

Abstract
Objective. This study evaluates possible correlations between the pattern of antinuclear antibodies (ANA) on indirect immunofluorescence (IIF) testing and nailfold microangiopathy stage (early, active, and late stage) in systemic sclerosis (SSc). Patients with SSc were followed prospectively to monitor progression of microvascular damage.
Methods. The ANA pattern on IIF was searched in 42 patients with SSc showing an early pattern of nailfold microangiopathy at baseline, and was followed using nailfold videocapillaroscopy (NVC) for a median time of 91 months.
Results. Among patients whose microangiopathy showed a rapid progression from early to late pattern on NVC, the IIF pattern was fine-speckled + nucleolar (Scl-70+) in 44%, centromeric in 33%, nucleolar in 11%, and homogeneous in 11% of patients with SSc. Antitopoisomerase I antibodies were significantly more frequent (57%) in patients with late pattern of microangiopathy on NVC. The median time of progression from early to active disease was significantly lower in patients with both fine-speckled + nucleolar and nucleolar ANA positivity. The severity of microangiopathy was higher in patients with the nucleolar pattern on IIF. Patients already showing a slight reduction of capillary number at baseline were likely to have either the nucleolar or the fine-speckled + nucleolar pattern on IIF. Of note, 37% of patients still showing the early microangiopathy pattern on NVC at the end of the followup were ANA-negative.
Conclusion. ANA-negative patients with SSc display a slower progression of nailfold microangiopathy characterized by the early pattern on NVC. Progression to the late NVC pattern (more advanced stage of microvascular damage) seems to be associated with a different autoantibody pattern on IIF (fine-speckled + nucleolar pattern being the most prevalent).
- NAILFOLD VIDEOCAPILLAROSCOPY
- SYSTEMIC SCLEROSIS
- MICROANGIOPATHY
- ANTINUCLEAR ANTIBODIES
- INDIRECT IMMUNOFLUORESCENCE
- SCLERODERMA
Nailfold microvascular impairment is an early clinical feature of systemic sclerosis (SSc) and its progression through different patterns of capillary damage, as evaluated by nailfold videocapillaroscopy (NVC), has recently been confirmed by a longitudinal study1. The earliest nonspecific microvascular alteration is the appearance of capillary enlargements greater than 20 μm, which become homogeneously enlarged loops (i.e., giant capillaries, with capillary diameter > 50 μm) that along with pericapillary microhemorrhages represent the first marker of the scleroderma pattern. In this way, statistically significant prognostic values were observed for the presence of giant loops (HR 2.64) and microhemorrhages (HR 2.33) on NVC scans to identify patients complaining of isolated Raynaud phenomenon (RP) and at risk of developing scleroderma spectrum disorder2. Subsequently, nailfold capillary density decreases, and large avascular areas become evident, promoting a compensatory (although disturbed) neoangiogenesis with ramified capillaries and disorganization of the microvascular array3,4. The dynamic modifications of the nailfold microvascular bed, together with expression of different autoantibodies, during the course of SSc was demonstrated by a 20-year prospective study5. The authors reported capillary enlargement as the earliest event, occurring a median of 2.58 years after the onset of RP, whereas capillary loss was noted later, at a median of 4.51 years, followed by capillary telangiectasias and presence of specific antibodies5.
Using NVC results, we described 3 different patterns of nailfold microvascular damage (the early, active, and late stage scleroderma pattern) that mirror the progression of SSc microangiopathy6. The progression from early to active and subsequently to late pattern of microvascular damage was recognized as occurring in 13% of patients with SSc at 7 years1. However, the dynamic transition of the microvascular damage through different NVC patterns of microangiopathy was observed only in about half of patients with SSc at the end of the followup, because 34% of patients were showing active microangiopathy and 47% were still displaying the early pattern1.
The precise factors or events influencing a slower or faster progression of SSc microangiopathy are not yet identified, but several autoantibodies have been described as associated with disease progression and microvascular damage5,7,8,9,10.
Because SSc is an autoimmune disease, the aim of our study was to identify serum antinuclear antibodies (ANA) in patients with SSc who were prospectively followed to monitor progression of nailfold microangiopathy. We also aimed to investigate, to our knowledge for the first time, possible correlations between patterns of ANA assessed by indirect immunofluorescence (IIF) and stages of microangiopathy assessed by NVC.
MATERIALS AND METHODS
Patients
Retrospective data concerning serum autoantibodies were available from 42 patients with SSc [median age 47 yrs, interquartile range (IQR) 19 yrs; median disease duration from onset of RP 5 yrs, IQR 11 yrs; median disease duration from onset of first SSc sign/symptom different from RP 1 yr, IQR 3 yrs] with the early pattern of nailfold microangiopathy at baseline; they had been followed prospectively with NVC scans for a median 91 months (IQR 48 mo). SSc patients with RP and the early NVC pattern, with specific/nonspecific autoantibodies, and/or other related symptoms, entered the study; all met the LeRoy criteria for classification of early SSc11. Patients were consecutively recruited from the Rheumatologic Service for the Diagnosis and Management of Vascular and Connective Tissue Diseases at the University of Genoa from 2001 to 2010. All patients provided written informed consent before enrollment.
Nailfold videocapillaroscopy
NVC was performed in each patient using an optical probe videocapillaroscope equipped with a 200× contact lens and connected to image analysis software (Videocap; DS MediGroup). NVC examination was performed by the same operator (CP) every 6 months during followup. Each subject was inside the building a minimum of 15 min before the nailfold was examined, and the room temperature was 22°–23°C. Nailfolds of second, third, fourth, and fifth digits were examined in each patient; a drop of immersion oil was placed on the nailfold bed to improve image resolution.
The first line of capillaries at the nailfold was evaluated, and the following capillaroscopic measures were considered, according to previous observations: presence of enlarged and giant capillaries, hemorrhages, loss of capillaries, disorganization of the microvascular array, and capillary ramifications3. These variables were defined as described6,12.
A semiquantitative rating scale was adopted to score each capillary abnormality, in accord with previous studies (0–3 score for each variable: 0 = no changes, 1 = less than 33% of capillary alterations/reduction, 2 = 33%–66% of capillary alterations/reduction, 3 = greater than 66% of capillary alterations/reduction, per linear millimeter). The microangiopathy evolution score (sum of 3 scores for loss of capillaries, disorganization of microvascular array, and capillary ramifications) was also calculated to globally assess the progression of vascular damage6,13,14.
With regard to nailfold capillary abnormalities, patients were classified according to the early, active, or late microangiopathy pattern, as described6,12.
Autoantibody detection
The ANA pattern was evaluated yearly in all patients during the followup, by IIF, using HEp-2 cells (Euroimmun) as substrate; serum dilution (titer) ≥ 1:160 was considered positive. Antitopoisomerase I antibodies (Scl-70) were investigated in all patients by ELISA (Euroimmun). ANA centromeric IIF was confirmed by detecting anticentromere antibodies (ACA) by ELISA, as for Scl-70. No other SSc-specific autoantibodies were tested.
Statistical analysis
Chi-square test was used to investigate differences of distributions of categorical variables; Fisher exact test was employed when appropriate. Survival curves were estimated using the Kaplan-Meier method and compared using log-rank test. Mann-Whitney U and Kruskal-Wallis tests were performed to compare the unpaired groups of variables. Multiple regression analysis was used to investigate progression of nailfold capillary patterns in relation to both subsets of SSc skin involvement and ANA patterns on IIF. The p values < 0.05 were considered statistically significant.
RESULTS
At the end of followup (median 91 mo), the NVC pattern of microangiopathy had changed in 23 patients with SSc (55%), while 19 patients (45%) still showed the early scleroderma pattern. In particular, the NVC pattern became active in 14 patients (33%), and late in 9 (21%). The median period of progression from the early to the late NVC pattern was 76 months. Interestingly, the median period of progression from the early to the active NVC pattern was 20 months in all patients, and only 8 months in patients with SSc who progressed to the late NVC pattern. In this latter group, the median time of progression from active to late pattern on NVC was 38 months.
Concerning ANA positivity measured by IIF, in 9 patients whose microangiopathy showed a progression from the early stage, through the active pattern, to the late NVC pattern, the IIF pattern was determined to be fine-speckled + nucleolar (and Scl-70-positive) in 4 patients (44%), centromeric (ACA-positive) in 3 patients (33%), nucleolar in 1 (11%), and homogeneous in 1 (11%). Scl-70 positivity was associated with a fine-speckled + nucleolar positivity in all patients with SSc.
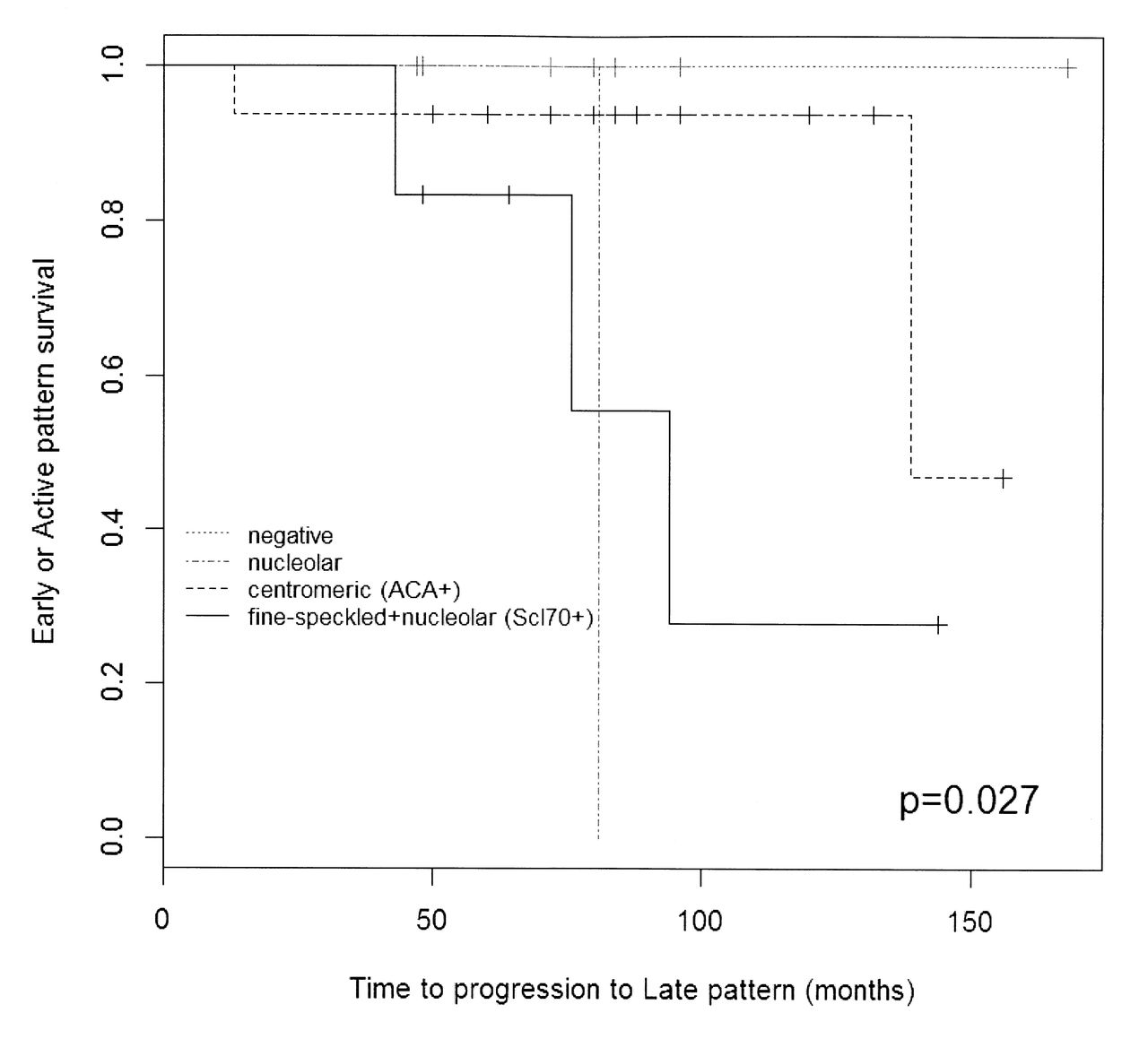
Survival curves for NVC pattern related to ANA IIF patterns were estimated using the Kaplan-Meier method, shown in Figures 1 and 2. The median time of survival of early to late stage NVC pattern was 94 months for the fine-speckled + nucleolar (Scl-70+), 139 months for the centromeric, and 81 months for the nucleolar ANA pattern on IIF. Of interest, the median time of survival from early to active disease pattern considering the ANA IIF evidence was significantly different: it was 10 months in the fine-speckled + nucleolar (Scl-70+) patient group, 48 months in the centromeric group, and 8 months in the nucleolar group (p = 0.006).
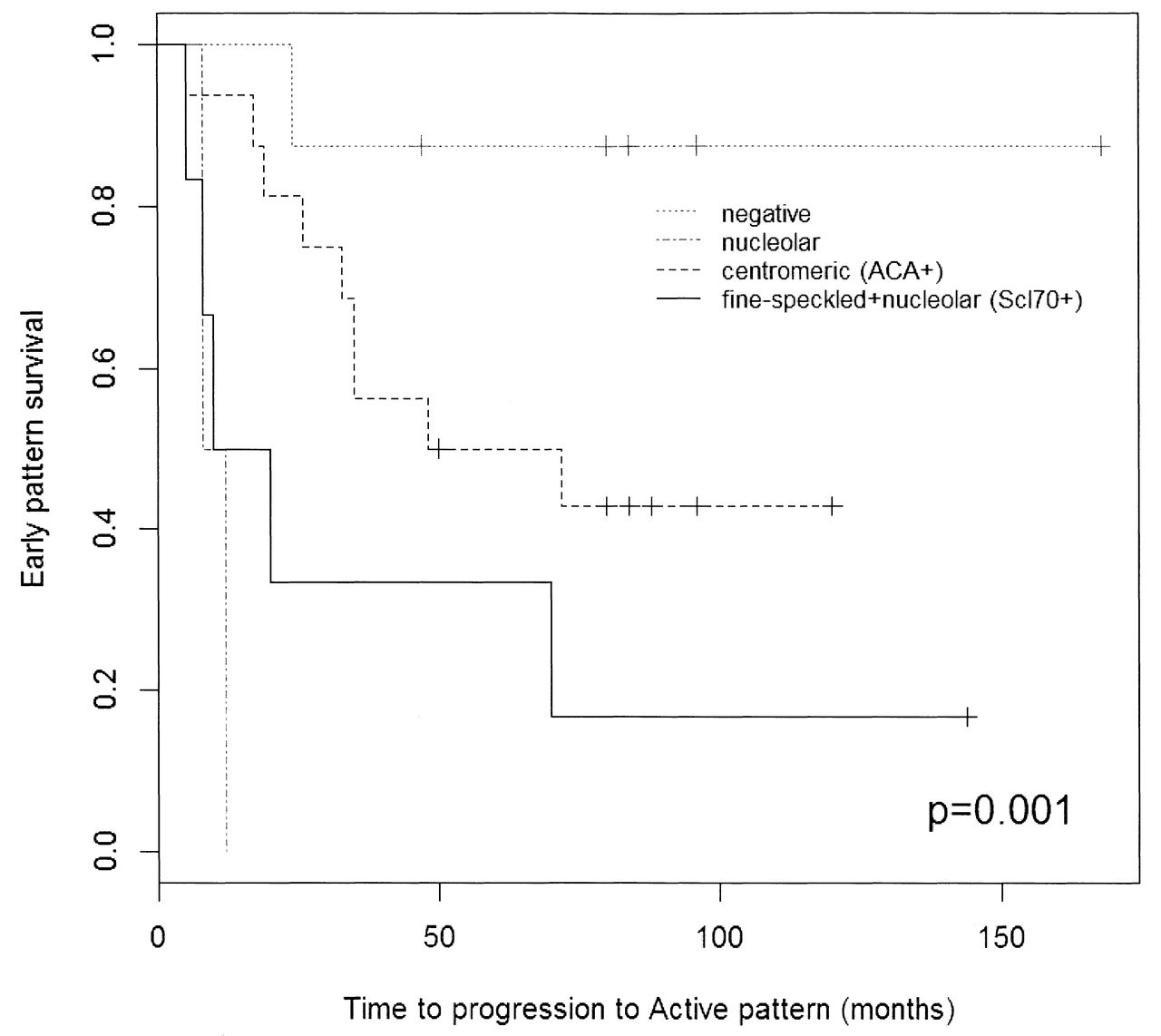
Kaplan-Meier plot shows survival probability of early stage disease determined by nailfold videocapillaroscopy pattern, in relation to different antinuclear antibodies measured by indirect immunofluorescence. ACA: anticentromere antibodies; Scl-70: antitopoisomerase I antibodies.
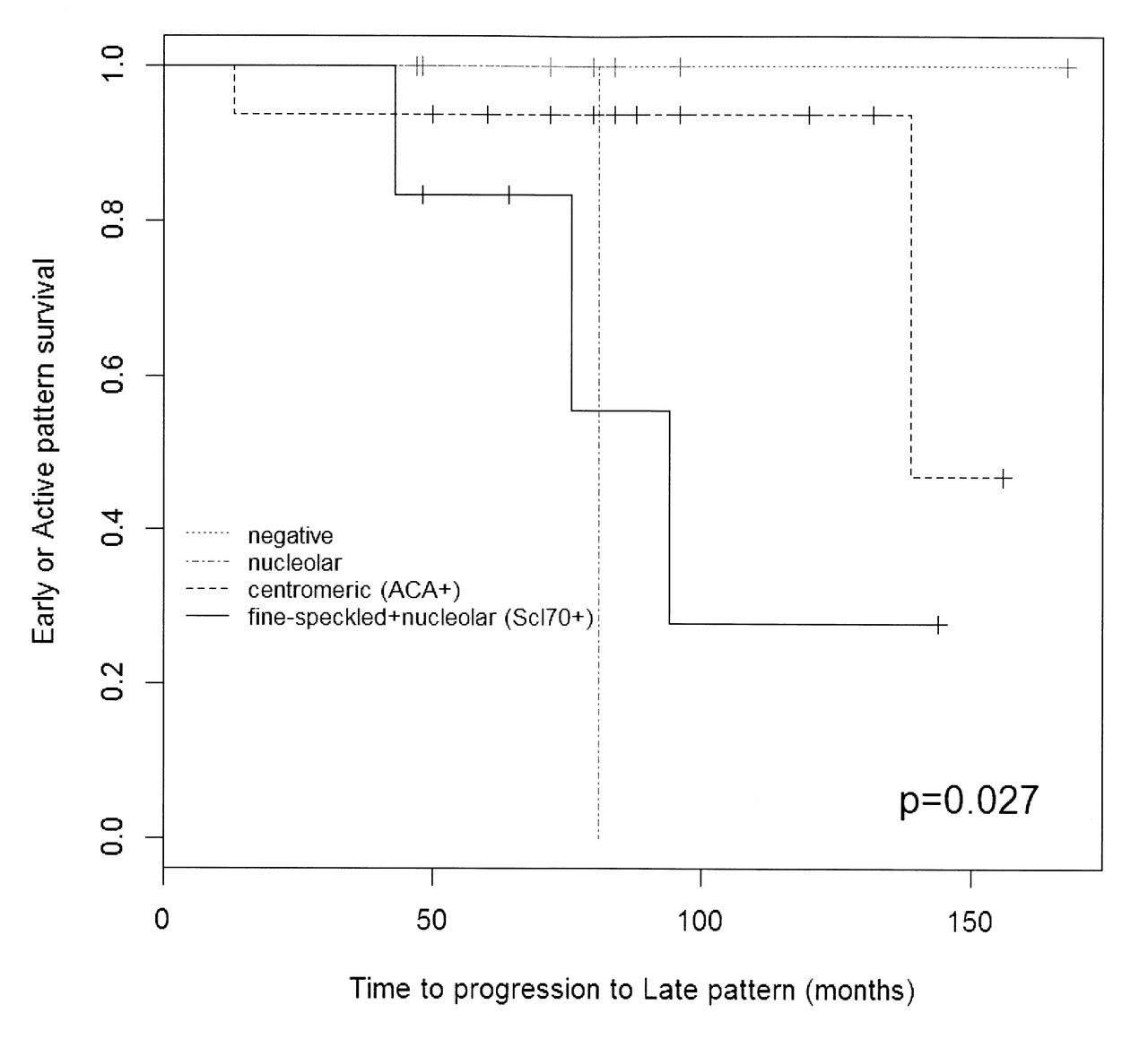
Kaplan-Meier plot shows survival probability of early/active stage of disease determined by nailfold videocapillaroscopy pattern, in relation to different antinuclear antibodies measured by indirect immunofluorescence. ACA: anticentromere antibodies; Scl-70: antitopoisomerase I antibodies.
In particular, Scl-70 autoantibodies (positive in 17% of all patients) were found significantly more frequently (57%) in patients with the late NVC pattern of microangiopathy (p = 0.025).
Observed frequencies for ANA IIF patterns and their distribution in SSc patients with different degrees of nailfold microvascular damage at the end of the followup period are reported in Tables 1 and 2.
Observed frequencies (%) for antinuclear antibodies (ANA) determined by indirect immunofluorescence in systemic sclerosis (SSc) patients with different patterns of nailfold microvascular damage (early, active, late) at the end of followup.
Distribution of antinuclear antibody (ANA) patterns determined by indirect immunofluorescence in scleroderma patients with different patterns of nailfold microvascular damage (early, active, late) at the end of followup. Data are percentages.
The microangiopathy evolution score was higher in patients with the nucleolar IIF pattern of ANA, compared with patients showing other IIF patterns, but the difference was statistically significant between only the nucleolar and the negative or speckled patterns (p = 0.05; Figure 3). No statistically significant difference was found at the end of followup between single capillaroscopy measurements and different autoantibody IIF profiles. Conversely, patients with SSc who showed a mild reduction of capillary number at the baseline visit were likely to have either the fine-speckled + nucleolar IIF pattern together with Scl-70 positivity or the nucleolar pattern.

Microangiopathy evolution scores (MES) in patients with systemic sclerosis who show different indirect immunofluorescence patterns for antinuclear antibodies (ANA). P = 0.05 nucleolar vs negative and nucleolar vs fine-speckled; p = 0.09 nucleolar vs centromeric; p = 0.10 nucleolar vs speckled + nucleolar Scl-70 (antitopoisomerase I antibodies).
In all patients with SSc, the ANA pattern on IIF did not change during the followup.
Interestingly, 37% of patients showing the early microangiopathy pattern at the end of followup were ANA-negative.
Within the limits of our small study population, among the patients with various ANA patterns on IIF, no imbalances or statistically significant differences were observed for patients’ ages at disease onset, duration of RP, or presence of limited or diffuse skin disease. Further, using multiple regression analysis, we investigated the evolution of the capillary patterns in patients with both subsets of skin involvement (limited or diffuse) and ANA patterns on IIF. No statistically significant correlation was found between evolution of capillary pattern and skin disease subset. Considering the ANA results, statistically significant correlations were observed only between those with the fine-speckled + nucleolar (Scl-70+) pattern and disease progression on NVC (p = 0.05), and between those with the nucleolar pattern and the microangiopathy evolution score (p = 0.03).
Clinical signs/symptoms progressed in accord with morphological nailfold changes in 62% of the patients with SSc, as previously reported1. In particular, SSc patients with the late microangiopathy pattern on NVC showed greater organ involvement than those with active and early patterns, determined by the prevalence of skin, lung, and esophageal involvement, pulmonary arterial hypertension, and digital ulcers.
DISCUSSION
Our study describes the dynamic and sequential progression of SSc nailfold microangiopathy through different NVC patterns linking them to different ANA patterns, and corroborates that it is an autoimmune-driven process1,6. The factors influencing the timing of progression of the microangiopathy have not been determined; however, patients with SSc may show the active or late scleroderma pattern even at the first visit, as a result of swift progression of the microangiopathy1.
In our study, different ANA IIF patterns were observed in patients whose microangiopathy progressed from the early through the active pattern to the late NVC pattern, or in patients still showing the early or active disease pattern at the end of the followup (Table 1). Centromeric (ACA) positivity was more prevalent in patients with SSc showing either the early or the active NVC pattern (not statistically significant), while the prevalence of Scl-70 autoantibody (associated with a fine-speckled + nucleolar IIF pattern) was significantly higher in patients with the late NVC pattern of microangiopathy. Both nucleolar and Scl-70 positivity were associated with faster progression of the SSc microangiopathy; thus patients showing rapid progression from the early to the active NVC pattern (i.e., < 1 year) should be monitored closely, because the evidence suggests they are at risk of rapid progression to the advanced NVC pattern of microangiopathy that is associated with more severe clinical manifestations of SSc.
In our prospective study, 45% of patients with SSc were still displaying the early NVC pattern of microangiopathy after a median followup of 7.5 years, while the pattern was changed in 55% of the patients. What hastened the progression of the SSc microangiopathy from early to active or late stage disease is not known, but few autoantibodies have been associated with the evolution of SSc, which is a well-recognized autoimmune disease5,7,8,9,10,15.
ACA have been described in association with a slower disease progression, and Scl-70 antibodies with a faster and more severe disease7,9. Further, SSc-specific autoantibodies were found to be strong predictors of microvascular damage in patients with RP who were prone to develop SSc. In such patients, findings of ACA and anti-Th/To antibodies predicted enlarged capillaries, whereas ACA and anti-RNA polymerase III predicted capillary loss. Moreover, each SSc-specific autoantibody was found to be associated with a distinct rate of microvascular damage5.
Antiendothelial cell antibodies (AECA) may also have a role in the progression of endothelial damage; their presence and titer were believed to represent additional risk factors for more severe disease, because advanced nailfold capillary findings were more frequently present in patients with higher levels of AECA16.
A possible limitation of our study is that only Scl-70 and ACA were investigated during the followup period 2001–2010, whereas other SSc-specific autoantibodies were not (i.e., antifibrillarin, anti-RNA polymerase, anti-Th/To, and AECA)15. Because these SSc-specific autoantibodies are not routinely assessed by many laboratories and are often associated with a specific ANA pattern on IIF, we focused on ANA patterns using IIF expression, which conversely may be easily detected by most laboratories. As well, possible associations between ANA titer and nailfold microvascular damage were not evaluated: the retrospective dataset did not permit this sort of evaluation, as most titers were reported as “> 1:320.” Thus, the results from our small sample should be examined by larger prospective studies of the role of specific autoantibodies in inducing nailfold microvascular damage.
From our IIF studies, the ANA fine-speckled + nucleolar pattern (not associated with Scl-70 antibody positivity) was more prevalent in patients with the early or active pattern of microangiopathy, and it was associated with a lower grade of microvascular damage. By contrast, a greater extent of microangiopathy was associated with the nucleolar pattern on IIF results (Figure 1).
A further interesting result was that 37% of patients with SSc showing the early NVC pattern of microangiopathy at the end of the followup were ANA-negative. Among them, only 25% of patients showed progression of organ involvement during the followup, leading to a confirmed diagnosis of SSc. The other 75% of patients still displayed the LeRoy criteria for limited SSc11 at the end of followup, with no further clinical manifestations, compared with the baseline visit. This observation suggests that large prospective studies are needed to evaluate the specificity and sensitivity of these classification criteria in patients with RP (observed by a physician), nailfold microangiopathy, and negative ANA results.
Our results confirm that there is a progressive transition of SSc microvascular damage through different NVC patterns of microangiopathy, and that ANA-negative patients with SSc (characterized by the early NVC pattern) display a slower progression of the nailfold microangiopathy. Faster progression to the late-stage NVC pattern (the more advanced stage of microvascular damage) seems to be associated with a different autoantibody pattern (anti-Scl-70/fine-speckled + nucleolar detected by IIF being the most prevalent), and this requires further investigation through larger longitudinal studies.
- Accepted for publication January 4, 2013.








{kind=link}
{kind=link}
{kind=link}