

Abstract
Objective. We evaluated endothelin (ET)-1 plasma levels and some clinical measures in patients with primary Raynaud’s phenomenon (PRP), and in patients with systemic sclerosis (SSc) and secondary RP (SRP), in the latter according to their different nailfold videocapillaroscopy (NVC) patterns of microangiopathy (early, active, and late).
Methods. Ninety-nine patients with SSc, 49 with PRP, and 45 control subjects were studied. NVC was performed in all patients to distinguish the pattern of microvascular damage, and the morphological alterations were scored by a semiquantitative rating scale. ET-1 plasma levels were evaluated in all individuals by ELISA.
Results. ET-1 plasma levels were significantly higher (p = 0.001) in patients with both PRP and SRP, compared to controls. A significant positive correlation (p = 0.03) was found between ET-1 plasma levels and SRP duration, but not between ET-1 plasma levels and PRP duration. Significant correlations were observed in patients with SSc between ET-1 plasma levels and clinical measures (e.g., digital ulcers), as well as the score value of single NVC measures, such as the number of capillaries, “ramified” capillaries, and enlarged capillaries (p < 0.05). Finally, the highest ET-1 plasma levels were found in patients with SSc showing the late pattern of microangiopathy when compared to the early pattern (p = 0.03) and to controls (p = 0.003).
Conclusion. Highest ET-1 plasma levels were detected in the more advanced stage of the SSc microangiopathy, namely the late NVC pattern, characterized by capillary loss and increased tissue fibrosis; this might support the involvement of ET-1 in the progression of the microvascular/fibrotic SSc damage.
Clinical criteria have been suggested in order to distinguish between patients with primary Raynaud’s phenomenon (PRP) and those with secondary disease-associated Raynaud’s phenomenon (SRP)1–3. RP represents the early clinical feature of vascular involvement in systemic sclerosis (SSc), and it is at least partially related to the function of the endothelial cells1,4.
Autoimmune inflammation, vascular injury, and excessive fibrosis are the major features of the disease process leading to irreversible organ damage and significant morbidity in patients with SSc5. Among the key molecular mediators that have potential to be involved in vascular processes, endothelin (ET-1) plays an important role by causing vascular endothelial cell proliferation, enhanced vasoconstriction, smooth muscle hypertrophy, and irreversible vascular remodeling in the lungs6–8. Further, ET-1 was shown to promote fibroblast synthesis of collagen types I and III by a receptor-dependent mechanism, and increased ET-1 production has been found by fibroblasts derived from patients with SSc8–10. Elevated plasma levels of ET-1 have been found in patients with PRP and with SRP11–15.
SSc microvascular damage, which develops years before other symptoms in early SSc, is characterized by recognized structural alterations of the capillaries. It may be evaluated by nailfold videocapillaroscopy (NVC), which is considered to have both diagnostic and prognostic value in the presence of isolated RP also2,16–24. At least 3 different patterns of microvascular damage have been described using NVC in patients with SSc — “early,” “active,” and “late”22,25.
The major aim of our study was to evaluate ET-1 plasma levels, as well as some clinical measures, in patients with PRP and SRP, and to correlate ET-1 levels with the different patterns of microangiopathy, as detected by NVC, in patients with SSc.
MATERIALS AND METHODS
Study population
One hundred ninety-three patients were enrolled into the study. Ninety-nine patients had SSc (90 women, 9 men; mean age 60 ± 12, range 18–77 yrs; mean RP duration 13 ± 13 yrs; mean SSc duration 6 ± 8 yrs) and 49 patients had PRP (40 women, 9 men; mean age 46 ± 18, range 18–77 yrs; mean RP duration 6 ± 10 yrs). Forty-five sex-matched subjects were enrolled as controls (36 women, 9 men; mean age 53 ± 15, range 25–77 yrs). The controls were recruited from the Rheumatologic Outpatient Clinic, referred for localized soft tissue diseases (mainly soft tissue painful conditions).
The patients were consecutively recruited from the Videocapillaroscopy Service for the Diagnosis of Vascular and Connective Tissue Diseases at the University of Genova, and informed consent was obtained from all patients. Patients with scleroderma met the criteria for SSc, or the criteria for the classification of early SSc2. Seventy-five patients had limited cutaneous SSc (lcSSc; skin involvement of the fingers, hands, forearms, toes, feet, legs, neck, and face), and 24 showed diffuse cutaneous SSc (dcSSc; skin involvement of arms, thighs, chest, abdomen, and back)26. All patients with SSc had SRP, and no concomitant serious systemic diseases other than SSc were found.
Diagnosis of PRP was achieved by the occurrence of symmetric attacks of vasospasm, absence of tissue ulceration, absence of an underlying disease (based on medical history and examination of the patient), absence of antinuclear antibodies (ANA), normal blood findings, and normal nailfold capillaries at NVC examination1,3.
The duration of RP and SSc, at the time of NVC assessment, was evaluated by clinical interview and from clinical file data. In particular, the duration of SSc was calculated from the time of onset of clinical symptoms (different from RP) clearly related to SSc (skin fibrosis, dysphagia, etc.) or from the time of instrumental and/or laboratory investigations confirming the diagnosis (i.e., NVC, esophageal and/or pulmonary involvement, detection of serum autoantibodies). Twenty-seven patients with SSc (28%) showed an early NVC pattern of microangiopathy (mean age 55 ± 14 yrs, mean SRP duration 9 ± 12 yrs, mean SSc duration 6 ± 9 yrs), 43 patients (43%) presented an active pattern (mean age 61 ± 11 yrs, mean SRP duration 13 ± 13 yrs, mean SSc duration 5 ± 5 yrs), and 29 patients (29%) showed a late pattern (mean age 62 ± 10 yrs, mean SRP duration 18 ± 12 yrs, mean SSc duration 9 ± 10 yrs; see below for classification).
The patients with SSc were not treated by immunosuppressors, vasodilators, angiotensin-converting enzyme inhibitors, or calcium channel blockers from the last 2 weeks before blood sample collection.
Nailfold videocapillaroscopy
NVC was performed in each patient using an optical probe videocapillaroscope equipped with magnification 200× contact lens and connected to image analysis software (Videocap, DS MediGroup, Milan, Italy). Each subject was inside the building for a minimum of 15 min before the nailfold was examined and the room temperature was 20–22°C. The nailfolds of the 2nd, 3rd, 4th, and 5th digits were examined in each patient, by the same rheumatologist, after a drop of immersion oil was placed on the nailfold bed to improve the image resolution.
The following capillaroscopic measures were scored, according to previous observations: presence of enlarged and giant capillaries, local hemorrhages, loss of capillaries, ramified capillaries, and disorganization of the microvascular array16,17,21. A semiquantitative rating scale to score each capillary abnormality was adopted, according to previous studies (0 = no changes, 1 = less than 33% of capillary alterations/reduction, 2 = 33–66% of capillary alterations/reduction, 3 = more than 66% of capillary alterations/reduction, per linear mm)16,22,27,28. The capillary number was considered reduced if < 10 capillaries per linear mm at distal row were detected.
Based on the NVC abnormalities, the patients with SSc were distributed into the appropriate NVC pattern of microvascular damage, as described22. The patterns included: (1) early NVC: few giant capillaries (< 4 altered capillaries per mm), few capillary hemorrhages, relatively well preserved capillary distribution, no evident loss of capillaries; (2) active NVC: frequent giant capillaries (> 6 altered capillaries per mm), frequent capillary hemorrhages, moderate (20/30%) loss of capillaries, mild disorganization of the capillary architecture (4–6 altered capillaries per mm), absent or mild ramified capillaries; and (3) late NVC: irregular enlargement of the capillaries, few or absent giant capillaries and hemorrhages, severe (50/70%) loss of capillaries with large a vascular areas, disorganization of the normal capillary array, evident ramified capillaries.
ET-1 assessment
ET-1 plasma levels were evaluated by enzyme-linked immunosorbent assay (ELISA; Biomedica Grouppe, Wien, Austria). The interassay coefficient of variation (CV) was 6.1–6.9%, and the intraassay CV was 3.9–4.9%. The resulting values are reported as fmol/ml [median and interquartile range (IQR)]. Sample collection was performed between 8:00 and 9:00 AM in fasting subjects, and patients were not reporting RP attack during the blood sampling. Blood samples were collected from March to November, and the time that patients spent inside the building to wait for both blood withdrawal and NVC analysis was enough to prevent them from evident RP episodes. The blood collection was performed in the area inside the bend of the elbow, and the blood samples from patients and controls were immediately cold-saved after collection and processed into a refrigerated centrifuge. Plasma samples were stored at −80°C before analysis.
Autoantibody detection
Total ANA, anti-topoisomerase I antibodies (anti-Scl-70), and anticentromere antibodies (ACA) were measured in all patients. ANA were detected by indirect immunofluorescence using human epithelial cell line 2 (HEp-2) cells as substrate (Euroimmun, Luebeck, Germany). Anti-Scl-70 antibodies and ACA were evaluated using an ELISA (Euroimmun).
Statistical analysis
The statistical analysis was carried out by nonparametric tests. Wilcoxon test was performed to compare the paired groups, and Mann-Whitney U-test to compare the unpaired groups of variables. Spearman rank correlation test was performed to assess possible correlations between variables, and the rank correlation coefficient (rho) calculated. The chi-squared test was adopted to evaluate the distribution of different NVC patterns in patient groups with different ET-1 plasma levels. A p value < 0.05 was considered statistically significant.
RESULTS
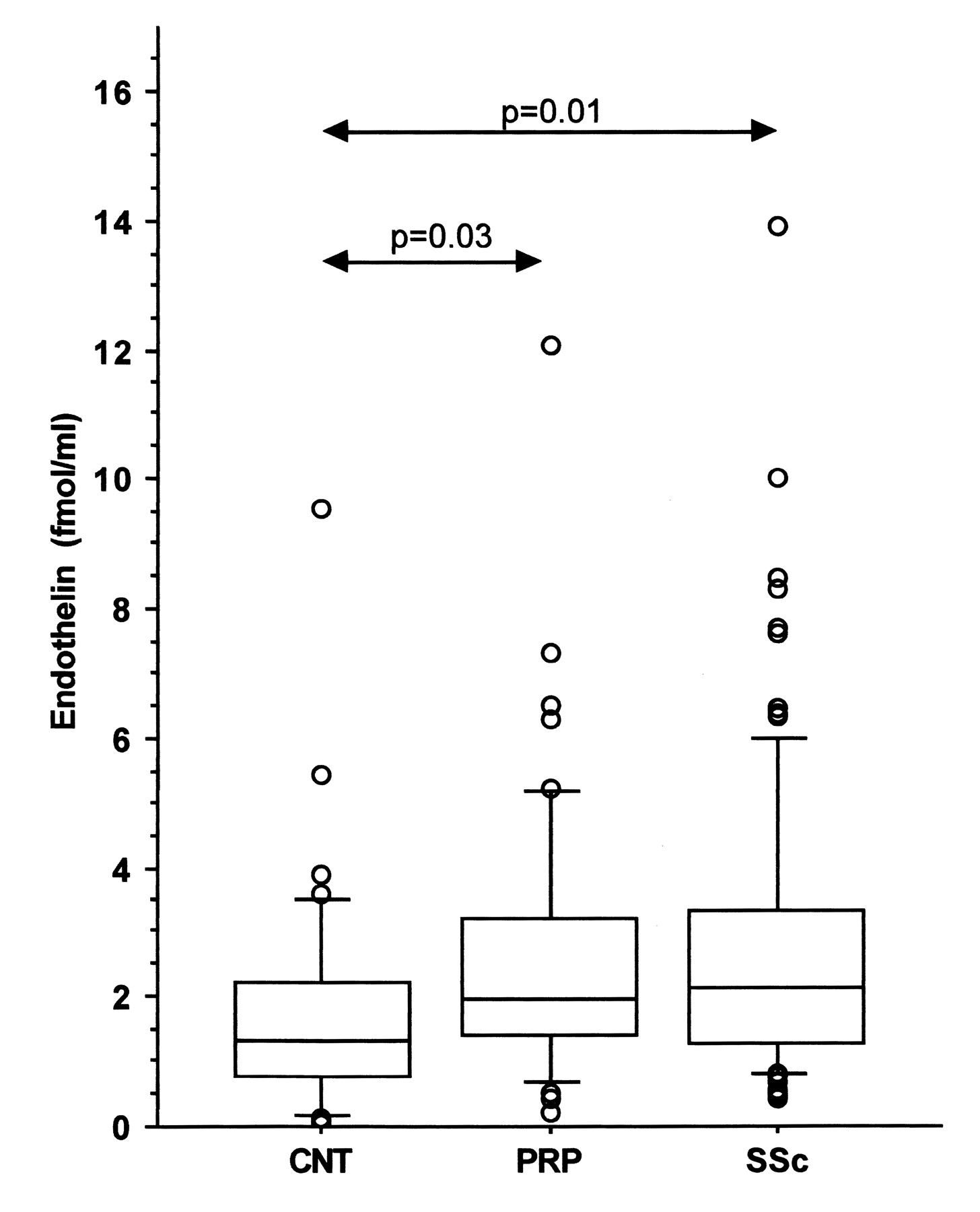
ET-1 plasma levels were found to be significantly higher (p = 0.001) in patients with both PRP and SRP [SSc-associated; median 2.0 fmol/ml (IQR 1.8) and 2.1 fmol/ml (IQR 2.1), respectively], compared with controls [median 1.3 fmol/ml (IQR 1.4)]. No statistically significant difference for ET-1 plasma levels was observed between patients with PRP and SSc (Figure 1).
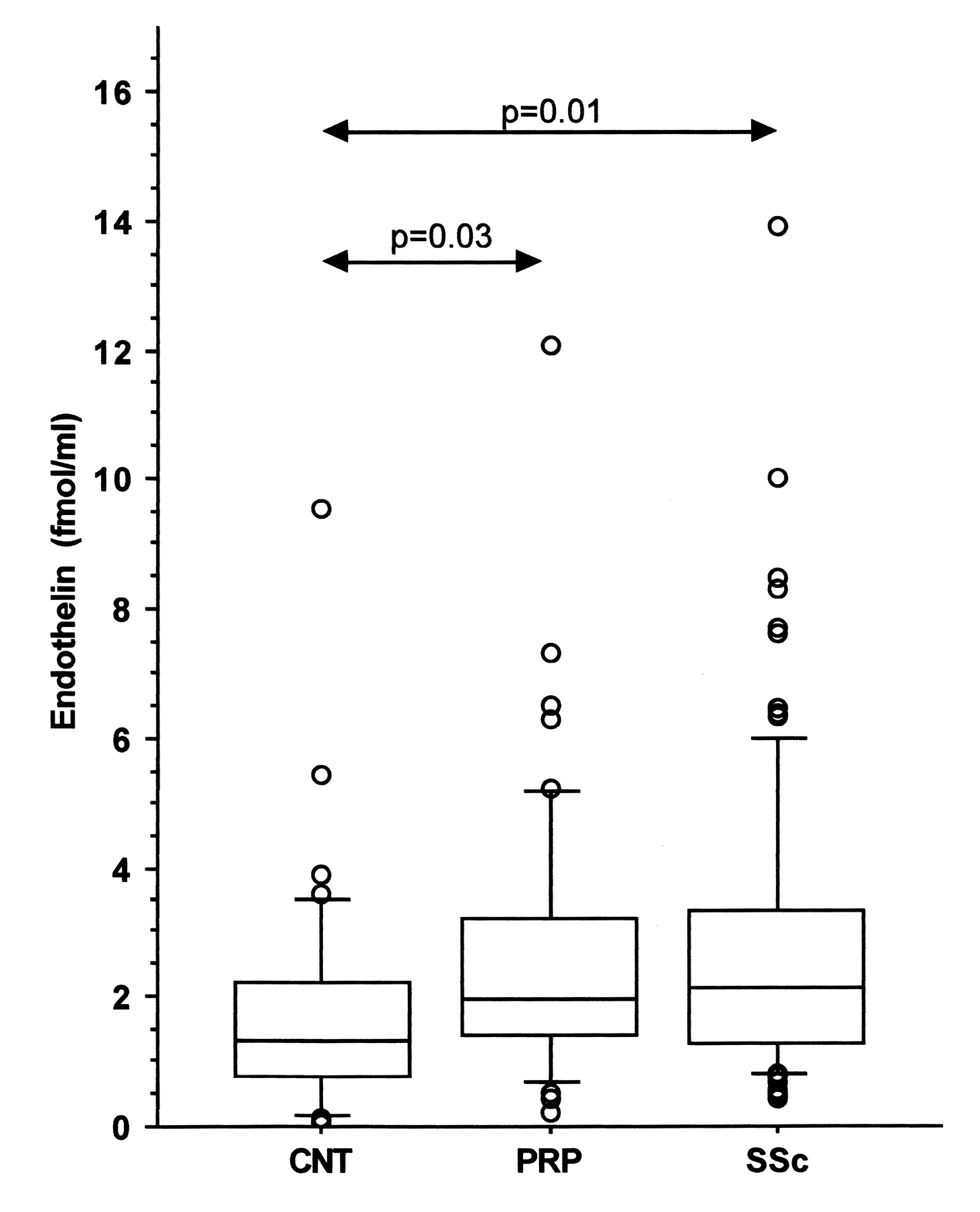
Plasma levels of endothelin-1 in controls (CNT), patients with primary Raynaud’s phenomenon (PRP), and patients with scleroderma-associated secondary Raynaud’s phenomenon (SRP). Box plots show 5th, 10th, 50th (median), 90th, and 95th percentiles.
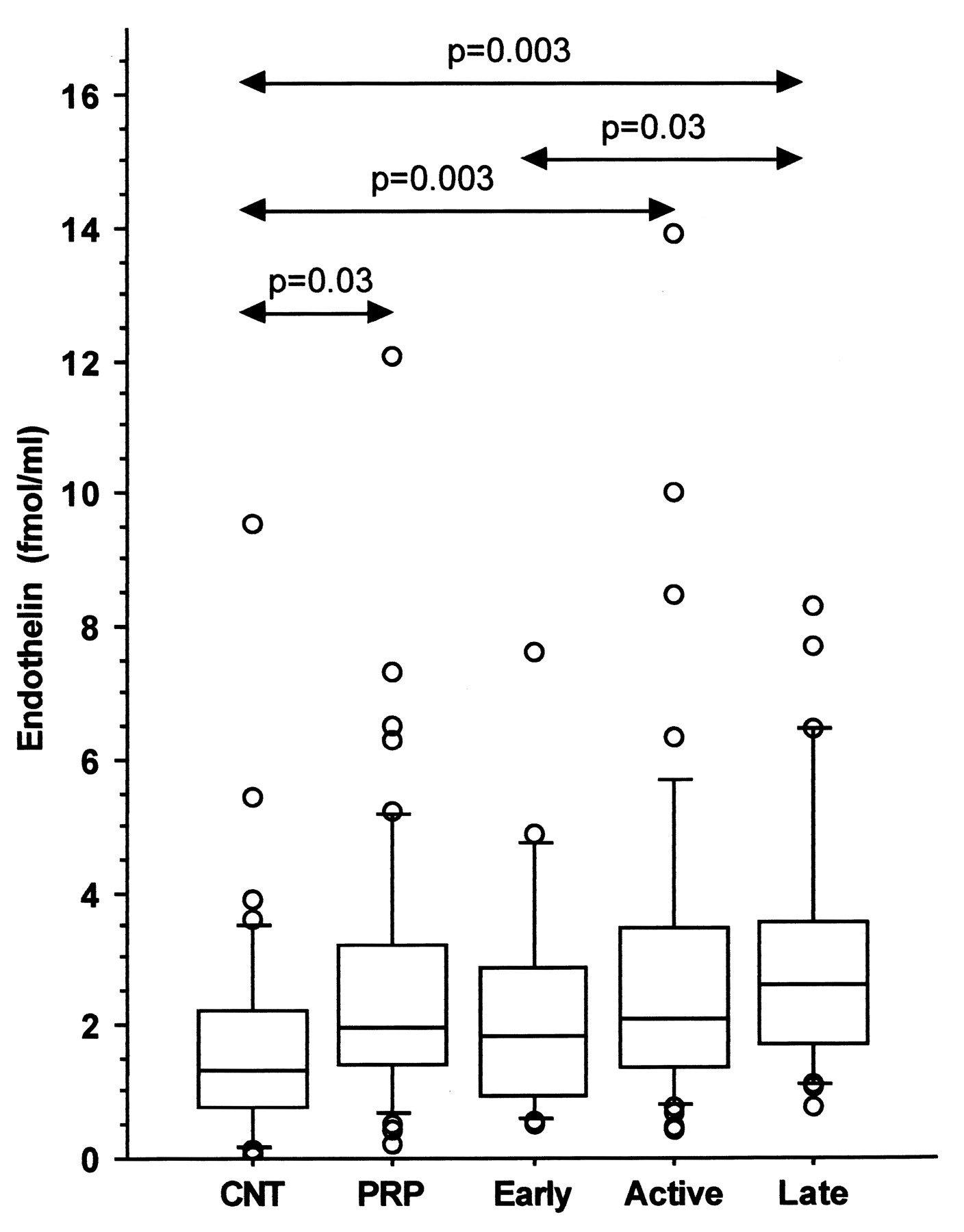
Among patients with SSc showing different NVC patterns of microvascular damage, ET-1 plasma levels were significantly lower (p = 0.03) in patients with the early pattern of microangiopathy [median 1.8 fmol/ml (IQR 1.9)], compared with patients showing the late pattern [median 2.6 fmol/ml (IQR 1.8)]. No statistically significant difference for ET-1 plasma levels was observed between the early and active [median 2.1 fmol/ml (IQR 2.1)] and the active and late patterns of microangiopathy (Figure 2).

Plasma levels of endothelin-1 in controls (CNT), patients with primary Raynaud’s phenomenon (PRP), and scleroderma patients (SSc) with different patterns of microvascular damage (early, active, and late), as assessed by nailfold videocapillaroscopy. Box plots show 5th, 10th, 50th (median), 90th, and 95th percentiles.
The highest ET-1 plasma levels were found in patients with SSc showing the active and late pattern when compared to controls (p = 0.003; Figure 2). No statistically significant difference was observed between patients with PRP and SRP with different NVC patterns of microvascular damage.
No statistically significant difference for ET-1 plasma levels was observed between patients with clinically assessed lcSSc [median 2.1 fmol/ml (IQR 1.8)] and dcSSc [median 2.0 fmol/ml (IQR 1.6)], or between female and male patients [median 2.1 fmol/ml (IQR 0.9) and 2.1 fmol/ml (IQR 2.2), respectively]. However, patients with digital ulcers (active or previous) showed significantly higher ET-1 levels than those without [median 2.4 fmol/ml (IQR 1.2) and 2.1 fmol/ml (IQR 1.8), respectively; p = 0.04].
A significant positive correlation was found between ET-1 plasma levels and duration of SRP (r = 0.22, p = 0.03), but not between ET-1 plasma levels and duration of PRP. Further, significant correlations were found in patients with SSc between ET-1 plasma levels and the score value of some morphological measures of microvascular damage. In particular, a positive correlation was observed between ET-1 plasma levels and number of both ramified and irregularly enlarged capillaries (r = 0.27 and p = 0.02, r = 0.34 and p = 0.01, respectively); and a negative correlation was observed between ET-1 plasma levels and number of capillaries (r = −0.22, p = 0.05). No correlation was found between ET-1 plasma levels and age of patients or duration of SSc, or between ET-1 plasma levels and presence of serum ANA, ACA, and Scl-70 antibodies. Moreover, no statistically significant difference in ET-1 plasma levels was observed between patients with SSc showing different ANA staining patterns (speckled, nucleolar, or homogeneous).
Finally, we observed a positive correlation between duration of SSc and microvascular abnormality scores, including irregularly enlarged capillaries, ramified capillaries, disorganization of the vascular array, and number of capillaries, confirming previous data22.
DISCUSSION
Our study confirms that patients with PRP or SRP/SSc (related to SSc) show higher ET-1 plasma levels than control subjects12,29–31.
Among patients with SSc, we observed significant differences in ET-1 plasma levels in relation to the different severity of microvascular damage: SSc patients with advanced NVC patterns of microangiopathy (late NVC pattern characterized by diffused fibrosis) showed higher ET-1 plasma levels than those with the early pattern.
These results support the hypothesis that increased local ET-1 concentrations may play a complex role in the pathogenesis of both RP and progressive microvascular/fibrotic damage in SSc. The highest ET-1 plasma levels associated with the late pattern of microangiopathy were correlated with more severe clinical involvement, such as skin damage (i.e., digital ulcers), but also with cardiac and lung fibrosis and pulmonary hypertension. Unfortunately, our study was not primarily designed to investigate correlations between single organ involvement and ET-1 levels (already demonstrated in several studies), as its primary aim was only to detect possible correlations between ET-1 plasma levels and the capillaroscopic patterns of microvascular damage in patients with SSc. Our study demonstrated higher ET-1 plasma levels in SSc patients with the late NVC pattern of microangiopathy. A larger study is needed to correlate ET-1 plasma levels, NVC patterns, and single organ involvement.
Interestingly, ET-1, among the strongest endogenous vasoconstrictor mediators, is also recognized as a potent mitogen, and there is experimental evidence to suggest that ET-1 contributes to the vascular remodeling and organ damage in different clinical conditions32. Low oxygen tensions, typical of the ischemic phase of RP, were shown to rapidly increase ET-1 secretion from cultured human endothelial cells 4- to 8-fold above the secretion rate at ambient oxygen tension (transcriptional gene-related)33. Our study confirmed higher ET-1 plasma levels in patients with digital ulcers (active or previous) compared to those without.
The confirmed lack of statistically significant difference in ET-1 plasma levels between patients with PRP and SRP supports the evidence that ET-1 is primarily involved in capillary vasospasm (clinical RP), independently from its association with an underlying connective tissue disease.
ET-1 plasma levels have been described as higher in patients with SSc with ACA, as well as in patients with diffuse SSc29,34,35. In contrast, our study failed to show a statistically significant correlation between ET-1 plasma levels and both ACA positivity and skin involvement subsets of SSc. Patients with ACA are recognized to have more frequently limited disease, therefore the results of these previous studies are difficult to interpret. However, ET-1 was also higher in lcSSc patients with pulmonary hypertension, supporting the fact that several other variables should be considered during the classification of patients with SSc into different disease subsets35.
ET-1 has been found to induce a fibrogenic phenotype in normal fibroblasts, similar to that observed from lesional SSc fibroblasts9. We previously found that NVC patterns correlated positively with the duration of SRP in patients with SSc, reflecting the possible evolution of the microangiopathy and the fibrotic process22. ET-1 plasma levels were significantly higher in SSc patients with the late NVC pattern of microangiopathy, again supporting that ET-1 might be involved in the progression of the SSc microvascular damage, and at the same time it might be involved in the fibrotic progression of the disease. Endothelial cell damage/dysfunction might induce through ET-1 an increased collagen and extracellular matrix synthesis by fibroblasts and consequential fibrosis35. Significantly higher levels of ET-1 and ET-1 mRNA were found in SSc fibroblast cultures than in those of normal fibroblasts, supporting a role for ET-1 in the SSc fibrotic process8. Recently, we showed that ET-1 seems to exert a profibrotic effect in normal and SSc cultured fibroblasts, by increasing the synthesis of fibronectin, strongly suggesting a role in the pathogenesis of the fibrotic process in SSc36. However, as patients with PRP (who notably will not develop fibrosis during the course of the disease) show plasma levels of ET-1 similar to those with SRP/SSc (but lower compared to the late SSc pattern), additional clinical/humoral cofactors should be considered to determine the fibrotic evolution of SSc.
Since none of the patients enrolled in our study was ever treated with endothelin receptor blockers, the possible effects on nailfold capillary patterns induced by treatment with endothelin receptor blockers should be investigated. We previously evaluated the possible modulatory action of longterm vasodilator drugs in SSc patients treated with iloprost for 1 year, and failed to demonstrate capillaroscopic microvascular changes37.
Using NVC, we detected the highest ET-1 plasma levels in patients with the more advanced stage of SSc microangiopathy, namely the late pattern, characterized by capillary loss and increased tissue fibrosis. This might support the involvement of ET-1 in the progression of microvascular/fibrotic damage in SSc disease.
Footnotes
- Accepted for publication January 30, 2009.








{kind=link}
{kind=link}