

Abstract
Objective. Patients with an HLA-B*58:01 allele have an increased risk of developing severe cutaneous adverse drug reactions (SCAR) when treated with allopurinol. Although one-off pharmacogenetic testing may prevent life-threatening adverse drug reactions, testing prior to allopurinol initiation incurs additional costs. The study objective was to evaluate the cost-effectiveness of HLA-B*58:01 screening compared with using other available urate-lowering agents (ULA).
Methods. A decision-analytical model was used to compare direct medical costs and effectiveness [including lifetime saved, quality-adjusted life-yrs (QALY) gained] in treating new patients with the following options: (1) genetic screening followed by allopurinol prescribing for noncarriers of HLA-B*58:01, (2) prescribing benzbromarone without screening, (3) prescribing febuxostat without screening, and (4) prescribing allopurinol without screening. A 1-year time frame and third-party payer perspective were modeled for both the entire cohort (base-case) and for the subgroup of patients with chronic kidney disease (CKD).
Results. The incremental cost-effectiveness ratio of genetic screening prior to ULA therapy was estimated as New Taiwan (NT) $234,610 (US$7508) per QALY gained in the base-case cohort. For patients with CKD, it was estimated as NT$230,925 (US$7390) per QALY. The study results were sensitive to the probability of benzbromarone/febuxostat-related hypersensitivity, and a negative predicted value of genotyping.
Conclusion. HLA-B*58:01 screening gave good value for money in preventing allopurinol-induced SCAR in patients indicated for ULA therapy. In addition to the costs of genotyping, it is important to monitor ULA safety closely in adopting HLA-B*58:01 screening in practice.
Drug hypersensitivity carries an immense burden of morbidity and mortality1,2,3. According to the Taiwan National Drug Relief and Voluntary Adverse Drug Reporting System, allopurinol is the drug with the most potential to induce severe cutaneous adverse reactions (SCAR), including Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug reaction with eosinophilia and systemic symptoms4,5. A strong association between possession of the HLA-B*58:01 allele and risk of allopurinol-induced SCAR has been observed among Han Chinese (i.e., ethnic Chinese from Taiwan and Hong Kong), Thais, Indians, and Koreans6,7. The prevalence of the HLA-B*58:01 allele ranges from 1.9% to 27.5% in the general Asian population, but is very rare in whites8. Chronic kidney disease (CKD) is also suggested to be a nongenetic factor associated with allopurinol hypersensitivity symptoms9,10. A plausible mechanism for this is that the oxypurinol metabolite accumulates in patients with impaired renal function11 so that the risk of allopurinol hypersensitivity is increased by 4–5× in patients with CKD treated with allopurinol (OR 4.7, 95% CI 2.3–9.3)11.
The 2012 American College of Rheumatology (ACR) gout guidelines recommends xanthine oxidase inhibitor (XOI) therapy with either allopurinol or febuxostat, and probenecid as the first-line alternative where XOI is contraindicated12. Other urate-lowering agents (ULA) such as benzbromarone are also in common use in Taiwan13. Benzbromarone is used particularly in patients with renal function disorders. Its recommended dose is usually 50–200 mg daily, which is generally well tolerated, although regular liver function monitoring is essential14. Specific genotyping for HLA-B*58:01 is currently available in Taiwan. Although the Taiwan Food and Drug Administration has suggested genotyping patients before prescribing allopurinol since 200915, this genotyping is not reimbursed by the National Health Insurance (NHI) program. Although the cost of genotyping is high, the high cost of alternative ULA and the chance that many patients will not develop SCAR mean that the value of routine genotyping prior to prescribing allopurinol is unclear.
We therefore evaluated the cost-effectiveness of HLA-B*58:01 screening compared with using available alternative ULA (benzbromarone, febuxostat, and allopurinol) without prior genotyping. We also examined the incidence of allopurinol-related SCAR and the associated costs of health services use.
MATERIALS AND METHODS
Identification of patients with allopurinol-related SCAR
A retrospective, population-based cohort study was conducted to identify incidence, mortality, and total medical costs attributed to allopurinol-related SCAR, using the 2 million random beneficiaries from longitudinal database in the Collaboration Center of Health Information Application (CCHIA), which were available from 2000 to 2011. The CCHIA database holds complete information about almost all claims from the Taiwan NHI program, and its details have been well described elsewhere16. The study proposal was reviewed and approved by the institutional review board and ethics committee of Chang Gung Medical Foundation in Taiwan (103–4218B).
Analysis of incidence of SCAR
The initial adverse drug reaction–related SCAR visits were defined by the following criteria: (1) International Classification of Diseases, 9th ed codes (Supplementary Table 1, available with the online version of this article) for SCAR from outpatient or emergency visit or hospitalization discharge17,18, (2) allopurinol discontinuation following the diagnosis of SCAR, and (3) SCAR events occurring within 100 days of discontinuation18. Because HLA-B*58:01 is not only a risk factor for severe cutaneous reactions, but also for mild cutaneous adverse reactions, such as maculopapular exanthema in the Han Chinese population19, broad criteria of any allopurinol-related skin reactions were used to minimize underestimation of incidence. The total number of incident cases over the study period was consistent with the documented reports in the national reporting center of adverse drug reactions in Taiwan between 1999 and 20104.
The incidence of adverse drug reactions was calculated for each calendar year from 2001 to 2011. Incidence was expressed as the number of SCAR divided by the total number of new allopurinol users in each calendar year. Within the cohort of allopurinol-related SCAR, the incidence of death and discharge were calculated using the number of adverse drug reactions in the corresponding calendar year as the denominator. The subgroup analysis was conducted for those new allopurinol users with CKD, assessing the incidence of SCAR in the same way.
All costs for outpatient care, emergency visits, and inpatient medical care are paid by a single third-party payer NHI program in Taiwan. The economic perspective for our study, therefore, included all related healthcare costs. The burden of adverse drug reaction–related visits to the healthcare system was estimated among patients receiving healthcare services for allopurinol-associated adverse reactions. The total cost included all corresponding outpatient and emergency visits and any hospital admissions. The total medical costs were updated to the last observed period of data and expressed in 2015 Taiwan dollars. The database was censored at the study end date, so costs could not be estimated for patients with SCAR after September 30, 2011. Mean annual costs of allopurinol-related SCAR, direct medical cost per SCAR event, and overall medical costs between 2001 and 2011 were assessed.
Cost-effectiveness analysis (CEA)
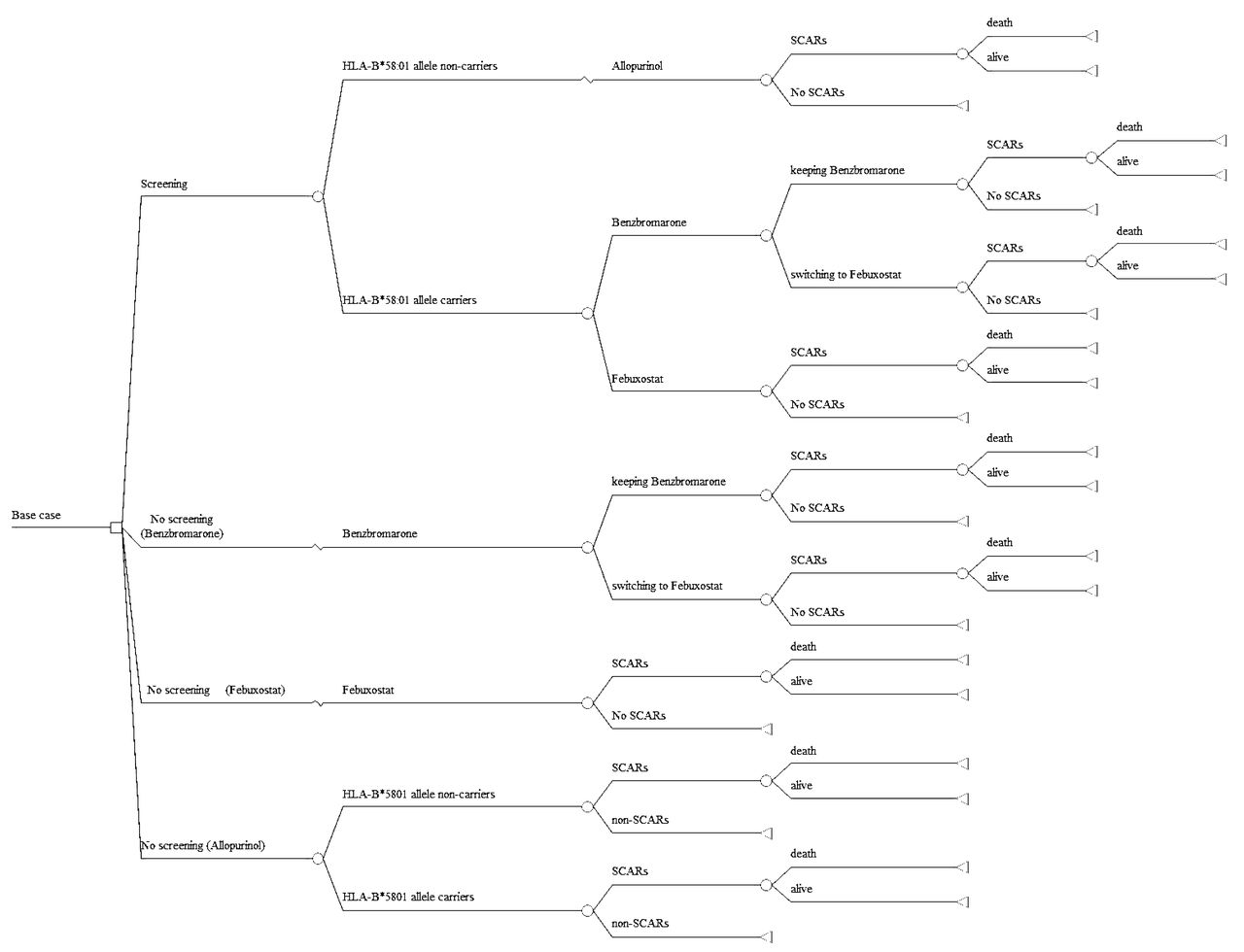
A decision tree model was developed to estimate the cost-effectiveness of HLA-B*58:01 genotyping for adult patients with newly diagnosed hyperuricemia or gout in Taiwan for whom allopurinol, benzbromarone, or febuxostat were considered suitable as first-line monotherapy (Figure 1).

Decision tree model for treatment strategy in allopurinol new users. There were 4 treatment strategies in the model: (1) genetic screening prior to allopurinol prescribing, (2) prescribing benzbromarone without screening, (3) prescribing febuxostat without screening, and (4) prescribing allopurinol without screening. Three possible outcomes were modeled: (1) being cured of allopurinol-induced SCAR, (2) death attributed to allopurinol-induced SCAR, and (3) not developing allopurinol-induced SCAR. SCAR: severe cutaneous adverse drug reactions.
Model variables
Prior cost-effectiveness analyses of HLA-B*58:01 genetic test did not include comparisons with febuxostat and benzbromarone as alternative treatment strategy20,21. In accordance with updated treatment guidelines for hyperuricemia and the pattern of ULA use in the real-world setting, the treatment strategies evaluated in our present study included (1) genetic screening prior to allopurinol prescribing, (2) prescribing benzbromarone without screening, (3) prescribing febuxostat without screening, and (4) prescribing allopurinol without screening. Table 1 presents variables used in the model8,9,11,22,23,24,25,26,27.
The variables in the cost-effectiveness analysis model.
Because the 2012 ACR gout guidelines recommended that allopurinol and febuxostat be considered as equivalent first-line options, the efficacy variation of ULA because of individual patients’ serum uric acid level and escalating doses were not considered in our study12. Overall, febuxostat was generally well tolerated and equally safe with allopurinol in large clinical trials, also in patients with renal dysfunction28,29.
Benzbromarone is considered at least equally effective as allopurinol at achieving target serum uric acid14, particularly for patients in whom allopurinol has insufficient response or toxicity, which is consistent with the recommendations of European League Against Rheumatism in 201630. Benzbromarone was withdrawn from the French market in 2003 by the manufacturer following the spontaneous reports of serious liver toxicities; it is still available in some European countries and several Asian countries, including Taiwan. The incidence of benzbromarone-induced hepatotoxicity has been estimated to be 1:17,000 persons based on 4 published case reports and 11 cases of postmarket safety reports between 1994 and 200231. The benefit-risk assessment of benzbromarone in the treatment of gout does not support the decision for the market withdrawal31. The current labeling of benzbromarone in Taiwan lists liver cirrhosis as contraindication and its risk of hepatotoxicity is lower than the general incidence of antituberculosis (5.9/1000 person-mos)32 and antifungal (1.58–8.39 per 10,000)33 drug-induced hepatoxicity. Benzbromarone was modeled in our study, and even though use of benzbromarone has changed over time13, it remains a common choice of ULA in a clinical setting.
Patients who have a negative HLA-B*58:01 testing result could receive and remain with allopurinol therapy. Patients with a benzbromarone strategy could switch to febuxostat (13.75%) if they experienced intolerance or failed to respond, or could remain with benzbromarone within 1 year of initial therapy based on our own investigation in the study setting. Further, patients who began with febuxostat could remain in the therapy for over 1 year. The clinical course of action for patients receiving ULA therapy was modeled in our study to reflect actual decision making in a clinical practice setting. A combination ULA therapy strategy (e.g., allopurinol or febuxostat combined with benzbromarone) was not considered during the initial phase of treatment.
Probenecid and sulfinpyrazone are uricosuric agents that were recommended as second-line use in those resistant to or intolerant of allopurinol30,34,35, but both drugs were not commonly used (< 50/100,000 persons) and not considered in the model13.
Incidence of SCAR
The probability of allopurinol-induced SCAR in patients with/without HLA-B*58:01 was calculated using conditional probabilities, in line with a previous study (Supplementary Data 1, available with the online version of this article)21,22. Although benzbromarone- and febuxostat-related severe skin adverse reactions have been reported, their actual incidence was not clear23,24. We therefore assumed the probability of an adverse drug reaction was 0.0001 (1 per 10,000 persons) or “very rare”36.
Outcomes
Three possible outcomes were defined and modeled. These were (1) being cured of allopurinol-induced SCAR, (2) death attributed to allopurinol-induced SCAR, and (3) not developing allopurinol-induced SCAR. The utility for patients with gout has been measured as 0.9435 for chronic patients in the Japanese population25. The utility for patients who developed SCAR was measured as 0.47 in the Thai population26. For patients with CKD, utility was recommended as 0.839 (0.794–0.884) in the Japanese population27.
The results were presented as the total expected costs, lifetime saved, and quality-adjusted life-years (QALY) gained. The incremental cost-effectiveness ratio was expressed as incremental cost per life-years or QALY gained.
Time frame
Because allopurinol-induced SCAR mostly occur within 1 year of the initiation of treatment, and 90% of cases occur within 180 days18, a 1-year study time frame was set. Costs of ULA therapy were followed for 1 year. The 1-year prescription cost of ULA use was measured based on the medication cost as unit cost of drug multiplied by annual quantity37.
The model further assumed that the cost of the HLA-B*58:01 screening test was NT$2648 (US$87.7, US$1 = NT$31.25 in 2015), the price given in the Taiwan National Health Insurance program.
Sensitivity analysis
Our model included data from various sources, so it was important to validate the data. We performed univariate deterministic analyses with a Tornado diagram for the variables in the model: the incidence of SCAR related to ULA alternatives, the association between the HLA-B*58:01 allele and allopurinol-related SCAR, positive predictive value and negative predictive value (NPV) of the HLA-B*58:01 genetic test (Supplementary Data 1, available with the online version of this article), and the prevalence of the HLA-B* 58:01 allele in the Taiwanese population. Also analyzed were the probability of death from allopurinol-related SCAR, the utility for patients with gout and with SCAR, the cost of HLA-B 58:01 screening, the annual cost of ULA (allopurinol, febuxostat, or benzbromarone) and hyperuricemia/gout management, the probability and duration of ULA switching, and the total medical costs of treating patients with and dying from SCAR. The range of each variable was retrieved from the 95% CI, if available. If not available, the range was defined as 0.5–1.5× the base value.
A probabilistic sensitivity analysis (PSA) was performed to obtain cost-effectiveness acceptability curves at different maximum willingness to pay (WTP) thresholds. The PSA examined the effect of uncertainty in all variables simultaneously using a second-order Monte Carlo simulation across 10,000 iterations, with the value of each variable being determined by a random draw from an assigned distribution.
The same analysis was conducted for the entire sample of patients and for the subgroup of patients with CKD. All assumptions were presented to and validated by clinical and health economic experts. A decision tree model was developed in TreeAge Pro 2014 software (TreeAge Inc.) to estimate the cost-effectiveness of HLA-B*5801 genotyping prior to ULA therapy.
Statistical analysis
Variables were expressed as means and SD or median and interquartile range (IQR) for continuous variables, and numbers and percentages for categorical variables. Statistical tests of significance for differences used the Pearson chi-square test for dichotomous variables and the Student t test for continuous variables. The level of significance was set at p < 0.05. All data processing and analyses were conducted using SAS 9.3 (SAS Inc.).
RESULTS
Health outcomes of allopurinol-related SCAR
Supplementary Table 2 (available with the online version of this article) shows the incidence of allopurinol-related SCAR and lifetime saved. A total of 147 allopurinol-related SCAR were observed among 66,276 new allopurinol users between January 2001 and December 2011. The mean time of followup was 28.08 months, and the overall incidence of allopurinol-related SCAR was 0.22% (95% CI 0.19–0.26%) or 2.2 SCAR cases per 1000 allopurinol new users. Of allopurinol-related SCAR (n = 147), 15 patients (10.2%) died during hospitalization for SCAR (95% CI 5.3–15.1%). The average length of time from starting the treatment to SCAR-related death was 297.98 days (median 304 days, IQR 296–310 days). In patients with CKD, the incidence of allopurinol-related SCAR was 0.46% (95% CI 0.34–0.61%) in the study population. Characteristics of patients are shown in Supplementary Table 3 (available with the online version of this article).
Costs
Supplementary Table 4 (available with the online version of this article) shows the total medical costs for patients with allopurinol-related SCAR. The average medical costs for each allopurinol-related SCAR hospitalization was NT$113,285 (median NT$40,760, IQR NT$17,309–113,562). For the 132 patients who survived SCAR, the mean medical costs were NT$92,091 (median NT$31,119, IQR NT$47,393–311,939). The medical costs increased in the 15 deceased patients, with mean cost being NT$264,140 (median NT$140,151, IQR NT$67,567–224,192).
Results of cost-effectiveness analysis
Table 2A shows the results of the base-case analysis. Two strategies dominated: febuxostat without genotyping (i.e., higher price), and allopurinol without genotyping (i.e., less effective). Compared with benzbromarone without screening, genetic screening with allopurinol had an additional cost of NT$2620, but added 0.00012 life-years and 0.01117 QALY. The estimated incremental cost-effectiveness ratio (ICER) of genetic testing was NT$21,651,688 per life-year saved and NT$234,610 per QALY gained.
Cost-effectiveness analysis in the base-case cohort.
Cost-effectiveness analysis in the subgroup of patients with chronic kidney disease.
The results for patients with CKD are shown in Table 2B. Compared with benzbromarone without screening, genetic testing added NT$2195, 0.00014 life-years, and 0.01089 QALY. The estimated ICER of genetic testing was NT$17,378,777 per life-year and NT$230,925 per QALY.
Figure 2 shows the results of the 1-way sensitivity analyses on the structural assumptions. These sensitivity analyses indicated that the ICER was sensitive to several assumptions: the incidence of SCAR following ULA alternatives, the utility of patients with gout/hyperuricemia, the NPV of HLA-B*58:01 screening, and the cost of genetic testing. When the incidence of SCAR from ULA alternatives in the Taiwanese population was varied from 0 to 0.0001, the ICER was –NT$1,684,609 to NT$11,945,417 per QALY gained.

One-way sensitivity analyses in the base-case cohort. One-way sensitivity analysis results showed the influence of individual variables on the ICER of the genetic screening strategy compared with no screening with benzbromarone. The minus sign at the left bar indicates that ICER decreases as the variables increase. ICER: incremental cost-effectiveness ratio; SCAR: severe cutaneous adverse drug reactions; ULA: urate-lowering agents.
Figure 3 shows probability sensitivity analyses. Genetic testing increased both costs and QALY in the majority of iterations (Figure 3A). Figure 3B shows the acceptability curves for HLA-B*58:01 screening prior to treatment. In the probability sensitivity analysis for the base-case cohort, genetic screening revealed that 70% of the iterations were cost-effective at a WTP of NT$800,000 (US$25,600 in 2015) per additional QALY gained in Taiwan. For patients with CKD, the probability of cost effectiveness was 70% at a WTP of NT$400,000 (US$12,800 in 2015) per QALY. The probability of HLA-B*58:01 screening being cost-effective increased following an increase in WTP.

(A) Cost-effectiveness scatter plot. Each point represents incremental cost (2015 values) and QALY between no screening with febuxostat and no screening with benzbromarone therapy from Monte Carlo simulation with multiple model variables. (B) Cost-effectiveness acceptability curve of genetic screening strategy in base-case cohort and patients with CKD. Cost-effectiveness acceptability curves from the probabilistic sensitivity analysis represent the 10,000 iterations. The probability of genotyping being cost-effective is 70% at a willingness-to-pay over NT$800,000 (US$25,600) per additional QALY gained in the base-case cohort, and NT$400,000 (US$12,800) per QALY in patients with CKD. CKD: chronic kidney disease; QALY: quality-adjusted life-years; $NT = New Taiwan Dollar (US$1 = NT$31.25 in 2015).
The number needed to screen was calculated to assess the effect of HLA-B*58:01 screening at population level. Of allopurinol users, 461 and 225 patients needed to be screened for HLA-B*58:01 to prevent 1 case of SCAR in the base-case cohort and among patients with CKD, respectively (Supplementary Table 5, available with the online version of this article). Thus, the cost of preventing 1 case of SCAR was calculated to be NT$1,220,728 for 461 base-case patients, and NT$595,800 for 225 patients with CKD (using a cost of NT$2648 for HLA-B*58:01 screening).
DISCUSSION
Our study objective was to inform health professionals and policymakers about the cost-effectiveness of genetic screening for preventing allopurinol-related SCAR. Our analysis incorporated the burden of hypersensitivity derived from real-world data and clinical alternatives (benzbromarone and febuxostat) in the model. The base-case analysis, based on available data and most likely clinical assumptions, indicated that HLA-B*58:01 screening prevented SCAR and saved more lives. Although no WTP threshold is universally accepted in Taiwan, the ICER per QALY of genetic screening prior to ULA therapy remained lower than the World Health Organization WTP threshold of US$22,635–67,905 (1–3× gross domestic product per capita, US$22,635 in 2015)38,39, and is considered more cost-effective than alternatives without prior screening in Taiwan.
Hyperuricemia is prevalent in patients with CKD40. It is recommended that allopurinol therapy be started with a low dose and close monitoring in these patients, but the reduction in risk of allopurinol-related SCAR was not significant41,42. According to the incidence estimated by our study, the ICER of HLA-B*5801 screening was lower than for the base-case cohort compared with the same alterative treatment strategies. These study findings suggested that HLA-B*58:01 allele screening before ULA initiation is necessary to prevent potential life-threatening SCAR in high-risk subgroups.
The ICER in our study was sensitive to the safety profile of benzbromarone and febuxostat. Febuxostat has a chemical structure unrelated to allopurinol, and the probability of developing cross-related adverse drug reactions is theoretically low. The incidence of 2% rash was, however, documented among patients taking 80 mg/day of febuxostat in a clinical trial, a level similar to that for allopurinol 300 mg/day43. Since 2008, several reports about tolerability and hypersensitivity to febuxostat have been published23,44,45. Although the immunological causality and true incidence of hypersensitivity reactions remain unclear, we suggest that scenarios linked to febuxostat hypersensitivity including renal insufficiency45 and severe skin reactions44 described in these reports are relevant to our study cohort. Our study’s findings suggest the importance of gathering further evidence about patterns of febuxostat-related hypersensitivity reactions to strengthen the value of febuxostat initiation without genetic information in the target patient population. The price of febuxostat is another influential factor in its initiation.
Although there is a strong genetic association between allopurinol-related SCAR and the presence of HLA-B*58:01 allele, test results must be reliable to make genetic information meaningful for clinical decision making. Based on the prevalence of genetic markers in the population (18%) and estimated incidence of allopurinol-related SCAR (2.2/1000 persons), we calculated that 461 patients needed to be tested for HLA-B*58:01 to prevent 1 case of SCAR. Although the sensitivity and specificity of the HLA-B*58:01 test were reported to be 100%, any possibility of an NPV for the test increased the ICER value per QALY gained.
The economic model was based on the best evidence available, but some limitations remained. First, from an economic perspective, it was necessary to consider a longer period of time to avoid giving excessive relevance to the direct treatment costs associated with one-off genotype screening under assessment. The main goal of our study was to compare the costs, health outcomes, and value of HLA-B*58:01 allele screening for allopurinol-related SCAR prevention. Our study did not consider the lifelong direct costs of care for SCAR-associated complications or benefits gained by avoidance of lifelong complications, such as blindness46,47, which may lead to underestimation of the value of one-off genotyping. For instance, the value of HLA-B*58:01 screening was concluded to be cost-effective with a lifelong time frame from a societal perspective in the Thai population21. On the other hand, inevitably additional uncertainties in both benefits and costs exist in relation to extrapolating evidence over time because of the implicit assumption that outcomes in the short term are good predictors of outcomes in longterm gout therapy. Another study evaluated the cost-effectiveness of HLA-B*5801 over a lifetime horizon, but yielded contradictory conclusions on the longterm value in prevention of allopurinol-induced SJS/TEN20. It is possible that the assumptions of ULA outcomes and costs of gout management increased additional temporal uncertainties in the CEA models. Although the study design differed from ours in many ways, the short-term value of HLA-B*58:01 screening–guided therapy is consistent with that found in the Korean population48.
Second, the actual health utility among patients with hyperuricemia or gout in the initial stages of treatment is unknown. To show differences in value of genetic screening for prevention of rare but life-threatening adverse drug reaction, additional assumptions of utility for patients with SCAR and gout/hyperuricemia were made in our study. Sensitivity analyses revealed that if the utility for patients with ULA therapy remained > 0.53 within the initial stage of treatment, genotyping can be considered cost-effective. Although we used an assumption of switching treatment in the model, in reality health-related quality of life may be considerably different from the base-case value. Further research on this topic is recommended to focus on the health utility for patients with hyperuricemia or gout to ensure the estimated value of genotyping is correct in practice.
Finally, because each country has a different healthcare system and ethnic background, our study results may only be applicable to specific populations, where HLA-B*58:01 is prevalent in the general population and the genetic screening resource is accessible. It is still not clear whether allopurinol hypersensitivity is dose-dependent. Irrespective of genotyping, therefore, all patients should be assessed for risks attributed to allopurinol-related hypersensitivity reactions and closely monitored for signs and symptoms of hypersensitivity.
Our study demonstrated that genotyping can serve as a clinical decision-making support tool to prevent allopurinol-related SCAR, and indicated that HLA-B*58:01 screening is cost-effective compared with prescribing an alternative ULA (i.e., benzbromarone, febuxostat, and allopurinol) option without prior genotyping. Our study results highlight the need for genetic information to prevent severe hypersensitivity reactions and of developing effective interventions to identify and manage patients who are at risk of such life-threatening adverse reactions.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
The authors thank Ying-Jen Hsu and SAS Working Group in the Department of Management of Information Systems, Chang Gung Memorial Foundation, for their technical assistance with electronic healthcare data retrieval. This study was based in part on data from the 2 million random beneficiaries from the longitudinal database (2000–2011) provided by the Ministry of Health and Welfare in Taiwan (Registered number H104006). We express our appreciation to the staff at the Collaboration Center of Health Information Application in Kaohsiung Medical University who assisted with population-based longitudinal database analysis.
Footnotes
Full Release Article. For details see Reprints and Permissions at jrheum.org.
Funded by Kaohsiung Chang Gung Memorial Hospital (BMRPD36).
- Accepted for publication February 3, 2017.
Free online via JRheum Full Release option








{kind=link}
{kind=link}
{kind=link}