

Abstract
Objective. To evaluate the utility of anticytoplasmic autoantibody (anti-CytAb) in antisynthetase antibody–positive (anti-SynAb+) patients.
Methods. Anti-SynAb+ patients were evaluated for antinuclear antibody (ANA) and anti-CytAb [cytoplasmic staining on indirect immunofluorescence (IIF)] positivity. Anti-SynAb+ patients included those possessing anti-Jo1 and other antisynthetase autoantibodies. Control groups included scleroderma, systemic lupus erythematosus, Sjögren syndrome, rheumatoid arthritis, and healthy subjects. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy of anti-CytAb, and ANA were assessed. Anti-CytAb and ANA testing was done by IIF on human epithelial cell line 2, both reported on each serum sample without knowledge of the clinical diagnosis or final anti-SynAb results.
Results. Anti-SynAb+ patients (n = 202; Jo1, n = 122; non-Jo1, n = 80) between 1985–2013 with available serum samples were assessed. Anti-CytAb showed high sensitivity (72%), specificity (89%), NPV (95%), and accuracy (86%), but only modest PPV (54%) for anti-SynAb positivity. In contrast, ANA showed only modest sensitivity (50%) and poor specificity (6%), PPV (9%), NPV (41%), and accuracy (12%). Positive anti-CytAb was significantly greater in the anti-SynAb+ patients than ANA positivity (72% vs 50%, p < 0.001), and 81/99 (82%) ANA-negative patients in the anti-SynAb+ cohort had positive anti-CytAb. In contrast, the control groups showed high rates for ANA positivity (93.5%), but very low rates for anti-CytAb positivity (11.5%). Combining anti-CytAb or Jo1 positivity showed high sensitivity (92%) and specificity (89%) for identification of anti-SynAb+ patients.
Conclusion. Assessing patients for anti-CytAb serves as an excellent screen for anti-SynAb+ patients using simple IIF. Cytoplasmic staining should be assessed and reported for patients suspected of having antisynthetase syndrome and a negative ANA should not be used to exclude this diagnosis.
- ANTISYNTHETASE SYNDROME
- ANTISYNTHETASE AUTOANTIBODY
- POLYMYOSITIS
- DERMATOMYOSITIS
- ANTINUCLEAR ANTIBODY
- CYTOPLASMIC ANTIBODY STAINING
Anti-tRNA synthetase autoantibodies (anti-SynAb) target aminoacyl-tRNA synthetases (anti-ARS), a family of cytoplasmic proteins that catalyze the binding of specific amino acids to their cognate tRNA during protein synthesis. Autoantibodies to 8 distinct anti-ARS have been identified: anti-Jo1 (histidyl), anti-PL-7 (threonyl), anti-PL-12 (alanyl), anti-EJ (glycyl), anti-OJ (isoleucyl), anti-KS (asparaginyl), anti-Zo (phenylalanyl), and anti-TYR (tyrosyl)1,2,3,4,5. As a group, the anti-SynAb are the most common of the myositis-specific autoantibodies (MSA) and are seen in 35%–40% of patients with idiopathic inflammatory myopathy (IIM)6. While anti-Jo1 is the most commonly detected anti-SynAb, occurring in up to 30% of patients with IIM, the other anti-SynAb (non-Jo1) are found in about 20% of patients with myositis, collectively7,8. The MSA segregate patients with IIM into phenotypically homogeneous subsets. Patients are considered to have antisynthetase syndrome if they have an anti-SynAb and 1 or more of the following clinical features, in decreasing order of frequency: myositis, interstitial lung disease (ILD), inflammatory arthropathy, Raynaud phenomenon (RP), “mechanic’s hands,” and fever4. Although many patients with antisynthetase syndrome have myositis [either polymyositis (PM) or dermatomyositis (DM)], the diagnosis can certainly be made in the absence of PM or DM. Because of the lack of overt myopathic clinical features or the characteristic rash(es) of DM, such patients are underrecognized because testing for anti-SynAb (particularly non-Jo1) may not be done in the absence of obvious myositis or other extrathoracic disease manifestations9,10.
ILD is a common feature in myositis, particularly antisynthetase syndrome, occurring in up to 40% of patients with PM/DM and 90% of those possessing anti-SynAb11 and is a major cause of morbidity and mortality12,13. Non-Jo1 anti-SynAb+ patients have a worse survival compared with their Jo1+ counterparts9, perhaps related to the former group presenting with nonmyositis connective tissue disease (CTD) features, including pulmonary manifestations, leading to a delay in both diagnosis and initiation of effective immunosuppressive treatment9. A contributing factor is a delay in ordering or the lack of available and validated commercial testing of the non-Jo1 anti-SynAb. Additionally, a negative antinuclear antibody (ANA) test is commonly reported in these patients. In fact, in 37 patients presenting with clinical features of antisynthetase syndrome and a negative Jo1, none had a positive ANA14. Thus, the negative ANA may potentially direct clinicians away from an autoimmune etiology in patients presenting with clinical features of antisynthetase syndrome, especially ILD, delaying both the diagnosis and treatment and worsening the outcome. Based on these considerations, a better screening test for detecting autoimmune ILD because of antisynthetase syndrome is imperative, especially because testing for the 7 non-Jo1 anti-SynAb is inadequate.
Despite several alternate assays (e.g., ELISA or multiplex bead), detecting ANA by indirect immunofluorescence (IIF) has been used for nearly 4 decades as a reliable screening test for various autoimmune diseases15. The ANA detects IF within the nucleus because of the presence of various ANA, but also exhibits reactivity for antibodies against all types of subcellular structures and cell organelles, including cell surfaces, cytoplasm, nuclei, or nucleoli16. The antigens recognized by IF in the cytoplasm during ANA testing include RNA protein or DNA protein complexes, including the anti-ARS (i.e., the antigen for anti-SynAb) participating in protein synthesis17,18,19. Thus, “cytoplasmic staining” by IF on ANA testing is often observed in patients with anti-SynAb5, but infrequently reported because of its unclear significance. In some clinical scenarios (e.g., acute ILD), this could be used to raise the awareness for antisynthetase syndrome before more specific testing for all anti-SynAb is completed.
Although cytoplasmic patterns on IIF have been observed in patients with anti-SynAb, few reports have addressed the use of such testing as a screening test for these rare autoantibodies. To address this, we assessed cytoplasmic staining by IIF (anti-CytAb) as a screening test for anti-SynAb and compared it with the standard ANA using a large prospective cohort of patients with anti-SynAb evaluated at a single tertiary center over a 2-decade period. This is clinically relevant given that most hospitals send these specialized tests (anti-SynAb, especially non-Jo1) to outside referral laboratories that take considerable time to report results, whereas the ANA by IF is done locally. We evaluated a combination of Jo1 and anti-CytAb as a screening test for anti-SynAb, given that anti-Jo1 testing by ELISA is readily available20.
MATERIALS AND METHODS
Patients
The University of Pittsburgh CTD Registry encompasses more than 3 decades of prospective data and serum collected on consecutive patients with various autoimmune diseases evaluated in the rheumatology outpatient offices or inpatient service at the University of Pittsburgh Medical Center (UPMC). Patients included in our study (case and control groups) were restricted to patients enrolled in the CTD Registry between January 1985 and December 2013. The study design was a case-control retrospective study using prospectively collected data. Appropriate University of Pittsburgh Institutional Review Board approval was given prior to obtaining consent.
Anti-SynAb–positive cases
All patients enrolled in the CTD Registry were tested for anti-SynAb. Anti-SynAb+ subjects had a serum specimen positive for an anti-SynAb, regardless of their underlying CTD diagnosis. Thus, we did not restrict the diagnosis to PM or DM because many patients with antisynthetase syndrome lack overt myositis. The clinical features of our anti-SynAb+ cohort have been previously published and have one of the classic clinical features of antisynthetase syndrome described earlier9.
Control cohorts
(1) Systemic sclerosis (SSc) control group: All SSc patients with 1 of the 3 most common SSc-specific autoantibodies (anticentromere, Scl-70, RNA polymerase III) were enrolled in the CTD Registry from January 2000 to December 2013. They were chosen because they represent phenotypically distinct subgroups of patients with CTD compared with the anti-SynAb cohort and generally have high specificity for SSc with mutually exclusive autoantibodies.
(2) Non-anti-SynAb myositis control group: All patients had a probable or definite diagnosis of PM and DM based on the Peter and Bohan criteria21,22 and 1 of the non-synthetase MSA (excluding anti-SRP because it also produces cytoplasmic staining) and were enrolled in the CTD Registry from January 2000 to December 2013. Although this presents a potential limitation of the use of anti-CytAb as a screening test for anti-SynAb, anti-SRP antibody+ patients represent a clinically distinct phenotype from anti-SynAb+ patients. Further, anti-SRP staining leads to a more diffuse pattern whereas the antisynthetase pattern is more speckled.
(3) Other CTD/healthy control groups: Twenty patients with systemic lupus erythematosus (SLE), 22 seropositive rheumatoid arthritis (RA), 43 Sjögren syndrome (SS), and 16 healthy controls were also included as other control groups. All patients with SLE and RA met the American College of Rheumatology (ACR) diagnostic criteria verified by an experienced rheumatologist while all patients with SS had severe sicca symptoms and a similarly confirmed diagnosis. All anti-SynAb+ patients and controls underwent ANA IIF testing and anti-CytAb determination using the same methodology.
Clinical data
Prospectively collected clinical data in the CTD Registry database was supplemented by a retrospective review of the electronic medical record for missing data.
Serologic data
The initial stored serum samples from the first UPMC visit were used for all autoantibody testing including ANA by IIF, anti-CytAb testing, and myositis-associated and SSc-associated autoantibody testing.
ANA and anti-CytAb testing: All patients with anti-SynAb and control groups were evaluated simultaneously for ANA and anti-CytAb positivity using the standard method for ANA testing at a 1/40 dilution on a commercial HEp-2 substrate. If ANA were detected using a HEp-2 cell substrate, the staining pattern was recorded (speckled, nucleolar, homogeneous, centromere, etc.). If anti-CytAb were identified using the same method as ANA, their pattern was recorded as speckled, diffuse, or both. The final specific anti-SynAb or other specific antibody for SSc, SLE, SS, or RA was not known to the research technician before performing and interpreting the ANA and anti-CytAb determination on HEp-2 cells. Similarly, the subsequent results of IIF testing did not influence the final CTD-specific autoantibody.
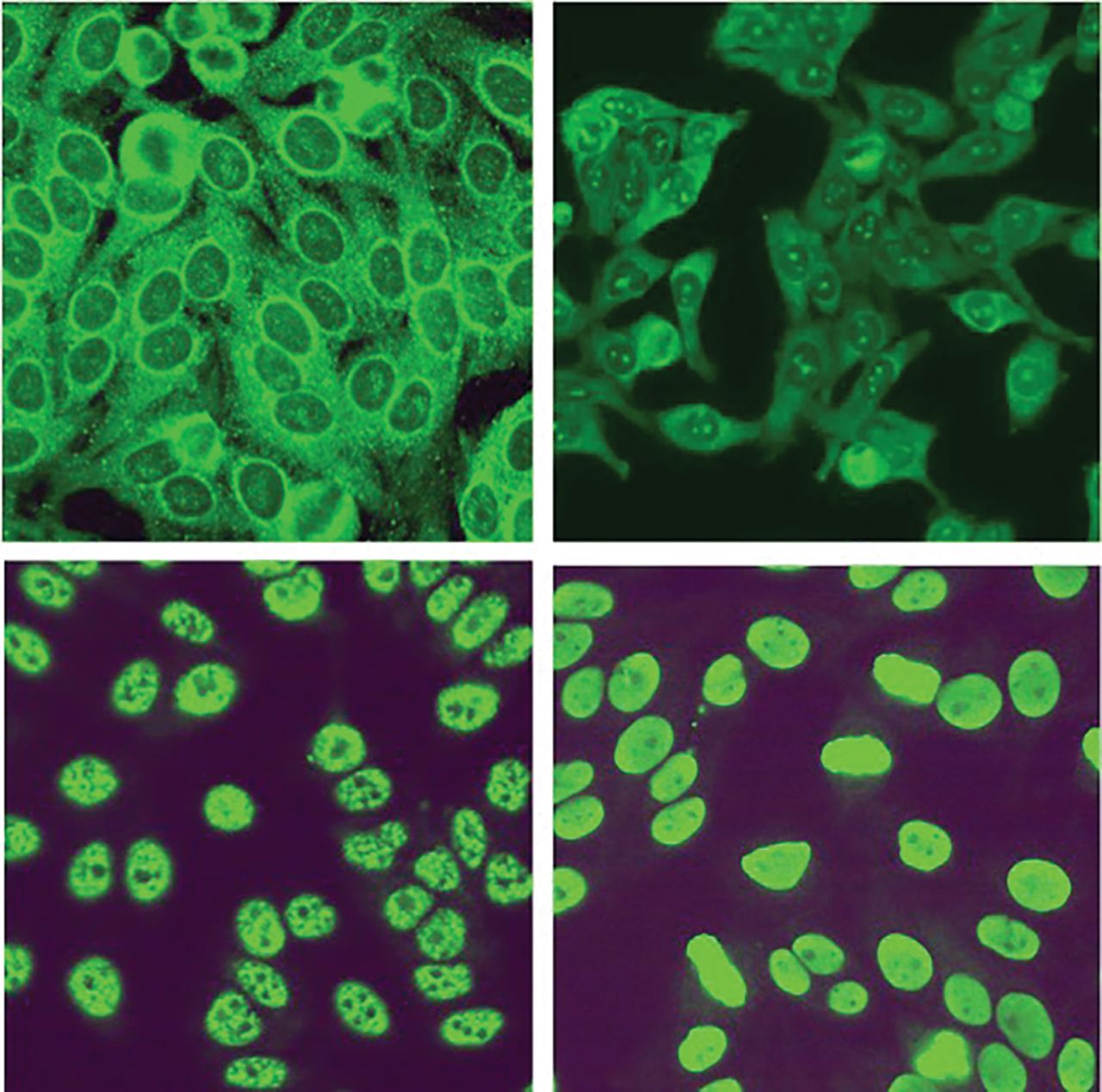
IIF: IIF was carried out with Immuno Concepts HEP-2000 Fluorescent ANA-Ro Test System according to the manufacturer’s protocol. Briefly, 30 μl of serum was placed on the slides and incubated at room temperature for 30 min. The slides were washed with phosphate buffered saline (PBS) for 15 min. Next, antihuman IgG-FITC conjugated was added to the slides and incubated for another 30 min, and the slides were washed with PBS. The staining pattern was identified with a UV microscope using appropriate positive and negative controls (Figure 1).
Myositis autoantibody testing: Anti-Jo1 was determined by protein and RNA immunoprecipitation (IP) and Ouchterlony immunodiffusion. Non-Jo1 anti-SynAb (anti-PL7, anti-PL12, anti-KS, anti-EJ, and anti-OJ antibodies) and other MSA, including anti-SRP antibody, anti-Mi-2 antibody, TIF1-γ antibody, and anti-NXP2, were detected using a combination of protein and RNA IP as previously described23,24,25,26,27. Briefly, a 20 μl serum sample was bound overnight at 4°C to 2 mg Protein A Sepharose CL-4B beads (Amersham Biosciences) and washed 3× with IP buffer (10 mM Tris/HCl pH 8.0, 500 mM NaCl, 0.1% Igepal CA630). For protein IP, the IgG-bound Protein A Sepharose was then re-suspended in 500 μl of IP-buffered 35S methionine–labeled extract from about 1 × 106 rapidly dividing K562 cells and incubated for 2 h at 4°C. The beads were washed 3× with IP buffer, suspended in 2× Laemmli sample buffer, loaded on a standard size 8% gel, and electrophoresed at 200 V. The gel was enhanced with 0.5M sodium salicylate, dried, and autoradiographed for 3–6 days. Apparent molecular weights were determined by comparison with known 14C labeled standards run concurrently. For RNA IP, the IgG-bound Protein A Sepharose was re-suspended in 300 μl NET-2 buffer (50 mM Tris/HCl, pH 7.4, 150 mM NaCl, 0.05% Igepal CA630), and incubated with 200 μl K562 whole cell extract/NET-2 buffer for 2 h at 4°C. After 3 washes with NET-2 buffer, the resultant complexes were re-suspended in 350 μl extraction buffer (NET-2, 0.25 M sodium acetate, 0.83% SDS, 1 μl glycogen) and extracted with 350 μl phenol/chloroform/isoamyl alcohol (50:50:1) plus 0.1% 8-hydroxychloroquinone. RNA samples were ethanol precipitated, dissolved in 20 μl urea sample buffer, resolved on a 7 M urea 8% polyacrylamide gel, and visualized by neutral silver staining. Apparent electrophoretic mobility was compared with controls of known specificity.
SSc-specific and -associated autoantibodies: Anticentromere autoantibody was detected using a HEp-2 cell substrate at 1:40 dilution to prevent missing any possible cases with ANA positivity. In practice, a 1:80 ANA dilution is used, which would further decrease the frequency of ANA positivity reported in our study. Antitopoisomerase I and anti–U1 RNP antibodies were detected by Ouchterlony immunodiffusion24. Sera negative for these latter 3 autoantibodies were examined by IP for 5 other SSc-associated antibodies (anti–RNAP III, anti–PM-Scl, anti-Th/To, anti–U3 RNP, and anti-Ku), as previously reported27. Protein and RNA IP studies were performed as previously described23,24,25,26,27.
Specific autoantibodies for other CTD: Autoantibodies for RA [rheumatoid factor (RF), cyclic citrullinated peptide (CCP)] and SLE (dsDNA, Sm/RNP) were commercially performed.

Anticytoplasmic antibody and antinuclear antibody by indirect immunofluorescence. Top panels show cytoplasmic staining (left with speckled pattern and right with diffuse pattern). Bottom panels show antinuclear staining (left with speckled pattern and right with homogeneous pattern).
Statistics
Descriptive statistics were reported for the frequency of various CTD-specific autoantibodies as well as ANA and anti-CytAb positivity in cases and controls. Two-by-two tables were made for anti-SynAb+ patients versus controls, reporting (1) ANA positivity versus negativity, (2) anti-CytAb positivity versus negativity, and (3) either positivity for anti-Jo1 antibody or anti-CytAb on IIF versus both negative. The following test characteristics of anti-CytAb and ANA as screening tests for anti-SynAb+ patients were assessed: (1) sensitivity [true positive (TP)/TP + false negative (FN)], (2) specificity [true negative (TN) + false positive (FP)], and (3) positive predictive value (PPV; TP/TP + FP), negative predictive value (NPV; TN/TN + FN), and accuracy (TP + TN/total number of patients tested). Chi-square test was used to determine the statistical significance of the difference between ANA and anti-CytAb positivity for all groups and subgroups of patients. All calculations were performed using STATA for Windows statistical software version 10 (StataCorp). Findings were considered statistically significant with a p < 0.05.
RESULTS
Anti-SynAb cohort
Of the 202 total anti-SynAb patients, 122 possessed anti-Jo1 antibodies and 80 had non-Jo1 anti-SynAb [PL-12 (n = 35), PL-7 (n = 25), EJ (n = 9), KS (n = 6), OJ (n = 5)] while 133 were diagnosed as PM (44.6%) or DM (21.3%)21,22. There were 68% women and 83% whites with a mean (SD) age at diagnosis of 47.5 years. Clinical features were those typically reported: 76% ILD, 54% RP, 63% arthritis, 75% myositis, and 48% DM rashes. Detailed clinical features by autoantibody subgroup were previously reported and vary significantly between Jo1 versus other non-Jo1 anti-SynAb9. ANA and anti-CytAb results were available in 199 and 196 patients, respectively.
Control groups
The patients with SSc (n = 741) included 307 (41%) with anticentromere, 192 (26%) with anti-Scl-70, and 242 (33%) with RNA pol III. The autoantibody results in the nonsynthetase myositis control group (n = 223) included 71 TIF1-γ, 52 Mi-2, 25 anti-NXP2, 31 anti-PM-Scl, 8 anti-SAE, 18 anti-MDA5, and 18 anti-SSA antibody. The 22 control patients with RA included 68% with anti-CCP positivity and 86% with RF positivity. The 20 patients with SLE included 6 with anti-dsDNA, 4 with anti-Sm/RNP, 3 with anti-SSA, 1 with anticardiolipin antibody, and 5 who were only ANA+. There were 43 seronegative (anti-SSA/B–negative) patients with SS.
Performance of anti-CytAb as screening test for antisynthetase syndrome
Positive anti-CytAb showed a significantly greater frequency in the anti-SynAb+ patients than ANA positivity (72% vs 50%, p < 0.001; Table 1). This difference was more significant in the non-Jo1 anti-SynAb+ patients compared with Jo1+ patients (Table 1). Anti-CytAb was more sensitive for the non-Jo1 anti-SynAb+ group (81%) compared with the Jo1 patients (66%). Of importance, 81/99 (82%) ANA-negative patients in the entire anti-SynAb+ cohort had positive anti-CytAb. Thus, anti-CytAb showed high sensitivity (72%), specificity (89%), NPV (95%), and accuracy (86%), but only modest PPV (54%) for antisynthetase syndrome (Table 2 and Table 3). Conversely, the ANA showed only modest sensitivity (50%) as well as poor specificity (6%), PPV (9%), NPV (41%), and accuracy (13%) for anti-SynAb+ patients (Table 2 and Table 3).
Frequency of ANA and anticytoplasmic antibody in patients with anti-SynAb and various control groups. Values are n unless otherwise specified.
Two-by-two tables for anti-CytAb, ANA, and the combination of anti-Jo1 or anti-CytAb in antisynthetase syndrome–positive and –negative patients. Values are no. patients.
Performance characteristics of ANA and anti-CytAb for antisynthetase syndrome.
In contrast, the control group of SSc (n = 741) showed very high positive rates for ANA (739/741, 99.9%), but very low positive rates for anti-CytAb (70/741, 9.4%). Among the myositis nonsynthetase control group (n = 223), there were 36 patients (16%) with anti-CytAb and 187 (84%) with ANA positivity. The frequency of ANA and anti-CytAb in other control groups are given in Table 1.
Performance of combination tests
Combining anti-CytAb or ANA positivity to identify anti-SynAb+ patients increases the sensitivity to 90% (177/196), but the specificity decreases dramatically (0.4%) because of the high frequency of ANA positivity in the nonsynthetase groups. Finally, the combination of anti-CytAb or Jo1 positivity shows high sensitivity of 92% and specificity of 89% for the identification of anti-SynAb+ patients (Table 2 and Table 3).
DISCUSSION
Our study suggests that in patients potentially possessing anti-SynAb, anti-CytAb, i.e., a cytoplasmic staining pattern on routine ANA testing by IIF, may offer diagnostic utility even if ANA is reported as negative. The strength of our study is our large, prospectively collected longitudinal database of anti-SynAb+ patients with matched serum samples in which all samples underwent systematic ANA testing by IIF (including reporting for the presence of cytoplasmic staining) followed by subsequent analysis for all myositis-associated and -specific autoantibodies by IP and other techniques. Second, our research laboratory is skilled in these autoantibody detection techniques (on specimens stored at −80°C for many yrs) with a publication record in myositis and SSc spanning several decades with multiple publications23,24,25,26,27. Third, the index test (screening ANA) results were reported without knowledge of the results of either the CTD diagnosis or more specific (i.e., IP) autoantibody results.
As discussed earlier, the finding of a negative ANA in the setting of antisynthetase syndrome is not uncommon because of the cytoplasmic location of the target autoantigens, the anti-ARS. Thus, a negative ANA may incorrectly dissuade clinicians away from considering an autoimmune etiology in some settings. Because isolated autoimmune ILD is occasionally a forme fruste of antisynthetase syndrome (particularly in the non-Jo1 antisynthetase+ patients) and because these patients may present with severe pulmonary manifestations, it is imperative to diagnose and treat such patients promptly. Thus, there is a need for a rapid and sufficiently sensitive and specific serologic marker to establish the autoimmune characteristic of lung disease in these patients. Most rheumatologists and other subspecialists caring for patients with pulmonary manifestations of myositis are cognizant of the Jo1 autoantibody and its clinical features, but that is not the case with the other non-Jo1 anti-SynAb. Compounding this problem is the inability to accurately detect non-Jo1 anti-SynAb in the sera of these patients because of less readily available and validated commercial assays. Moreover, testing of non-Jo1 anti-SynAb is often delayed by weeks because the specimen being sent to specialty laboratories and the results reported in our experience are not entirely consistent among different laboratories doing the testing, thus wasting crucial time in the management of severe ILD associated with antisynthetase syndrome.
We suggest that ordering anti-Jo1 (commercial ELISA) combined with the assessment for anti-CytAb on ANA testing by IIF (an inexpensive and quick screening test) leads to both high sensitivity and specificity for diagnosing autoimmune ILD associated with antisynthetase syndrome. Given that a delay in diagnosis may contribute to worsening outcome in patients with non-Jo1 anti-SynAb9, the earlier recognition and treatment of such patients may favorably affect survival.
The international consensus on a diagnostic laboratory reporting the ANA pattern (ICAP) includes the discussion of reporting a positive ANA when cytoplasmic staining is found28. However, there is no consensus on this topic and no definitive guidelines have been developed in this regard. Although there are several advantages and disadvantages of including cytoplasmic staining as a positive ANA and it continues to be under scrutiny by ICAP, at the very least a cytoplasmic pattern/staining should be reported in addition to an ANA being reported as positive or negative. Currently, the ACR and the European League Against Rheumatism do have clear guidelines on ANA reporting regarding a cytoplasmic pattern28.
Our study has limitations. First, our cohort of patients reflects those referred to a single tertiary care center with pulmonary/rheumatology specializations, indicating potential recruitment bias. Therefore, the data should be interpreted in the context of patients being specifically referred to a tertiary rheumatology (and pulmonary) referral center specializing in the treatment of antisynthetase syndrome where the pretest probability might be high for a rare condition such as antisynthetase syndrome. Whereas in another clinical setting such as community rheumatology practice, even a high specificity of 90% of a diagnostic test might yield a very low post-test probability. Second, we did not assess the anti-CytAb profile of 2 additional anti-SynAb [anti-Zo (phenylalanyl) and anti-TYR (tyrosyl)], the inclusion of which could have led to more positive results. However, these are very uncommon anti-SynAb. Third, control groups were limited especially for SLE, RA, SS, and healthy cohorts given that the database is primarily established for myositis and SSc, as well as by the availability of a baseline serum sample. Additionally, we recognize that cytoplasmic staining includes several patterns such as fine speckled (associated with anti-SynAb), diffuse (associated with anti-SRP), mitochondrial, lysosomal, golgi, actin, vimentin, etc. However, our primary goal was to recognize cytoplasmic staining as positive or negative considering that specific pattern recognition is reported in more specialized immunology laboratories and not in most hospital immunology laboratories. We also recognize that serum samples in patients with autoimmune liver diseases (e.g., primary biliary cirrhosis) can be associated with CTD and may also have anti-CytAb. Fourth, a small number of serum samples has been stored at −80°C for nearly 30 years, potentially leading to sample degradation. However, our state-of-the-art research laboratory has extensive experience in the longterm storage of serum samples and we have routinely completed IP testing on such samples in many previous manuscripts23,24,25,26,27,29,30,31.
Our study emphasizes the importance of assessing for the presence of anti-CytAb by IIF of HEp-2 cells as an initial screening test in patients potentially manifesting antisynthetase syndrome. This is especially useful in those presenting with acute ILD with or without subtle features of a CTD (e.g., rash, RP, polyarthritis). The combination of either anti-Jo1 positivity or anti-CytAb by ANA IIF has very high sensitivity and specificity for identifying patients with antisynthetase syndrome. Thus, cytoplasmic staining should be looked for and reported in such patients potentially leading to earlier diagnosis and more effective treatment strategies. One can speculate that education and increased awareness among rheumatology and pulmonary specialists regarding cytoplasmic patterns on human epithelial cell line 2 will lead to improved care of patients with antisynthetase syndrome.
- Accepted for publication October 19, 2016.








{kind=link}