnoses were confirmed on CT scans. The fourth patient showed only apical fibrotic lesions in CT, but had clinical features of Poncet’s disease and positive TST and QTG, therefore she was diagnosed as having TB. The fifth patient had ankle arthritis with normal chest radiograph and chest CT, but a synovial biopsy showed tuberculous synovitis, therefore he was also diagnosed with TB. In the remaining 12 patients, clinically there was no TB disease, and they were diagnosed as having latent TB infection. Thirty-five patients were negative in all the 4 screening tests and were diagnosed as having no latent infection or TB disease.
Based upon these figures the sensitivity of the combination of TST, QTG, and CT was 0.83, specificity was 0.74, positive predictive value 0.29, and negative predictive value (NPV) 0.97. (One patient who was negative for all tests but developed active TB within 8 weeks of administration of infliximab was deemed to have latent infection. Thus in the final analysis there were 13 patients with latent TB infection among a total of 53 patients studied. This was taken into account calculating the above figures.)
TST and QTG positivity
Both the QTG and the TST tests were positive in 10 patients; only QTG or TST was positive in 3 and 4 patients, respectively; both tests were negative in 6 patients. Details of these 6 patients were as follows: 3 had sarcoidosis (Lofgren); one was confirmed on mediastinal lymph node biopsy; in the other 2 patients the diagnosis was based upon typical clinical features of Lofgren syndrome. Bilateral hilar lymph nodes were detected on CT, and excellent response to standard treatment for sarcoidosis was seen. The remaining 3 patients with some CT findings were considered nonspecific and to not have latent TB infection (details below). The association of these 2 tests was significant in the entire group taken together. Among patients with TB disease, the concordance rate was 100%, while among patients with latent TB infection, there was significant discordance (Table 1). Only one of the 53 patients showed an “indeterminate” QTG test result.
Tuberculin skin test (TST) and QuantiFERON-TB Gold (QTG) test positivity in patients with TB and latent TB infection.
Chest radiograph and CT results
Chest radiographs showed some abnormality in 5 of the 53 patients. Hilar adenopathy was detected in 3, which was confirmed on chest CT scans. Combined with clinical assessment these 3 patients were considered to have typical Lofgren syndrome and were treated accordingly. Of the remaining 2 patients, one showed fibrotic lesion at the apex (confirmed on CT). She had persistent ankle arthritis with high-positive TST (ulcerated Mantoux test) and positive QTG test. She was started on standard treatment for TB disease, with satisfactory response. The other patient, also with positive TST and QTG, showed suspicious lung nodules that were confirmed on CT, which was consistent with TB disease and treated accordingly. CT scans showed some abnormalities in 14/53 patients. Seven were considered compatible with TB, 4 with latent TB infection (fibrotic healed lesions, or small inactive nodular lesions), and 3 with TB disease (pulmonary infiltrates/nodules and/or mediastinal lymph nodes with necrosis). All 7 patients tested positive on TST and QTG tests, and were treated. In summary, CT scan was never positive unless either TST or QFT or both were positive.
Details for the remaining 7 patients with abnormal CT scans but not considered to have TB disease or latent infection were as follows: 4 were diagnosed with sarcoidosis (bilateral hilar lymphadenopathy; 3 had suspicious findings on chest radiograph as noted above), one had findings of interstitial lung disease, one had axillary lymph nodes with generalized reticuloendothelial hyperplasia (including splenomegaly) as part of severe RA, and one had nonspecific pleural thickening and additional minor findings considered nonspecific.
Treatment with TNF-α inhibitors and development of TB disease
Since implementation of the strategy above, only 22 of these 53 patients could afford treatment with TNF-α inhibitors (21 with infliximab, 1 with etanercept); 19 of them were negative for TST and QTG tests; 3 were positive for TST and/or QTG. Among these 22 patients, 1 who had tested negative for TST and QTG developed probable TB disease within 8 weeks of the last dose of infliximab; this had not been detected earlier by any of the 4 TB screening tests but in retrospect was considered latent infection. An additional patient was suspected with TB disease 1.5 years after the last dose of infliximab, which could have been reinfection. The first patient developed fever and lower zone pneumonitis within 2 months of a single dose of infliximab. Sputum and bronchoalveolar lavage material were negative for M. tuberculosis. However, as there was no clinical response to standard antibiotic treatment, the pulmonologist recommended full treatment for TB disease; the patient recovered slowly but completely. He agreed to restart infliximab after full course of anti-TB treatment. The second patient developed fever and pleural effusion 1.5 years after the third and last dose of infliximab. Aspiration of the effusion and antibiotic treatment was ineffective and he developed empyema. Again the pulmonologist recommended full treatment for TB disease, after which he recovered slowly. This patient most probably had a TB reinfection and not a TB flare. However, he did not agree to restart infliximab treatment. Two patients with ankle arthritis were misdiagnosed as “inflammatory arthritis” at the first contact in the outpatient rheumatology service, and therefore routine TB screening tests were performed if they required anti-TNF treatment in future. But clinical reevaluation by the senior rheumatologist revealed the correct diagnosis of TB of the ankle joint. These patients were then treated as active TB disease according to standard guidelines. Patients with Poncet’s disease were also treated similarly as active TB disease.
Treatment with TNF-α inhibitor after full treatment of TB disease
Four patients were given treatment with TNF-α inhibitor after at least 6 months of treatment for TB disease. During this period they continued on the 2-drug treatment (INH plus rifampicin), with no TB disease flare during the followup period (> 1.5 yrs).
Reduction in incidence of TB flare
Before we adopted this policy of latent TB infection screening the incidence of TB disease flare was about 18.2%; this declined to 4.5% (1/22) with the modified TB screening strategy (p = 0.3, Fisher’s exact test). The patient who developed probable TB disease 18 months after the last dose of infliximab was considered as a reinfection and not included in this calculation.
DISCUSSION
Our strategy for TB screening among intent-to-treat patients who were to receive TNF-α inhibitors showed a high NPV, with very small chance of TB flare among patients given this treatment. Our strategy for reducing TB disease among patients receiving TNF-α inhibitor therapy has differed in the following aspects: (1) Use of both TST and QTG testing in all patients. (2) Use of chest CT scanning helped to detect additional cases of TB disease that were missed on chest radiographs. (3) Doing away with the loading dose of infliximab. Using this standardized policy, the proportion of patients developing TB disease went down from 18% to 4.5%. Although much higher than the figures of 0.6% to 1% quoted from randomized controlled trials of anti-TNF monoclonal antibodies from Europe and South America4, this was considered to be a clinically significant improvement under Indian conditions. It was disappointing that despite these stringent measures TB disease flares could not be brought down to zero. Other studies have similar observations10,19. As available tests for latent TB screening are not 100% sensitive, some patients may be slipping through this screening procedure.
The use of 10 TU PPD for Mantoux TST was based upon the prevailing practice in India for patients with chronic diseases with the possibility of an immunocompromised state11. Some investigators have not favored TST for screening of latent TB infections in IRD, fearing inherent cutaneous anergy giving false-negative results20. However, most have used 2 or 5 TU PPD for TST (in some reports the dose is not given)21–26. Therefore, it would appear that a mild immunocompromised state in patients with IRD could be compensated for by using a higher dose of 10 TU of PPD, improving the rate of detection of latent TB infection. Experts have cautioned on the use of TST for latent TB screening because of reliability concerns, i.e., prior bacillus Calmette-Guerin (BCG) vaccination or exposure to non-TB mycobacteria interfering with the results27,28. In India BCG vaccine is given at birth and is not repeated thereafter29. Two recent reports from high-burden TB regions concluded that BCG vaccination did not increase the risk of positive skin test in unexposed individuals, but it was closely related to exposure risk for TB among case and control contacts30,31. A European report on interference of BCG vaccination in the interpretation of TST conceded that the findings could be specific for a low-prevalence area32. Thus, TST remains a useful tool for diagnosing TB infection despite BCG vaccination in a region of high disease burden like India. The decision to use induration ≥ 10 mm as the cutoff point for considering the TST to be positive followed recommendations of the American Thoracic Society and the CDC12. That is, 3 different cutoff points are recommended for considering the test positive among persons from different populations as follows: (1) For persons at highest risk for developing active TB if they are infected with M. tuberculosis (i.e., those with HIV infection, those who are receiving immunosuppressive therapy, those who have had recent close contact with infectious TB, or who have abnormal chest radiographs consistent with prior TB), the recommended cutoff for induration is ≥ 5 mm. (2) For subjects with an increased probability of recent infection or with other clinical conditions that increase the risk for progression to active TB (e.g., persons from high-prevalence countries, or with clinical conditions such as silicosis, diabetes mellitus, etc.) ≥ 10 mm induration is recommended to be considered positive. (3) For persons at low risk for TB, for whom tuberculin testing is not generally indicated, ≥ 15 mm induration is recommended to be considered positive. For our studies a cutoff ≥ 10 mm was adopted considering that subjects were from India, a high-prevalence country, and they had an IRD. High-dose glucocorticoids could modify the response to TST, which may require using a different cutoff level for induration to be considered positive. However, prolonged use of high-dose glucocorticoids in IRD is not common practice in India because of the fear of TB and type II diabetes mellitus, 2 common widespread diseases in this country.
Recently, we have seen the development of the IGRA on the strong theoretical grounds of high specificity for M. tuberculosis infection13,33–35. Based on these findings, an IGRA-based test, the QTG, has been recommended as the preferred test for latent TB screening in a normal population13,36. However, as discussed by Keane and Bresnihan4, the usefulness of the QTG in immunocompromised patients (e.g., those with IRD) has not been proven beyond doubt and experts continue to recommend TST in combination with a risk stratification strategy in these situations. Conflicting results have been reported in a few recent studies that used QTG for latent TB screening in patients with IRD25,37. While Matulis, et al found QTG to be superior to TST25, Greenberg, et al found no difference between QTG and TST, and recommended modified TST for screening of latent infection in this patient population37. Others recommend combination of IGRA and TST in detecting latent infection in patients with IRD38,39. Our observations showed a low sensitivity of TST (even when 10 TU PPD was used) as well as QTG. Also, these tests appeared to be detecting somewhat different patient populations. When both tests were used, however, 94% of cases of TB disease/probable latent infection could be detected.
An important question was whether it was necessary to get CT chest scans in every patient considered for TNF-α inhibitors. That is, did we have patients with negative TST and/or QTG but CT scans that showed TB disease. The result was that the CT scan was never positive unless either TST or QFT was positive. There were patients with abnormal CT chest scans, but these were typical for other pathologies — sarcoidosis, interstitial lung disease, or nonspecific insignificant fibrotic bands at the lung bases. Based on these findings it would be reasonable if CT chest scanning is reserved for patients with positive TST and/or QTG. It could be safer, and cost-effective, and yet would help in distinguishing TB disease from latent infection, which is important as these groups are given different anti-TB drug regimens.
A weakness of our report is a possible selection bias, where only financially well-off patients were given TNF-α inhibitor therapy. The possibility of TB flare could be quite different among such patients compared to those who were not well off.
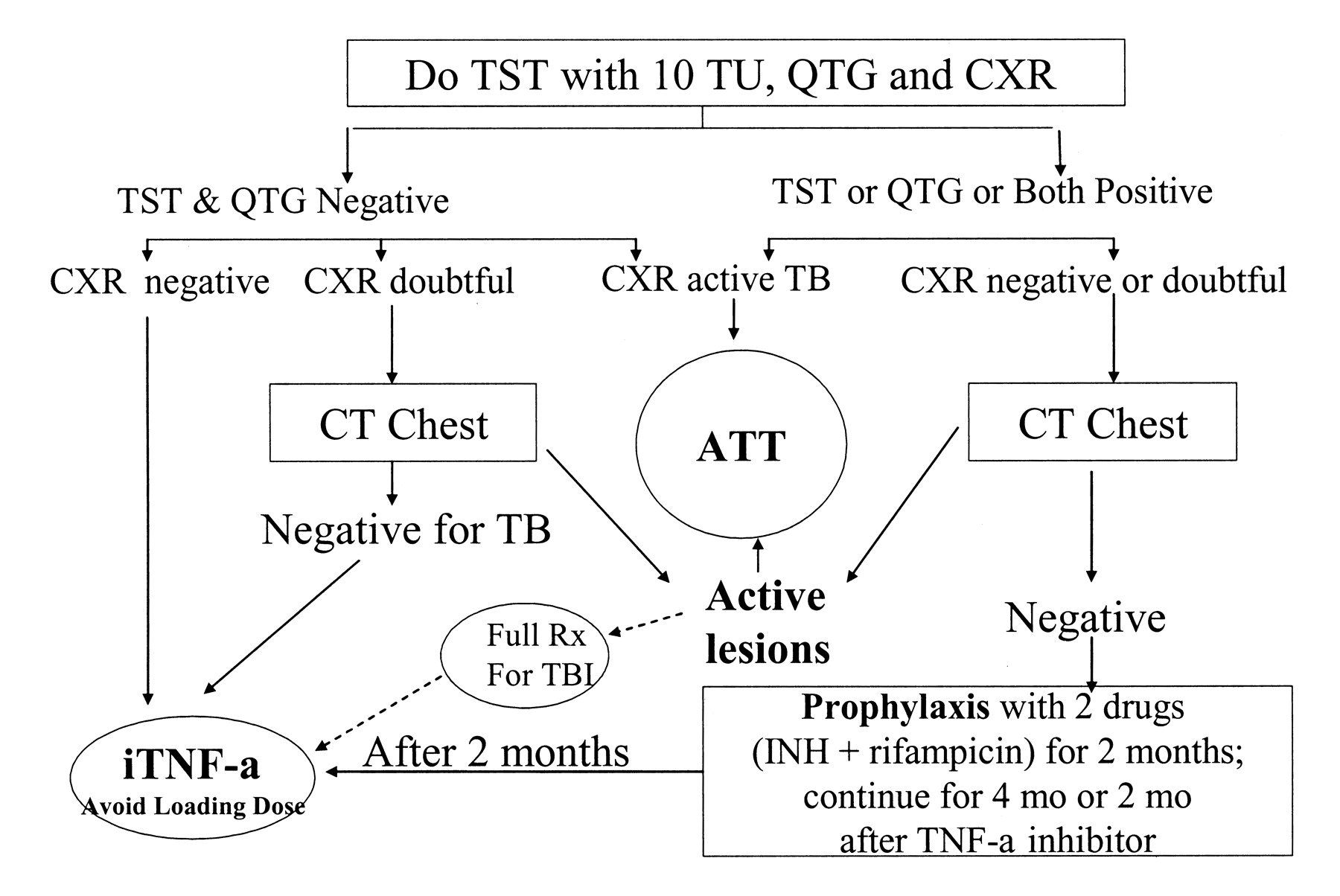
Based on our observations we believe that for screening of latent TB infection among patients with IRD it may be prudent to use both the TST and the QTG, along with chest radiograph and CT scan, only in cases of suspected TB disease. Others have also recommended continued use of TST in populations with depressed cell-mediated immune responses; patients with IRD may belong to this group39. Use of the IGRA as the additional screening test has also been recommended by some authorities in certain situations38,40,41. Therefore, we recommend an algorithm for the screening and treatment of latent TB infection among Indian patients with IRD in the intent-to-treat category for TNF-α inhibitors (Figure 1).

Algorithm for the screening and treatment of latent TB infection among Indian inflammatory rheumatic disease patients with intent-to-treat with tumor necrosis factor-α inhibitors (iTNF-α). ATT: anti-TB treatment.
Acknowledgments
We thank Prof. Alladi Mohan, MD, Chief, Division of Pulmonary and Critical Care Medicine, and Head, Department of Medicine, Sri Venkateswara Institute of Medical Sciences, Tirupati, Andhra Pradesh, and Dr. P.K. Mangla, MD, Senior Consultant Pulmonologist, Indian Spinal Injuries Centre Superspeciality Hospital, New Delhi, for their expert advice on TB diagnosis, diagnostic tests, their interpretation, and treatment. Thanks also to Prashant Deshmukh for meticulous data entry and record-keeping, Rajiv Ratna Raja, Occupational Therapist, and Mohd. Irfan, Physiotherapist, for performing outcome measures in patients.
Footnotes
- Accepted for publication January 27, 2009.








{kind=link}