

Abstract
Objective. To analyze clinical and serological characteristics of subjects with scleroderma renal crisis (SRC) in Italian patients with systemic sclerosis (SSc).
Methods. A retrospective analysis of medical records from 9 Italian rheumatologic referral centers was carried out. All patients with SRC and an available serum sample at the time of crisis were included. Antinuclear antibodies (ANA) by indirect immunofluorescence, anti-topoisomerase (topo) I by enzyme-linked assay (ELISA), anti-RNA polymerases (RNAP) by ELISA for the subunit III, and immunoprecipitation (IP) were performed.
Results. Forty-six cases (38 female; 40 diffuse cutaneous SSc) were identified. Mean age at SSc and SRC onset was 52.8 years ± 13.2 and 55.4 years ± 11.8, respectively. ANA were present in 44 patients (96%). Anti-topo I antibodies were detected in 30 (65%), anti-RNAP I–III in 7 (15%). No differences emerged between these 2 groups for their main clinical characteristics. The proportion of patients in the anti-RNAP I–III group developing SRC early (< 18 mo) in the course of SSc was significantly higher (p = 0.03). Cumulative survival rates were 64%, 53%, and 35% at 1, 2, and 10 years of followup, respectively. Survival rates of SSc patients significantly differed according to their autoantibody profile, being lower in the anti-topo I than in the anti-RNAP I–III group (p = 0.034).
Conclusion. SRC is a rare manifestation of SSc in Italy but it is still associated with severe prognosis. Anti-topo I reactivity was more frequent than anti-RNAP I–III in our patients with SRC and was associated with delayed onset and high mortality rates.
Systemic sclerosis (scleroderma, SSc) is a chronic inflammatory multiorgan disease whose etiology is still unclear but which has a strong autoimmune background1. As many as 95% of patients with SSc display a positive serologic reaction to antinuclear antibodies (ANA); moreover, autoantibodies represent a valuable tool in disease classification and prognosis2,3.
The main pathological features of SSc are endothelial damage and abnormal collagen deposition that clinically manifest with a variable degree of cutaneous and visceral fibrosis and vascular complications. One of the most serious of the latter is characterized by onset of a rapidly progressive acute renal failure eventually accompanied by malignant hypertension, termed scleroderma renal crisis (SRC)4. In British and US cohorts, about 10% of SSc patients experience SRC, most of them early in the disease course5. The frequency is also higher (up to 25%) when only patients with diffuse cutaneous involvement are considered6.
Antibodies to the RNA polymerase (RNAP) subunits I–III are mutually exclusive with respect to the 2 other major SSc autoantibody groups, anti-topoisomerase I (anti-topo I) and anticentromere (ACA) antibodies, distinguishing a serologic subset of patients that, in contrast to anti-topo I and ACA, more frequently display diffuse cutaneous and renal involvement, in particular SRC7,8. This complication has been reported to occur at lower rates in countries in the Mediterranean area versus UK and US series9 and, in parallel, anti-RNAP I–III have been reported to be relatively rare in patients from Mediterranean countries10. Such differences were further supported by a direct comparison of clinical features and serologic characteristics in 2 groups of patients from the US and France: anti-RNAP I–III were reported to be more frequent (25% vs 4%) in American patients, as was occurrence of SRC (9% vs 2%)11.
In our multicenter retrospective analysis we investigated characteristics of Italian patients with SSc who developed SRC, with a particular interest in determining their serologic profile.
MATERIALS AND METHODS
Patients
We performed a multicenter retrospective study on patients with SSc from 9 tertiary referral centers in Italy. We reviewed medical records of patients observed between 1987 and 2007. Included patients satisfied the LeRoy criteria for SSc12 and had a diagnosis of SRC defined as abrupt onset of renal failure with or without accelerated/malignant arterial hypertension4. SSc onset was regarded as the first non-Raynaud symptom attributable to the disease. The extension of their cutaneous involvement was classified as limited cutaneous (lcSSc) or diffuse (dcSSc) according to LeRoy, et al12. Pulmonary involvement was defined as presence of bibasilar fibrosis on standard chest radiographs and/or restrictive lung disease on pulmonary function tests (PFT) and/or pulmonary hypertension, as described9. Presence of microangiopathic hemolytic anemia (MAHA) was diagnosed if anemia was associated to schistocytes or other erythrocyte fragments on blood smear, and to increased reticulocyte count.
A total of 51 patients with SRC were identified, and for 46 of them there were enough clinical data and a serum sample available at the time of SRC for laboratory assays. Sera had been stored at −70°C by each participating unit until sent to the single center where serologic investigations were performed simultaneously.
Autoantibodies
Tests for ANA, anti-extractable nuclear antigens (ENA), and anti-RNAP determination were conducted simultaneously on all serum samples. ANA were investigated by indirect immunofluorescence on HEp-2 cells (Diamedix Co., Miami, FL, USA) with serum diluted 1:80. ACA were identified from their ANA pattern (centromeric). Other auto-antibody specificities, including anti-topo I, anti-SSA/Ro, anti-SSB/La, anti-Sm, anti-RNP and anti-Jo1, were evaluated using commercial kits (EliA test) according to the manufacturer’s recommendations (Phadia, Freiburg, Germany).
Anti-RNAP antibodies were tested in patients’ sera by an immunoenzymatic kit for anti-RNAP III (MBL, Nagoya, Japan) as described13. The results were confirmed by immunoprecipitation (IP) assay with 35S-methionine-labelled HeLa cell extracts, as described10.
Statistical analysis
SPSS Software for Macintosh (SPSS Inc., Chicago, IL, USA) was used. Continuous values are expressed as mean ± standard deviation or median (range) according to the variable distribution. Categorical variables are expressed as absolute number or percentage. Continuous variables have been arranged in categories by the median values of their distribution. Student t test, analysis of variance, or Mann-Whitney U test were performed when appropriate to evaluate differences between groups for quantitative variables. Posthoc comparisons were evaluated with the Bonferroni correction when variance between groups was homogeneous. When appropriate, categorical parameters were compared by chi-square test or by Fisher’s exact test. Cumulative survival rates were obtained by Kaplan-Meier method, and differences between groups and between group stratifications were compared by log-rank test, with correction for each stratum when needed. Univariate and bivariate analyses of survival were obtained using the Cox regression model. For all variables in the study, a 2-tailed p value < 0.05 was considered statistically significant.
RESULTS
Patient characteristics
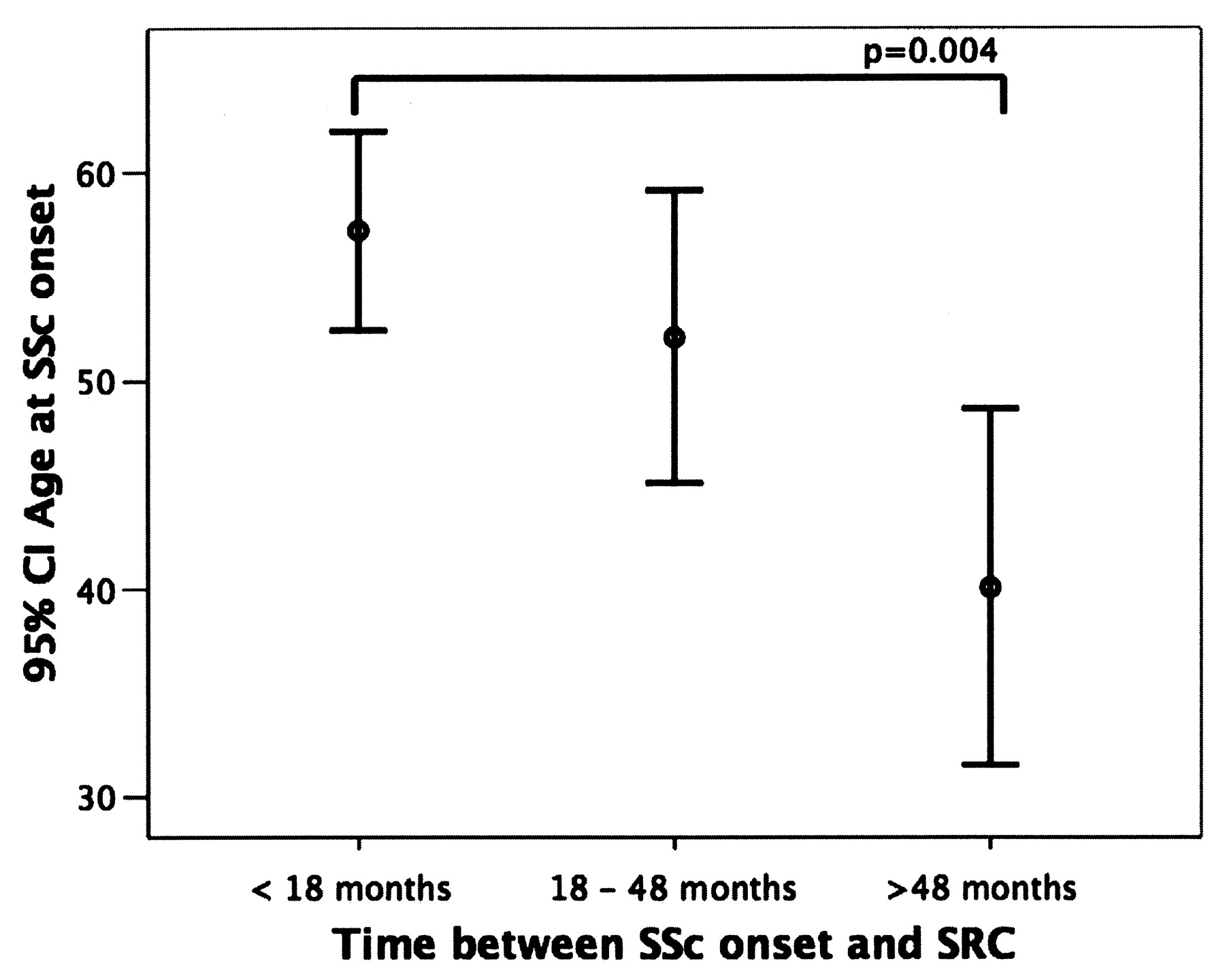
Demographic and clinical characteristics of patients are listed in Table 1. We categorized patients into those presenting with SRC within 18 months of disease onset, between 18 and 48 months, and after 48 months. Sixty-two percent of SRC cases occurred within the first 18 months, 18% between 18 and 48 months, and 20% presented more than 48 months after SSc onset. Patients with SRC occurring early (< 18 mo) had a significantly older age (57.2 ± 12 yrs) versus patients developing SRC later than 48 months in the disease course (40.2 ± 11.9 yrs) (p = 0.004; Figure 1). Accordingly, age > 54 years at SSc onset was significantly associated with SRC occurring within 18 months (p = 0.002). The same trend, albeit not statistically significant, was observed for age at SRC onset between different groups (57.8 ± 11.9 years in cases within 18 months vs 48.1 ± 11.4 years in cases occurring after 48 months; p = 0.92). No other clinical features besides age were found to distinguish patients with early- and late-onset SRC.
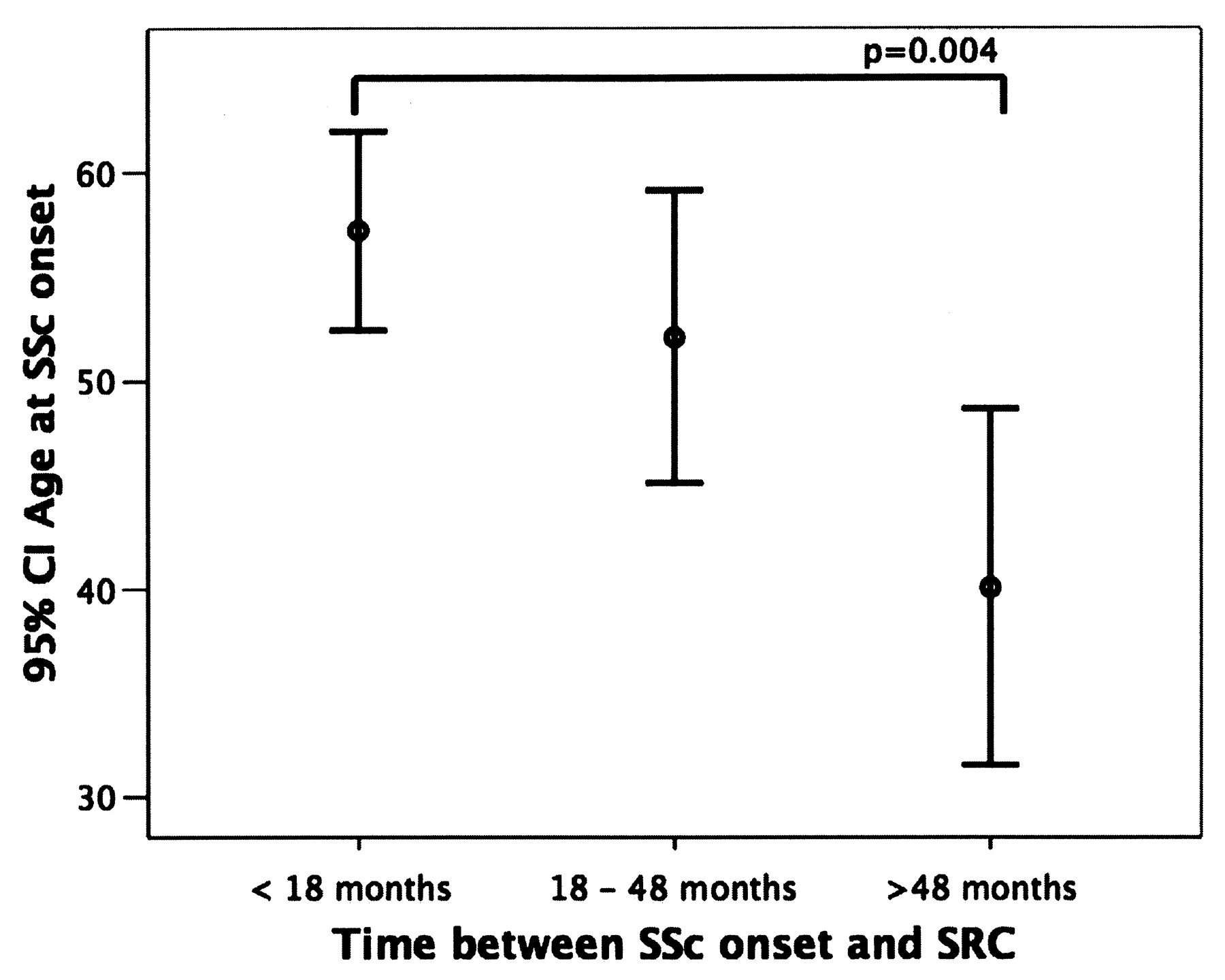
95% CI error bars for age at onset of systemic sclerosis (SSc) showing development of earlier scleroderma renal crisis (SRC) in patients with late-onset SSc. The mean age of the group developing SRC within 18 months of onset of SSc was significantly greater than that of the group developing SRC more than 48 months after SSc onset.
Main demographic features of patients. Data are mean ± standard deviation or median (range) when appropriate.
Renal biopsy, performed in only 5 patients, showed pathologic changes typical of SRC, such as intimal cell proliferation, intravascular fibrin thrombi, mesangiolysis, and glomerular and tubular ischemic features.
SRC treatment data were available for only 42 patients. Among them, 33 (78%) received angiotensin-converting enzyme (ACE) inhibitors as soon as SRC diagnosis was established; 26 (62%) required dialysis. Dialysis regimen was discontinued in 7/26 (27%) patients. Three patients (7%) received renal transplants after a mean followup of 140 ± 54 months after SRC. They had immediately been treated with ACE inhibitors and had undergone peritoneal dialysis. They were alive at the end of the study and showed recovered renal function after transplant. One developed isolated pulmonary hypertension and was started on nonselective endothelin-1 receptor antagonist therapy.
Information regarding therapy before SRC was available for 28 patients: 12 patients were taking low-dose steroids (< 15 mg/day prednisone or equivalent) at the time of SRC; only 5 received low-dose ACE inhibitors.
The cumulative survival rates at 1, 2, 5 and 10 years were 64%, 53%, 40%, and 35% respectively. Univariate analysis showed that survival was significantly affected by age at SRC development, use of steroids prior to the crisis, and prompt administration of ACE inhibitors after the crisis, but not by other known clinical characteristics such as sex, age at SSc onset, type of cutaneous disease, presence of a pulmonary involvement, or prior ACE inhibitor use. Age > 56 years conferred a hazard ratio (HR) of 2.6 (95% confidence interval 1.1–6, p = 0.025); steroids before crisis showed a HR of 3.061 (95% CI 1.155–8.1, p = 0.024), while prompt treatment with ACE inhibitors had a protective role (HR 0.255, 95% CI 0.07 – 0.934, p = 0.039).
Autoantibody profile
ANA were positive in 44 patients (96%) and anti-ENA or anti-RNAP III were positive in 39 (85%). ANA pattern was speckled in 25/44 patients (57%), nucleolar in 10/44 (23%), homogeneous and nucleolar in 8/44 (18%), homogeneous in 1/44 (2%). An isolated nucleolar ANA pattern with no other serological specificities was detected in 4/44 patients (9%).
IP and ELISA for anti-RNAP III gave concordant results: in particular, all patients with a positive ELISA test for anti-RNAP III showed a reactivity in IP for the subunits I–III of the enzyme. Autoantibody profiles were represented by anti-topo I, found in 30/46 patients (65%); anti-RNAP I–III, in 7/46 (15%); and anti-Ro/SSA, in 4/46 (9%). In one case anti-Ro/SSA were associated with anti-topo I and in another one with anti-RNAP I–III.
Characteristics of the anti-topo I and anti-RNAP I–III-positive subsets
We compared demographic and clinical features of patients from the 2 most common serological groups. There was no statistically significant difference between anti-topo I and anti-RNAP I–III-positive patients for the age at SSc onset and at the time of SRC. All patients with anti-RNAP I–III developed SRC within 18 months, and in 2 out of 7 cases SRC was the presenting feature of SSc. In the anti-topo I-positive group the onset of SRC occurred within 18 months of disease in only 15 (50%) cases (p = 0.03) and was the presenting feature in none. In this same group, 7 (23%) patients developed SRC between 18 and 48 months, and 8 (27%) after 48 months.
All patients in the anti-RNAP I–III group presented with hypertensive renal crisis, while in the anti-topo I group 12 patients (40%) had a normotensive-type crisis. Mean initial creatininemia was slightly higher in the anti-topo I-positive patients (4.9 ± 2.6 mg/dl) than in the anti-RNAP I–III group (3.6 ± 0.9 mg/dl). No patient among those whose information was available (n = 4) in the anti-RNAP I–III group and 8/18 (44%) patients in the anti-topo I group showed presence of MAHA (all p nonsignificant).
All anti-RNAP I–III-positive patients had diffuse cutaneous involvement, while in the anti-topo I-positive group there were 3 (10%) patients with limited cutaneous disease. Pulmonary involvement was detected in 18 out of 30 anti-topo I patients (60%) and in 3 out of 7 anti-RNAP I–III patients (43%). There was no significant difference between the 2 serological groups for mean forced vital capacity (anti-RNAP I–III 85% ± 25% vs anti-topo I 85% ± 26%) and mean carbon monoxide diffusing capacity (anti-RNAP I–III 77% ± 19% vs anti-topo I 65% ± 26%), both expressed as percentage of the predicted value (all p = NS).
Data on prior steroid or ACE inhibitor use were available for 7 patients in the anti-RNAP I-III group and for 18 of the anti-topo I-positive patients. Two of the 7 (29%) anti-RNAP I–III patients and 8 of the 18 (44%) anti-topo I patients received low-dose steroids. No one in the anti-RNAP I–III group and 5 (28%) patients in the anti-topo I group had been treated with ACE inhibitors before SRC (all p = NS). Also, no statistically significant difference was found for the proportions of patients receiving prompt ACE inhibitor treatment for SRC in the 2 groups.
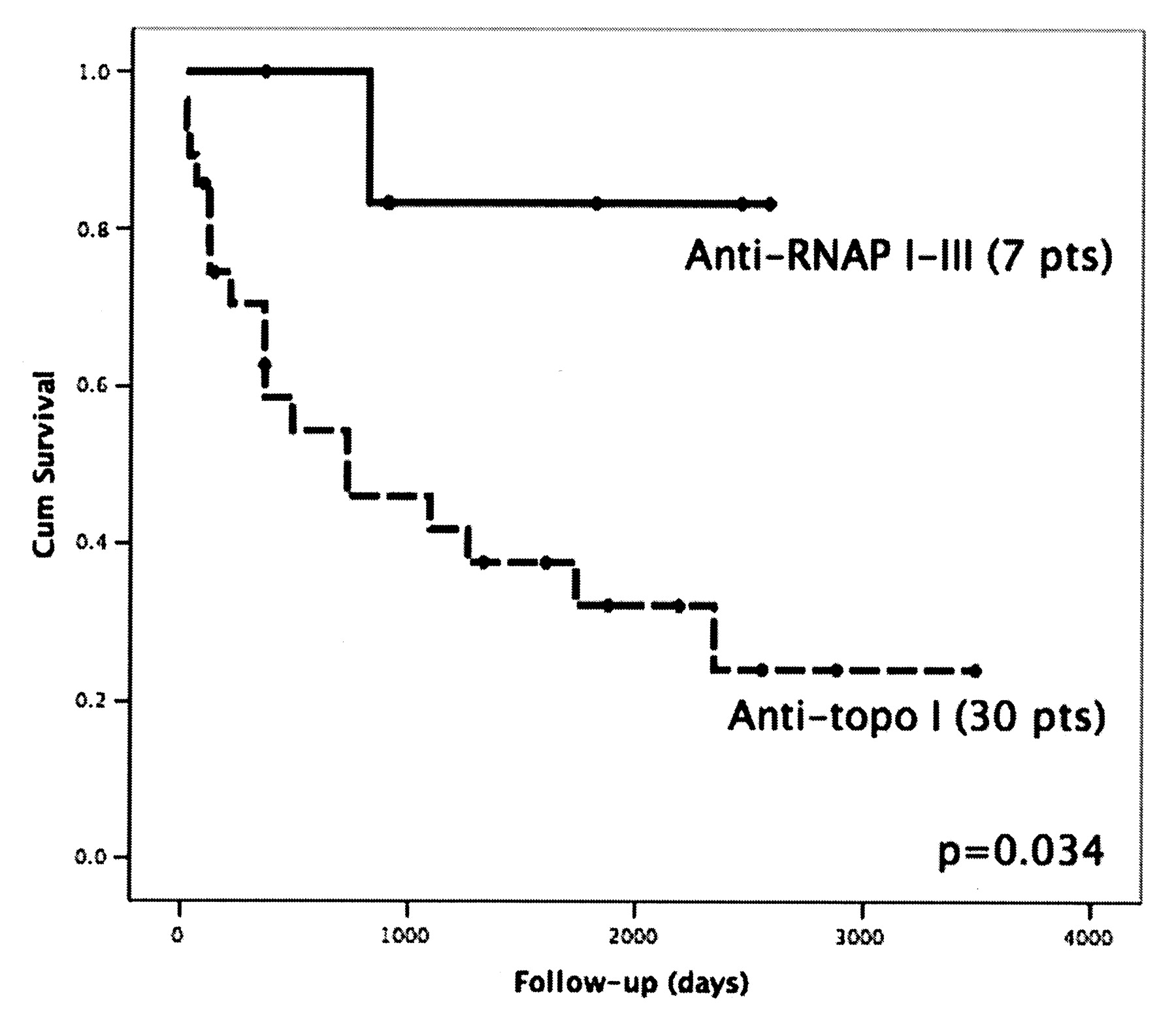
At 5 years of followup, cumulative survival of anti-RNAP I–III-positive patients was 86% versus 32% in the anti-topo I group, with a median survival time of 730 days (p = 0.034; Figure 2). This difference also emerged after adjustment for steroid use before (p = 0.039) or ACE inhibitor use after SRC crisis (p = 0.05). Analyzing only those subjects who did not receive steroids, survival at 5 years was 100% in anti-RNAP I–III patients and 33% in anti-topo I patients. Analogously, considering only those patients treated for SRC with ACE inhibitors, the 5-year survival rate was 83% in the anti-RNAP I–III group and 27% in the anti-topo I group.

Kaplan-Meier curves of patients with scleroderma renal crisis grouped according to their autoimmune profile, i.e., anti-RNA polymerases (RNAP) I–III and anti-topoisomerase (topo) I. The survival rate was significantly higher in the patients who were anti-RNAP I–III-positive.
Stratifying patients for their cutaneous involvement, the cumulative survival rates for anti-topo I-positive dcSSc patients decreased further to 14% at 10 years, values again significantly lower than those in the anti-RNAP I–III-positive dcSSc patients (p = 0.013).
Differences in survival rates were not related to later onset of SRC in the anti-topo I group with respect to anti-RNAP I–III-positive patients, who all developed SRC within 18 months. Survival in anti-topo I dcSSc patients developing SRC within the first 18 months (n = 13) was significantly lower (25% at 5 years; p = 0.04). Accordingly, no significant changes were observed for anti-topo I-positive patients when a distinction was made for those with SRC onset within the first 18 months (31% at 5 years) versus patients with a later onset (30% at 5 years; Figure 3). In our series of patients, either type of cutaneous involvement or presence of pulmonary involvement did not significantly affect survival.

Kaplan-Meier curves of patients who were anti-topoisomerase (topo) I-positive subdivided according to time of onset of scleroderma renal crisis (≤ 18 or > 18 months).
DISCUSSION
In this Italian study on SRC, we found a high percentage of anti-topo I-positive patients who had a reduced survival rate compared to anti-RNAP I–III-positive patients.
We were not able to estimate the prevalence of SRC because of the retrospective design of our data collection. Nevertheless, the limited number of SRC cases collected supports previous observations of a rather low prevalence of SRC in Italian patients with SSc9,14. The main clinical characteristics of our study patients do not seem to diverge from those observed in other countries, except for a slightly lower frequency of lcSSc than that reported in a British cohort15–17. It has been shown that SRC occurs in most patients within 4 years5. In our series, 80% of patients underwent SRC within 4 years and, in particular, all the anti-RNAP I–III-positive patients experienced SRC within 18 months. Interestingly, after categorizing patients by these 2 time-points, it emerged that patients with early-onset SRC had an older age at onset of SSc versus patients with a longer disease course at time of SRC. On the basis of this result a very close clinical monitoring is warranted, including blood pressure and renal function, in patients with early SSc, especially in the elderly.
An important issue emerges from analysis of the auto-antibody profile of our patients. In Italian patients with SRC the frequency of anti-RNAP I–III antibodies (15%) is comparable to non-SRC dcSSc patients10, but it seems lower than British SRC patients (59%)17. Thus, anti-RNAP I–III do not seem to be specifically associated with SRC in our country, although this association is somewhat difficult to evaluate because of the rarity of this autoantibody in our series, which is indeed reflected by the small number of patients with anti-RNAP I–III-associated SRC in our country9,10. These results are in line with the finding that autoantibody frequencies vary in patients from different geographic areas, and strengthen the hypothesis of a decreasing north-south gradient for the prevalence of anti-RNAP in Europe, a feature also suggested for SRC itself10,11. Accordingly, 65% of the patients with SRC described in our study were positive for anti-topo I antibodies versus only 17% of the British series. This difference could be explained in part by the reported higher prevalence of anti-topo I in Italian patients with respect to Caucasian patients from the US and UK10,18,19. An important percentage (9%) of patients in our series displayed anti-Ro/SSA. These data are consistent with a study in British SSc patients that described anti-Ro/SSA to be associated with renal involvement in SSc20. Nevertheless, the lack of specificity of anti-Ro/SSA reactivity and its presence along with other autoantibodies makes this association difficult to establish.
The general cumulative survival rates in our series are slightly lower than those described in other studies from the US and France4,16. Interestingly, when a stratification is done on the basis of the autoantibody profile, results show that these differences are due to the higher mortality rate in the anti-topo I-positive patients, who also represent the majority of our cases. The different trend between these serologic groups is also the result of excluding from the survival analysis those subjects in our study with onset of SRC before the early 1990s who were not reported to be promptly treated with ACE inhibitors, an approach that has since dramatically changed the outcome of this complication4,21.
When compared to the anti-RNAP I–III group, anti-topo I patients showed a significantly later onset of SRC. Half of the patients from our anti-topo I-positive series developed renal crisis after 18 months of disease course, and 23% after 4 years. However, a delayed onset of SRC is not per se associated with a poor prognosis, and other distinctive factors in this group should be investigated. Yet again, this observation underscores the need for physicians to continuously follow up on patients’ renal function and blood pressure during the course of disease to promptly identify this renal complication and to initiate appropriately aggressive treatment immediately on diagnosis.
Possible explanations for the different survival findings in the 2 serological groups analyzed could also be the seemingly different presentations of patients in these subsets. In our study anti-RNAP I–III patients all displayed an acute course (within a short time after disease onset, hypertensive-type crisis), which is reported to be associated with more favorable prognosis15–17, while the clinical picture in anti-topo I-positive patients was likely masked by the normotensive-type crisis, which might have delayed diagnosis and treatment, and may also have been favored by steroids, whose negative role in SRC has been clearly established16.
The main limitations of our study are the lack of detailed clinical data regarding other organ involvement, which could have been a critical factor explaining the different outcomes, and the limited data on therapy. The multicenter and retrospective design explains the difficulty in collecting complete information. These issues also influenced the strength and significance of the statistical analysis in evaluating clinical differences between the 2 main serological groups and in the combined estimate of risk factors. Nevertheless, our data strongly support the high relevance of autoantibodies in SSc as useful prognostic tools in clinical practice and their strong contribution to patient subsets and stratification in the event of SRC.
Despite a dramatic decrease in SRC-related mortality in patients with SSc in recent decades21, survival in patients who develop SRC remains lower than that expected in SSc patients without SRC8,22. Our data support the view that anti-RNAP I–III-positive SRC, which is more frequent in the US and UK, is associated with a quite favorable outcome, while the anti-topo I-positive SRC subset, the most common in our series, is associated with a severe prognosis. Larger prospective studies are needed to identify factors and comorbidities accounting for such a high mortality rate in anti-topo I-positive patients with SRC.
Footnotes
- Accepted for publication February 23, 2009.








{kind=link}
{kind=link}
{kind=link}