

Abstract
Objective. Biologic therapies can improve disease control for patients with rheumatoid arthritis (RA) but may be both overused and underused. We aimed to identify predictors of greater use of biologic therapies and to identify factors associated with persistent glucocorticoid use.
Methods. Using national US Veteran’s Affairs databases 2005–2016, we identified patients with RA receiving a first-ever prescription of methotrexate (MTX), requiring ≥ 6 months of baseline data. We evaluated predictors of biologic therapy initiation within 2 years of starting MTX and factors associated with baseline and persistent glucocorticoid use at 6–12 months using multivariable models.
Results. Among 17,415 patients starting MTX, 3263 patients received biologic therapy within 2 years (20.6% 2-yr incidence). In adjusted analyses, biologic use was substantially lower in older patients [e.g., aHR 0.20 (95% CI 0.16, 0.26) for patients ≥ 80 vs < 50] and patients with more comorbidities [aHR 0.79 (95% CI 0.72, 0.87) for Charlson score ≥ 3 vs < 3]. Patients with heart failure [aHR 0.68 (95% CI 0.54, 0.84)], cancer [aHR 0.78 (95% CI 0.66, 0.92)], or who were nonwhite [aHR 0.79 (95% CI 0.72, 0.87)] were also less likely to receive a biologic. In contrast, baseline and persistent glucocorticoid use was similar across age groups and more common in patients with greater comorbidity.
Conclusion. Biologic therapy is initiated less frequently in patients with RA who are older, have more comorbidities, and who are nonwhite. While biologics may be avoided in older and sicker patients because of safety concerns, glucocorticoid use is similar regardless of age and is more frequent in patients with comorbidities, with implications for patient outcomes.
Biologic disease-modifying antirheumatic drugs (bDMARD) have become an integral part of the treatment of rheumatoid arthritis (RA) over the past 2 decades. Clinical treatment guidelines provide options for the use of bDMARD in early disease, with either bDMARD or addition of conventional DMARD (cDMARD) recommended in patients with inadequate response to methotrexate (MTX)1,2. Prescribing of bDMARD may be influenced by the severity of disease, demographics, comorbidities, patient preferences, and preferences of the prescribing physician3,4. Differing treatment patterns and access may result in overtreatment of some patients who could achieve disease control with cDMARD, but also potential undertreatment of patients who continue conventional treatments despite active disease, leading to inadequate disease control or increased chronic glucocorticoid use.
Previous studies have identified a number of determinants of early initiation of biologic use, with differences in study design and study settings potentially contributing to varied results5–12. Limitations to the observational study of early biologic initiation include challenges identifying large numbers of individuals early in the disease course and difficulty accounting for differences in patient access to biologics due to variations in health insurance coverage. Critical to the assessment of treatment patterns is a study design that identifies a homogeneous patient population early in the course of disease with similar access to biologics.
Further, existing studies of biologic use have not evaluated predictors of longterm glucocorticoid use, an important and common alternative treatment to bDMARD. Glucocorticoid use is of particular interest because of substantial side effects even at modest doses and the uncertain safety of longterm low-dose therapy13. Patient subgroups with low bDMARD use but high glucocorticoid use could potentially be at greater risk of adverse outcomes.
In this study, we aimed to better understand patient factors affecting use of biologics and glucocorticoids. With this objective in mind, we used detailed clinical and administrative data from the US Veterans Affairs (VA) health system to evaluate predictors of early biologic use and persistent glucocorticoid use in a large, well-defined cohort of patients with RA initiating MTX.
MATERIALS AND METHODS
Study setting
We performed a cohort study using historical real-world clinical data from 3 linked national VA databases: The Corporate Data Warehouse, the Decision Support System National Pharmacy Extract, and the Pharmacy Benefits Management database between 2005 and 2016 – a time during which bDMARD were widely available. Together, these databases provide information on demographics, body mass index (BMI), laboratory results, physician diagnoses, and detailed pharmacy dispensing records along with a number of other patient, provider, and system factors14. The study was approved by the University of Utah Institutional Review Board (IRB 00012917), with informed consent waived owing to the de-identified nature of the data.
Patient population
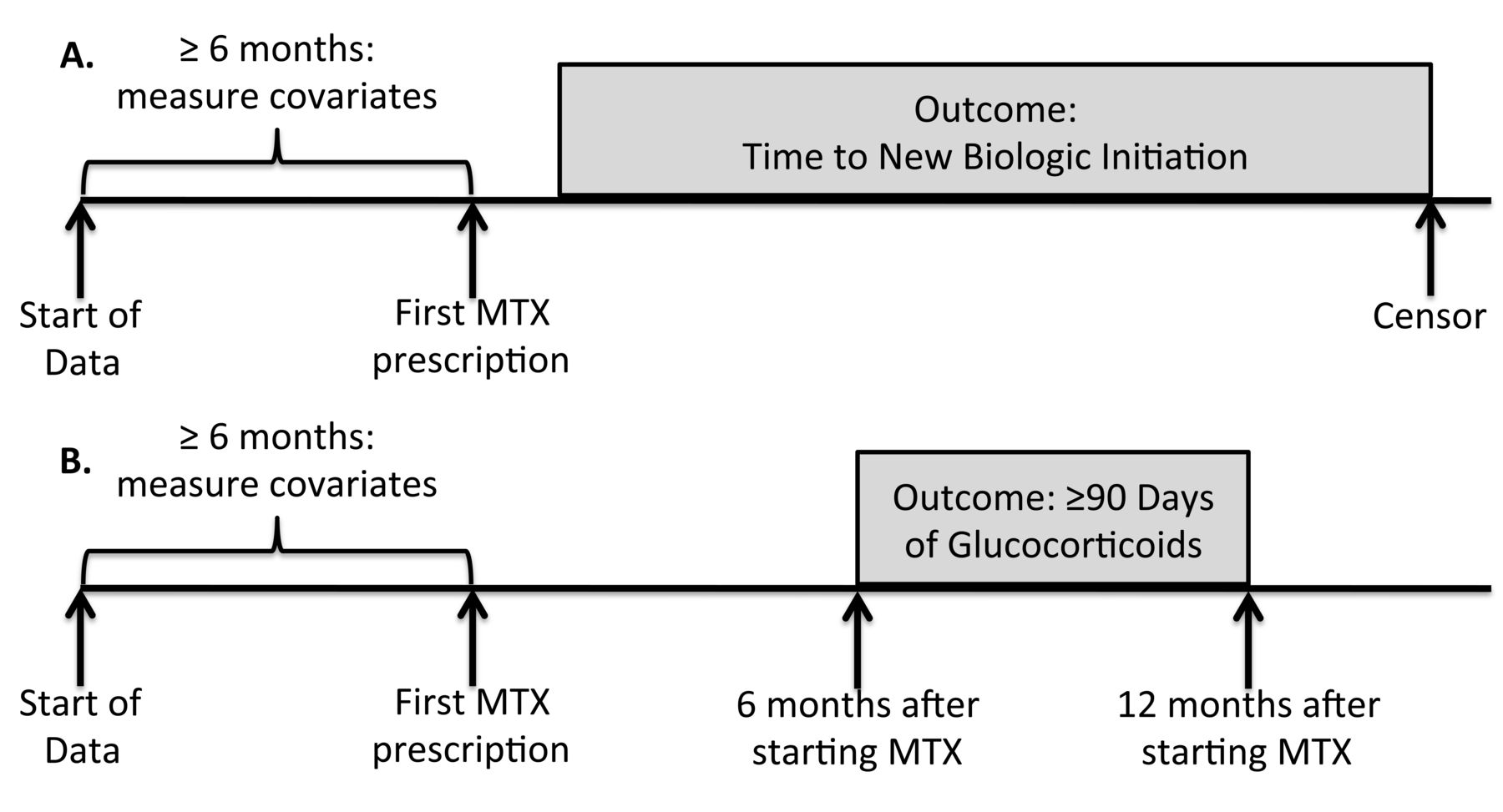
VA patients with RA were identified based on presence of a diagnosis code for RA and DMARD use15. We included patients receiving an initial prescription of MTX between 2005 and 2014, with data through 2016 used for followup. We required at least 6 months of prior baseline data within the VA prior to the first MTX prescription to identify an inception cohort of new users of MTX. The MTX start date was considered the index date (Figure 1). Patients with biologic therapy prescriptions or administration at any time prior to the index date, or those initiating biologic therapy within 30 days after the index date (considered simultaneous MTX and biologic initiation) were excluded. These criteria were designed to identify a homogeneous cohort of patients (all with disease severe enough for a physician to prescribe MTX) at a similar time in the course of their disease (at the time of first MTX initiation).

Study design. A. Evaluating time to biologic initiation within 2 years of starting methotrexate (MTX). B. Evaluating persistent glucocorticoid use in the 6–12 months after starting MTX, based on cumulative glucocorticoid prescriptions.
Medication courses
Medication-dispensing episodes were used to create medication courses for MTX, other DMARD, and glucocorticoids as previously described16,17. First, the expected supply for each prescription was determined based on dosing instructions and the number of pills dispensed. A medication course was defined as continuous treatment with a medication with no gaps > 90 days between the expected end of 1 prescription and the start of the next prescription. These medication courses were used to identify prior use of cDMARD before MTX [use of leflunomide (LEF), sulfasalazine (SSZ), or hydroxychloroquine (HCQ) prior to the first MTX prescription] and concomitant use of cDMARD (active medication course within 30 days of MTX initiation). Because glucocorticoid prescriptions may not match intended use and a single prescription at times may last several months, glucocorticoid use at baseline was defined as any active glucocorticoid course in the 90 days before or 30 days after the first MTX prescription.
Outcomes
The primary outcomes of interest were (1) time to biologic initiation; and (2) persistent glucocorticoid use. We evaluated time to biologic initiation by measuring the time from the initiation of MTX (the index date) to the first prescription or administration of a biologic therapy (including infliximab, adalimumab, etanercept, certolizumab, golimumab, abatacept, rituximab, or tocilizumab; Figure 1A). We defined persistent glucocorticoid use as ≥ 90 days of glucocorticoid exposure within the period 6–12 months after starting MTX, based on the sum of all glucocorticoid courses during this time window (Figure 1B). This time window was chosen to allow at least 6 months for disease control and glucocorticoid tapering after MTX initiation, identifying patients exposed to more longterm, persistent glucocorticoids. In a sensitivity analysis we also evaluated an alternative definition of persistent glucocorticoid use, defined as ≥ 30 days of cumulative glucocorticoid exposure in the 6–12 months after starting MTX.
Predictors of interest
This study evaluated a number of hypothesized predictors of early biologic initiation and persistent glucocorticoid use including age, sex, race (categorized as white, nonwhite, or unknown), current smoking, BMI (from measurements within 1 yr before the index date), comorbid conditions (based on International Classification of Diseases, 9th ed diagnosis codes in the year prior to the index date, based on established algorithms)18,19,20,21, overall comorbidity burden based on the Charlson score22, markers of RA severity [anticyclic citrullinated peptide antibodies (anti-CCP) positivity at any time and C-reactive protein levels within 6 mos before the index date], prior cDMARD use, and concomitant cDMARD use. Baseline glucocorticoid use was also evaluated as a potential predictor of biologic initiation. In analyses evaluating predictors of persistent glucocorticoid use, models were not adjusted for baseline glucocorticoid use because the majority of patients receiving persistent glucocorticoids received glucocorticoids at baseline (84%). We separately evaluated predictors of baseline glucocorticoid use.
Statistical analysis
Multivariable Cox proportional hazards models assessed factors associated with time to biologic therapy initiation, censoring at the earliest of death, end of study followup, or 2 years after starting MTX. Multivariable logistic regression was used to assess factors associated with persistent glucocorticoid use in the period 6–12 months after starting MTX, excluding patients who did not have at least 12 months of followup. A similar analysis was used to identify factors associated with glucocorticoid use at baseline among all patients initiating MTX. All models were reduced using stepwise backward selection of covariates with p > 0.2, forcing age, sex, and race into all models. Proportional hazards were assessed using log-log plots. Multiple imputation with 10 imputations was used to account for missing values of anti-CCP positivity, BMI, and C-reactive protein (CRP; Table 1 describes frequency of missingness). Sensitivity analysis requiring a 1-year baseline period before MTX initiation did not change results (not shown). All analyses were conducted with STATA 14.0 software (StataCorp. LP) within the VA Informatics and Computing Infrastructure.
Baseline cohort characteristics.
RESULTS
We identified 39,789 patients with a diagnosis of RA and a first prescription for MTX. Of these patients, 17,415 met all inclusion criteria, contributing 26,327 years of followup (up to 2 years for each patient). Forty-five percent of patients were ≥ 65 years old, 88% were male, and 73% were white (Table 1). Smoking, depression, anxiety, posttraumatic stress disorder, and asthma/chronic obstructive pulmonary disease (COPD) were common in the cohort. Almost half of the cohort received glucocorticoids, 22% of patients were treated with a combination of MTX and HCQ, and few received concurrent SSZ or LEF at baseline. Only 361 (2.1%) of patients were receiving triple therapy with MTX, HCQ, and SSZ at the time of MTX initiation.
Predictors of biologic therapy initiation
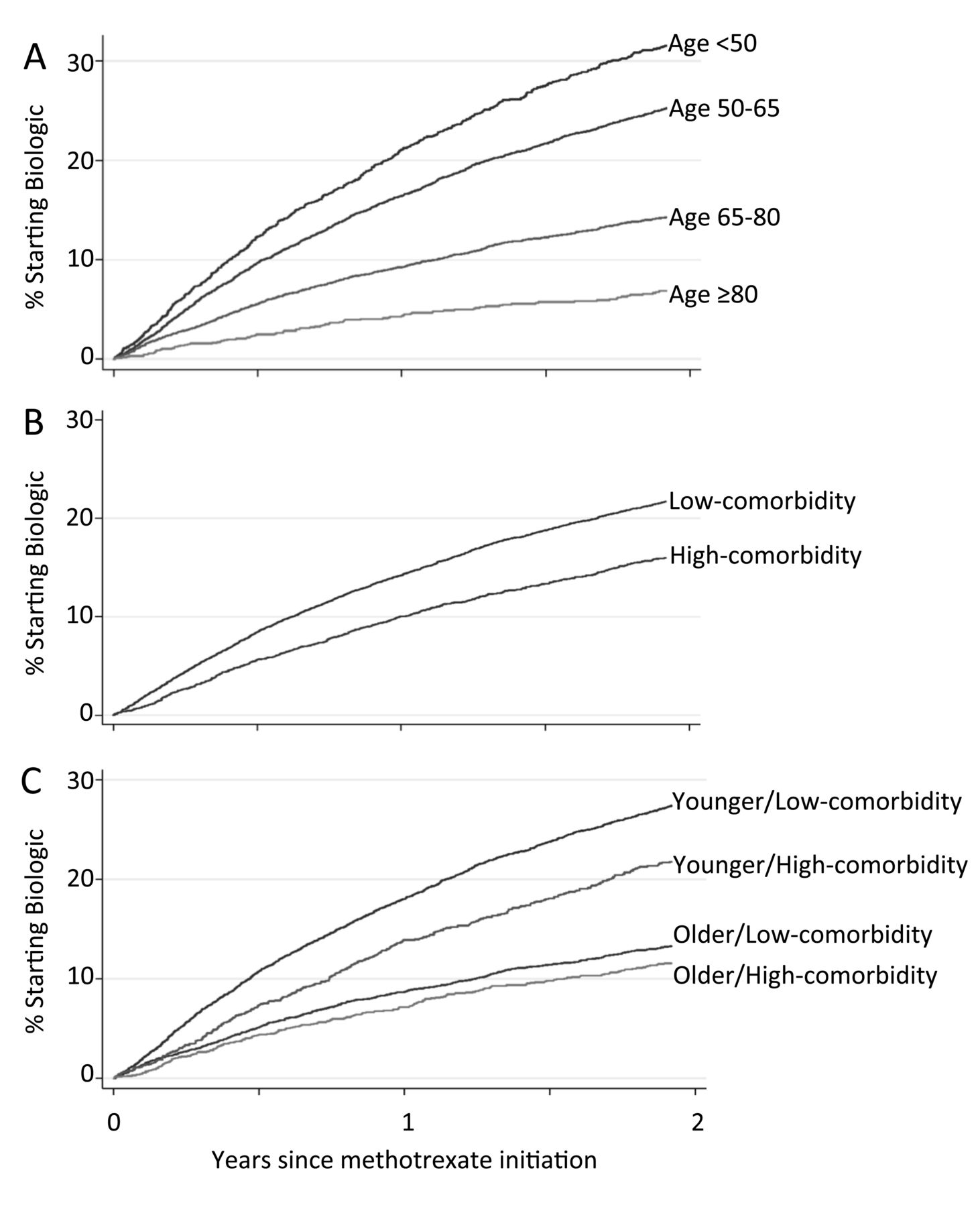
A total of 3263 patients initiated biologic therapy during up to 2 years of followup — a cumulative incidence of 12.6% at 1 year and 20.6% at 2 years. The most commonly prescribed first bDMARD class after MTX was tumor necrosis factor inhibitors (95.3% of biologic initiations). Rates of biologic initiation were substantially lower in older patients and those with high comorbidity burden (Charlson score ≥ 3, 20.1% of the cohort). Comorbidities were associated with less biologic use in older and younger patients (p for interaction 0.22), although rates of biologic use remained low in elderly patients without substantial comorbidity (Figure 2). In adjusted analyses, patients 80 years of age or older were 80% less likely to start a biologic compared to those < 50 (adjusted HR 0.20, 95% CI 0.16–0.26; Table 2). Additionally, patients were less likely to receive a biologic if they were nonwhite (aHR 0.79, 95% CI 0.72–0.87), had congestive heart failure (aHR 0.68, 95% CI 0.54–0.84) or cancer (aHR 0.78, 95% CI 0.66–0.92), or had received a cDMARD prior to MTX (aHR 0.82, 95% CI 0.76–0.88). Greater comorbidity (higher Charlson score) was associated with less biologic use even when several individual comorbidities were included in the model (aHR 0.95, 95% CI 0.92–0.98 per each additional point; Table 2). In a similar multivariable model without individual comorbidities included, a Charlson score ≥ 3 (20.1% of the cohort) was associated with a 20% lower rate of biologic use (HR 0.79, 95% CI 0.72–0.87, p < 0.001; full model not shown). In contrast, higher rates of biologic initiation were associated with higher BMI, anti-CCP positivity, smoking, and concomitant glucocorticoid, LEF, or SSZ use (Table 2). The likelihood of initiating a biologic was greater from 2011 to 2014 compared to 2005 to 2010 (aHR 1.20, 95% CI 1.11–1.29).

Effect of age and comorbidity on time to biologic initiation in patients with rheumatoid arthritis starting methotrexate. Kaplan-Meier curves showing cumulative incidence of biologic initiation based on (A) age; (B) comorbidity (low comorbidity = Charlson < 3, high comorbidity = Charlson ≥ 3); and (C) combination of age and comorbidity (younger = age < 65 yrs, older = age ≥ 65 yrs).
Factors associated with time to biologic therapy initiation in patients with RA starting methotrexate, using multivariable Cox regression.
Baseline and persistent glucocorticoid use
Glucocorticoids were used at baseline by 8465/17,415 patients (49%). Frequency of use was similar across age groups and was greater in patients with a higher Charlson comorbidity score, depression, asthma/COPD, interstitial lung disease, higher CRP, and patients who were concomitantly treated with HCQ (Table 3). Women, patients with higher BMI, and patients with diabetes were less likely to receive glucocorticoids at baseline (Table 3). Among 15,610 patients with at least 12 months of followup, 1440 (9.2%) received at least 90 days of glucocorticoids cumulatively in the 6–12 months after starting MTX (persistent glucocorticoids). Patients who were ≥ 80 received persistent glucocorticoids at similar rates as younger patients < 50 years old (aOR 1.07, 95% CI 0.83–1.39; Table 4). Greater comorbidity score was not associated with persistent glucocorticoid use (excluded from model, p > 0.2). Higher baseline CRP, HCQ use, and LEF use were associated with more persistent glucocorticoid use, while women and patients who smoked were less likely to receive persistent glucocorticoids. In separate adjusted analyses, we found that patients who initiated biologic therapy in the first 6 months were more likely to receive persistent glucocorticoids (aOR 1.25, 95% CI 1.02–1.53), although this association was not found among patients treated with glucocorticoids at baseline (aOR 1.02, 95% CI 0.81–1.28; full models not shown).
Factors associated with baseline glucocorticoid use, using multivariable logistic regression.
Factors associated with longterm glucocorticoid use: ≥ 90 days or ≥ 30 days of glucocorticoids 6–12 months after starting methotrexate, using multivariable logistic regression.
In sensitivity analysis using the alternative definition of persistent glucocorticoid use (≥ 30 cumulative days of glucocorticoid use 6–12 months after starting MTX; N = 3300, 21.1%), rates of persistent glucocorticoid use were again similar by age, but higher Charlson comorbidity score was associated with a greater likelihood of persistent glucocorticoid use (aOR 1.05, 95% CI 1.02–1.08 per point increase; Table 4). CRP, HCQ use, and LEF use were again associated with greater likelihood of persistent glucocorticoid use, as were anti-CCP positivity, depression, and interstitial lung disease. Again, female sex was associated with a lower likelihood of persistent glucocorticoid use, as were greater BMI, diabetes, and previous use of a cDMARD (Table 4).
DISCUSSION
Our study provides important insight into patterns of biologic use by studying a large, homogeneous cohort of patients with RA initiating MTX with similar access to bDMARD through the VA health system. In this population, rates of biologic initiation were dramatically lower in patients who were older, nonwhite, and who had a greater comorbidity burden. An important addition of our work to prior reports is the evaluation of predictors of baseline and persistent glucocorticoid use, which carry substantial toxicity risks and may suggest suboptimal disease control. We found that baseline and persistent glucocorticoid use were similar in older vs younger patients, and surprisingly, that patients with comorbidities were more likely to receive glucocorticoids at baseline and perhaps more likely to receive longterm glucocorticoids.
The patterns of treatment in older patients in our study are of particular interest, with significantly less biologic use but similar glucocorticoid use compared to younger patients. Less biologic use in elderly patients has been previously reported6,7,8,9,10,11 and may reflect safety concerns with biologics in this population. Yet if safety concerns exist, they have not led to lower rates of glucocorticoid use in this population. In fact, avoidance of biologic DMARD could potentially increase glucocorticoid requirements and possibly result in a worse safety profile in this high-risk population. Studies have suggested greater infection risk from moderate doses of glucocorticoids versus biologics, in addition to effects on bone health, cardiovascular risk, and other outcomes that disproportionately affect older adults13,23,24, yet the comparative risk of biologics and glucocorticoids (especially low-dose glucocorticoids) remains poorly understood, and especially considering the substantial cost differences of these therapies, is an important area of future research25. Our findings cannot exclude the possibility that RA was less severe or more easily controlled in older patients, but we restricted our study to MTX-treated patients (excluding patients whose disease was controlled only with low-dose glucocorticoids or HCQ, for example) and we found that glucocorticoid use was similar at baseline and in followup.
Comorbidities were also major predictors of biologic initiation. Previous studies have shown mixed results regarding associations between comorbidities and biologic use5,6,7,8,10,11,12. We found that patients with greater comorbidity, and in particular those with congestive heart failure or malignancy, were much less likely to receive biologic therapy. As with increasing age, this association likely reflects safety concerns for use of biologics in patients with these comorbidities. Interestingly, patients with greater comorbidity burden were more likely to receive glucocorticoids at baseline and had similar or greater rates of persistent glucocorticoid use compared to healthier patients. Determining whether avoidance of biologics in patients with comorbidities improves safety or conversely results in suboptimal disease control or greater complications from glucocorticoid exposure is an important area for future research.
Of additional concern is the racial disparity in biologic use observed in this study, similar to what has been reported in previous studies of other cohorts8,9. The VA system provides similar access to biologics to patients who meet a certain income threshold and to veterans whose condition is service-connected, independent of private insurance coverage, and so our findings are less likely to reflect differences in access to the therapies themselves. Interestingly, while we found differences in biologic use in white versus nonwhite patients in national VA data, these differences were not observed in a smaller study of veterans followed prospectively in the VA Rheumatoid Arthritis (VARA) registry, potentially related to differences in study design or to differences in patient and physician preferences in this prospective registry26. The complex contributors to racial disparity and its effect on disease control are important areas of investigation.
Differences in RA disease severity likely explain a number of other associations that were observed. Anti-CCP status, baseline glucocorticoid use, concomitant LEF or SSZ use predict greater biologic use because they are surrogates for more severe RA. Conversely, prior cDMARD use before MTX is likely associated with less biologic use because these patients have less severe disease. Similarly, while we did not find a steroid-sparing effect of biologic initiation (those initiating biologics in the first 6 months were not less likely to receive persistent glucocorticoids), we were not able to accurately assess for dose reductions and potential steroid-sparing effects because patients with early initiation of biologics have more severe disease, leading to increased glucocorticoid requirements. Women and patients with diabetes or obesity were less likely to receive glucocorticoids, perhaps reflecting greater risk of side effects in these populations.
Limitations of our study include the inability to fully adjust for disease activity, although we restricted the study to MTX initiators to create a more homogeneous population and included baseline CRP levels, previous DMARD treatment, and glucocorticoid use. Given the lack of comprehensive clinical disease activity measures, we could not assess the effect of variability in biologic prescribing on subsequent disease control or differing disease activity thresholds for biologic initiation. We did, however, evaluate the need for continued glucocorticoids and identified significant associations with persistent glucocorticoid use. Although we could not accurately assess glucocorticoid dose or dose changes, we were still able to identify important associations with glucocorticoid use. Dual care (receiving treatment outside of the VA system) is a potential issue in VA research, although previous work has suggested that the great majority of RA medications are filled through the VA system27. Additionally, a minority of patients may have had previous MTX or biologic prescriptions before entering the VA system; we limited this bias by requiring a 6-month baseline period before the first MTX prescription, and results were similar if a 12-month baseline period was required. Comorbidity data were based on diagnosis codes and we were unable to assess severity of comorbidities, but even with this limitation we found substantial associations between comorbidities and biologic use. The reasons for biologic use or avoidance cannot be directly determined and we were unable to assess the role of patient and provider preference. Finally, the VA population is largely male, with higher rates of smoking, lung disease, and mental health disorders than the general US population, although we found similar results in men and women, and patterns of biologic use were similar to reports from other US cohorts.
Advantages of our study are the large cohort of patients within a single healthcare system, the well-defined study design that mimics real-world decision making in patients starting MTX, and the additional evaluation of baseline and persistent glucocorticoid use. VA databases provide extensive and accurate prescription data as well as demographic, comorbidity, and laboratory data. Additionally, use of the VA system reduces potential bias related to patient access to medications due to cost or lack of health insurance.
In the VA health system, biologic therapy is initiated much less frequently in patients with RA who are older, have greater comorbidity, and who are nonwhite. Concern about the safety of biologics in older patients and patients with comorbidities is likely to be an important driver of the lower rates of biologic use in these patients. Glucocorticoid use, however, is similar regardless of age and is more frequent in patients with comorbidities. Determining the consequences of these treatment patterns on disease outcomes and the relative risks and benefits of biologics and glucocorticoids in these subgroups is needed to optimize treatment of these patients.
Footnotes
Dr. George is supported by the Rheumatology Research Foundation Scientist Development Award. Dr. Cannon is supported by Specialty Care Center of Innovation, Veterans Health Administration, Department of Veterans Affairs. Dr. England is supported by the UNMC Physician-Scientist Training Program and UNMC Internal Medicine Scientist Development Award. Dr. Mikuls is supported through funding from a VA Merit Award (CX000896) and from the US National Institutes of Health (National Institute of General Medical Sciences grant U54-GM-115458). Dr. Baker is supported by a VA Clinical Science Research and Development Career Development Award (IK2 CX000955). Drs. Sauer and Cannon receive grant funding from Amgen for unrelated work. The contents of this work do not represent the views of the US Department of Veterans Affairs or the US government.
- Accepted for publication July 18, 2018.








{kind=link}
{kind=link}