

Abstract
Objective.To develop and test a new multidimensional questionnaire for assessment of children with juvenile idiopathic arthritis (JIA) in standard clinical care.
Methods.The Juvenile Arthritis Multidimensional Assessment Report (JAMAR) includes 15 parent or patient-centered measures or items that assess well-being, pain, functional status, health-related quality of life, morning stiffness, disease activity, disease status and course, joint disease, extraarticular symptoms, side effects of medications, therapeutic compliance, and satisfaction with illness outcome. The JAMAR is proposed for use as both a proxy-report and a patient self-report, with the suggested age range of 7–18 years for use as a self-report. From March 2007 to September 2009, the questionnaire was completed by the parents of 618 children with JIA in 1814 visits and by 332 children in 749 visits.
Results.The JAMAR was found to be feasible and to possess face and content validity. All parents and children reported that the questionnaire was simple and easy to understand. Completion and scoring appeared to be quick, requiring < 15 minutes. There were very few missing data. Parents’ proxy-reported and children’s self-reported data were remarkably concordant. The JAMAR provided thorough information for the study patients about recent medical history and current health status. It performed similarly across different children’s ages and characterized the level of disease activity and disability well.
Conclusion.The development of the JAMAR introduces a new approach in pediatric rheumatology practice. This new questionnaire may help enhance the quality of care of children with JIA.
In recent years, there has been an increasing interest in parent/patient-reported outcomes (PRO) in juvenile idiopathic arthritis (JIA)1,2,3,4,5. Incorporation of these measures in patient assessment is deemed important as they reflect the parents’ and children’s perception of the disease course and effectiveness of therapeutic interventions. Because the physician’s evaluation of the disease status drives therapeutic decisions, and these decisions are of foremost importance to parents and patients, integration of their perspective in clinical evaluation may facilitate concordance with physician’s choices and compliance with therapeutic prescriptions6,7,8. Thus, information obtained from the parent or the child may contribute significantly to medical decision-making and to the success of patient care.
A number of measures for the assessment of PRO in children with JIA have been developed over the years, including visual analog scales (VAS) for rating of child’s overall well-being and intensity of pain, and questionnaires for the evaluation of functional ability and health-related quality of life (HRQOL)9,10,11,12,13,14,15,16,17,18,19,20. However, other PRO not addressed by conventional instruments, such as evaluation of morning stiffness and overall level of disease activity, rating of disease status and course, proxy- or self-assessment of joint involvement and extraarticular symptoms, description of side effects of medications, and assessment of therapeutic compliance and satisfaction with the outcome of the illness, may provide valuable insights into the influence of the disease and its treatment. Currently, a clinical intrument that groups all PRO used in the assessment of children with JIA does not exist. Such a tool would provide a physician with a thorough and systematic overview of the patient status to be scanned briefly at the start of the visit. This would facilitate focus on matters that require attention, leading to more efficient and effective clinical care.
These considerations led us to develop a multidimensional questionnaire for the assessment of children with JIA in standard clinical care that incorporates all main PRO. We describe this new instrument, the Juvenile Arthritis Multidimensional Assessment Report (JAMAR), and report the results to date with its use in our patient population.
MATERIALS AND METHODS
Development of the JAMAR
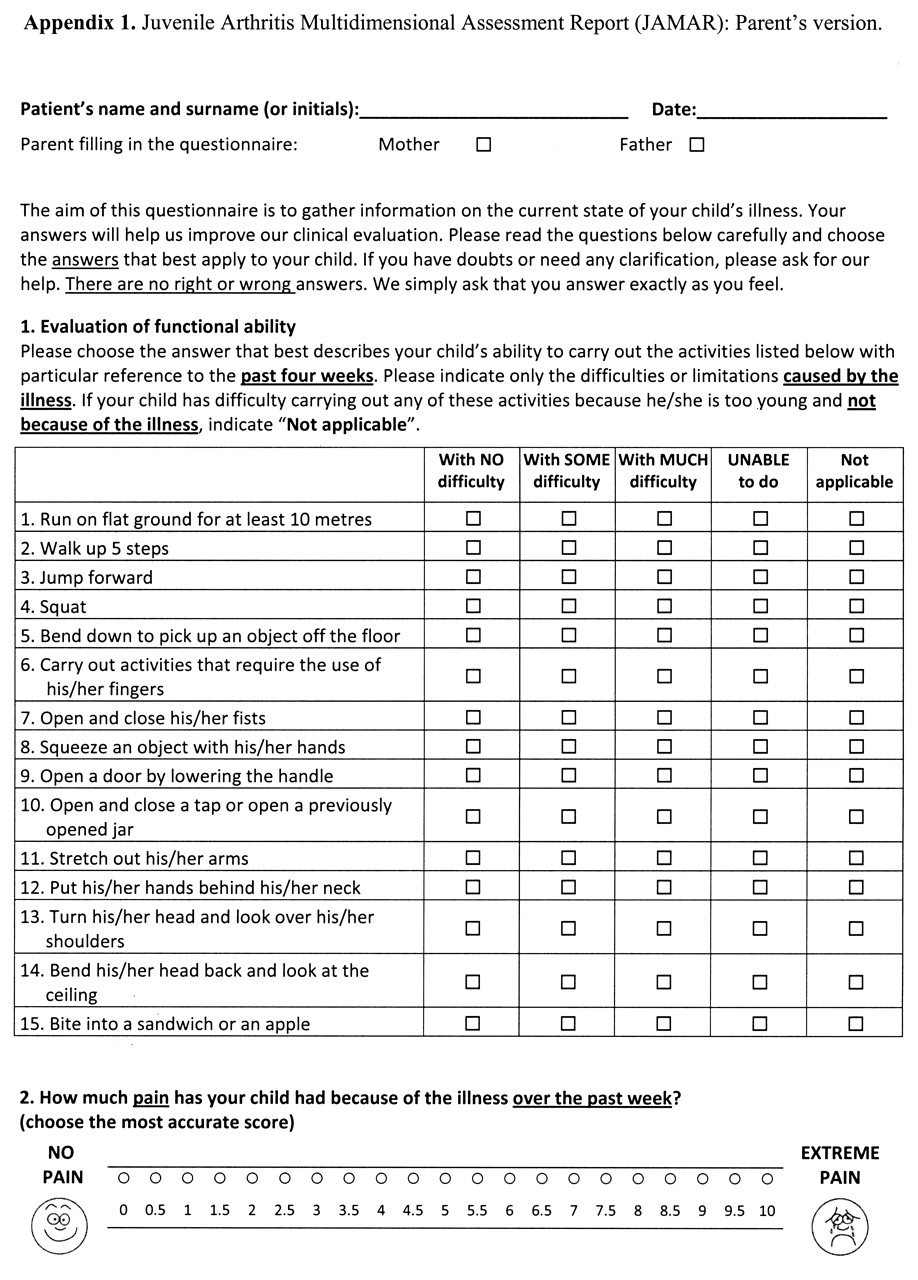
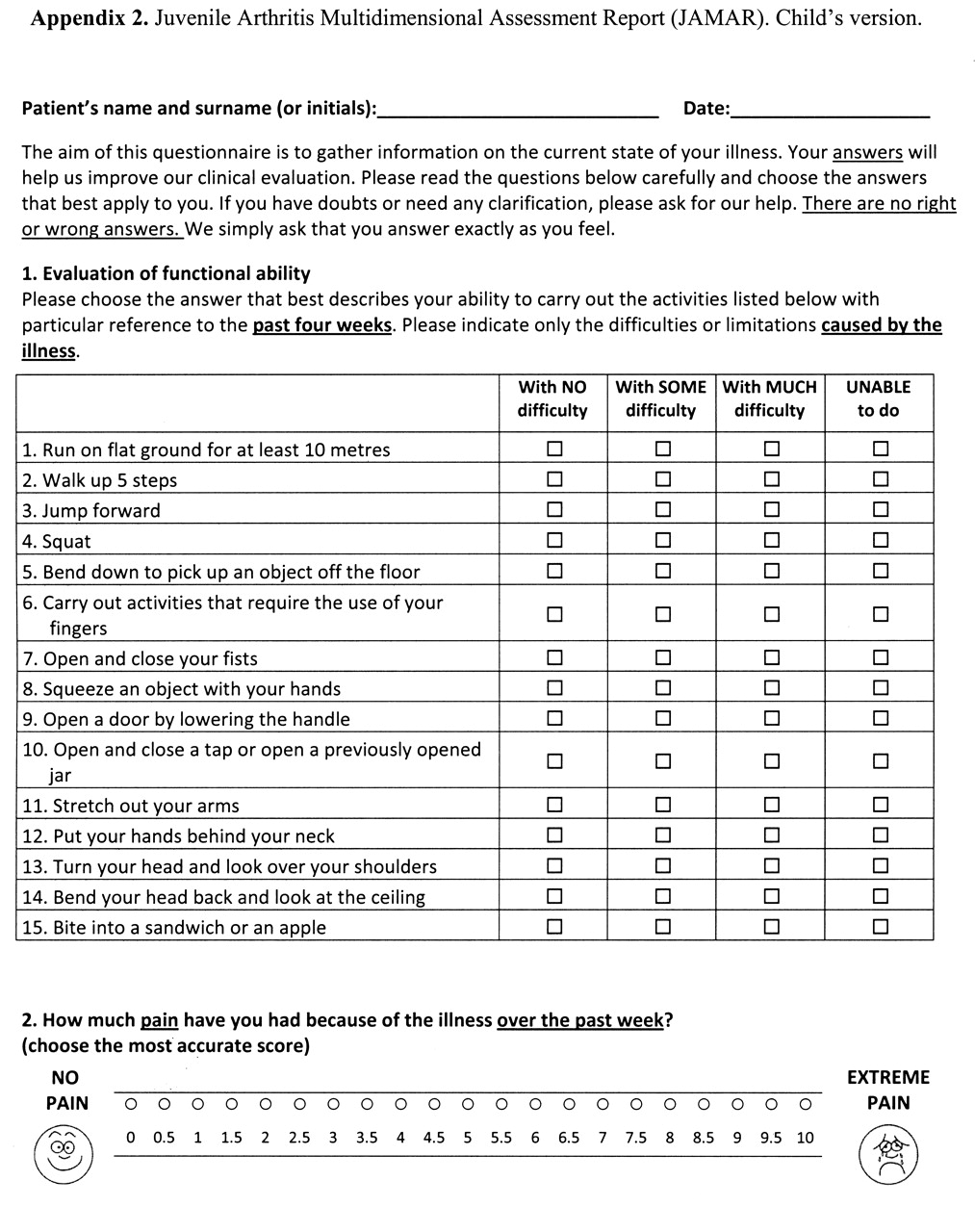
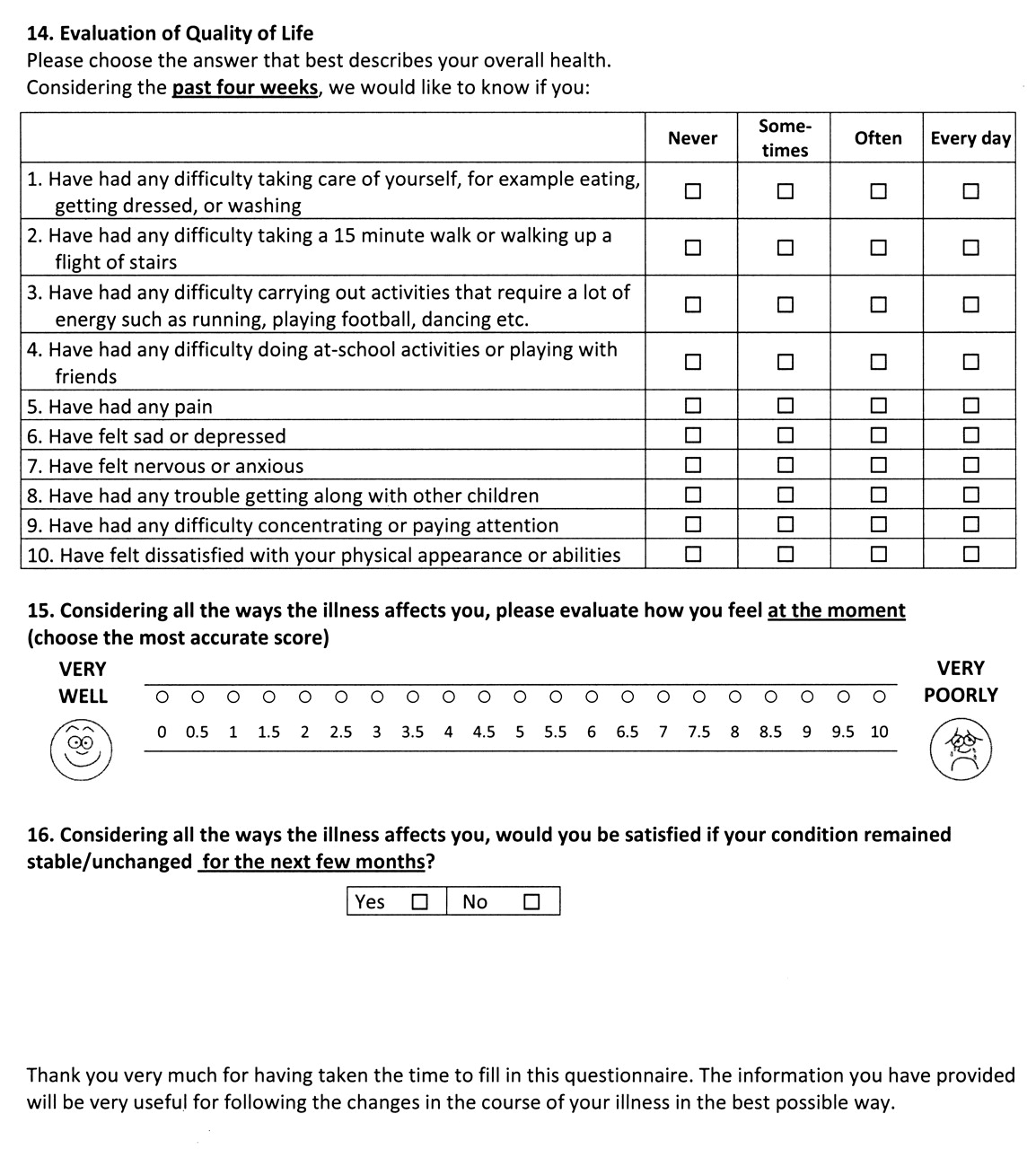
The JAMAR was devised by a group of 7 pediatric rheumatologists (GF, AC, SMM, NR, SV, AM, AR), based on their experience (3 to > 20 years) in clinical assessment of children with JIA, and on a literature review on PRO in adult and pediatric patients with chronic arthritis9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24. To make the JAMAR feasible and practical, it was decided that all measures included in the instrument should be short and easy to complete and score. A total of 32 measures were considered for inclusion in the instrument. After extensive discussion of the relative importance and suitability of each measure, a measure was retained only when there was agreement of at least 6/7 members of the panel that it should be kept in the questionnaire. Thus, content validity was obtained by the members of the panel. The following 15 measures/items were included: (1) Assessment of functional ability, through the Juvenile Arthritis Functionality Scale (JAFS)15. Briefly, the JAFS is a 15-item questionnaire in which the ability of the child to perform each task is scored as follows: 0 = without difficulty, 1 = with difficulty, 2 = unable to do. The total score ranges from 0 to 30. (2) Rating of the intensity of child’s pain on a 21-numbered circle VAS (0 = no pain; 10 = very severe pain)25. (3) Assessment of HRQOL, through the Pediatric Rheumatology Quality of Life Scale (PRQL)20. Briefly, the PRQL is a 10-item questionnaire that includes 2 subdimensions, physical health (PhH) and psychosocial health (PsH), each composed of 5 items. The responses are “never” (score = 0), “sometimes” (score = 1), “most of the time” (score = 2), and “all the time” (score = 3). The total score ranges from 0 to 30, higher scores indicating worse HRQOL. A separate score for the PhH and PsH subscales (range 0–15) can be calculated. (4) Rating of child’s overall well-being on a 21-numbered circle VAS (0 = very well; 10 = very poorly)25. (5) Assessment of the presence of pain or swelling in the following joints or joint groups: cervical spine, lumbo-sacral spine, shoulders, elbows, wrists, small hand joints, hips, knees, ankles, and small foot joints. (6) Assessment of morning stiffness. (7) Assessment of extraarticular symptoms (fever and rash). (8) Rating of the level of disease activity on a 21-numbered circle VAS (0 = no activity; 10 = maximum activity)25. Although the ability of parents/patients to understand the meaning and to be able to report the extent of disease activity may be questionable, we decided to include this VAS to investigate whether it could be a better indicator of the level of disease activity than the well-being VAS. The latter scale has been found to reflect the effects of both disease process and damage, particularly in patients with long-lasting disease26. (9) Rating of disease status at the time of the visit as remission; continued activity; or relapse. (10) Rating of disease course from previous visit as much improved; slightly improved; stable; slightly worsened; or much worsened. (11) Listing of medications the child is taking. (12) Description of side effects of medications. (13) Report of difficulties with medication administration. (14) Report of school problems caused by the disease. (15) A question about satisfaction with the outcome of the illness. Measures 1–6, 8, 9, 10, and 15 had been formally validated or tested in previous studies15,20,25,27,28. Items 7 and 11–14 were not meant to attain validation as they were only descriptive in nature.
To ensure face validity, the draft questionnaire was shown to 12 physicians (8 pediatric rheumatologists and 4 residents in pediatrics), 4 physiotherapists, and 3 specialist nurses who were not part of the JAMAR group, and to 1 clinical psychologist, and their opinion on the suitability of the instrument was queried. Although all agreed on the questionnaire, several points were raised regarding definition of items, which were discussed and partially incorporated in the final version. Face and content validity were tested further by asking a convenience sample of 49 children with JIA and their parents to complete the draft questionnaire and to criticize or comment about the design, content, structure, and response scale. Based on parents’ and children’s input, wording of questions regarding assessment of disease activity and therapeutic compliance, definitions of continued activity and disease flare, and some medication side effects was changed. Further, drawings of happy and sad faces were placed at the 2 ends of the VAS because some parents or, less frequently, children misinterpreted the score rule, particularly regardng the assessment of overall well-being, considering the score 10 as the best and the score 0 as the worst. After these tests, the questionnaire was refined further to reach its final version.
The English translation of Italian versions of the parent proxy-report of the JAMAR for ages 2–18 years and the child self-report for ages 7–18 are presented as Appendixes 1 and 2, respectively.
Patient selection and completion of the JAMAR
A parent or legal guardian of each patient seen at the study units from March 2007 to December 2009 who was ≤ 18 years and was diagnosed with JIA by the International League of Associations for Rheumatology (ILAR) criteria29 was asked to complete the Italian parent-version of the JAMAR at each visit. At the same visits, the child (if aged more than 7 or 8 years) was asked to independently complete the Italian patient-version of the JAMAR. A researcher assisted parents and children if they had questions during questionnaire completion. However, no questionnaire was administered in the form of an interview. All parents/guardians provided written informed consent to participate in the study. The study was approved by the Institutional Review Board of the Istituto G. Gaslini, Genoa, Italy.
Additional clinical assessments
The following data were recorded for each patient: sex, onset age, ILAR category, and disease duration. At each visit, the attending physician rated the overall disease activity on a 21-numbered circle VAS (0 = no activity; 10 = maximum activity)25 and assessed the count of joints with swelling, tenderness/pain on motion, restricted motion, and active disease30. Acute-phase reactants included erythrocyte sedimentation rate and C-reactive protein.
Statistics
Descriptive statistics were reported as medians and interquartile ranges for continuous variables and as absolute frequencies and percentages for categorical variables. Comparison of quantitative data between patient groups was by Mann-Whitney U test in case of comparison of 2 groups and the nonparametric analysis of variance (Kruskal-Wallis test) in comparisons of 3 groups. Comparison of categorical variables between patient groups was by chi-square test or Fisher exact test, as appropriate, in cases of categorical variables. Correlations of quantitative measures included in the JAMAR between questionnaires completed by parents and children were assessed by Spearman’s rank correlation test. All statistical tests were 2-sided; a p value < 0.05 was considered statistically significant. The statistical packages used were Statistica (StatSoft Corp., Tulsa, OK, USA) and Stata release 7 (Stata Corp., College Station, TX, USA).
RESULTS
Patient characteristics and questionnaire completion
A total of 618 children with JIA were included in the study. The demographic and clinical features as well as the values of physician-centered measures and acute-phase reactants of the 618 patients at study entry are presented in Table 1. A parent of each patient completed the JAMAR in a total of 1814 visits. In 749 of these visits, the JAMAR was also completed independently by 332 patients aged ≥ 7 years. All parents and children reported that the JAMAR was simple and easy to understand, with only a few parents and children having questions. Frequent questions regarded the meaning of the word “block” in the HRQOL tool and the way to rate the VAS of disease activity. A random sample of parents and children were asked whether the JAMAR was simple and easy to understand in front of the researchers, and none reported that the questionnaire was too complex or difficult to understand. Completion of the questionnaire appeared to be quick. The mean time for 23 parents and 14 children (aged 8–16 yrs) to complete the questionnaire was 7.2 minutes (range 2.3–11.1) and 8.3 minutes (range 5–13.2), respectively. Scoring of the various components of the JAMAR by a health professional took less than 5 minutes. There were very few missing data in parent- and child-reported questionnaires (Table 2). The center that collected the large majority of the questionnaires (the Istituto G. Gaslini, Genova) is a large tertiary care pediatric rheumatology center, whose catchment area extends to the entire country. The study sample is, therefore, likely representative of the whole spectrum of the educational and cultural background of the Italian children with JIA and their parents. No specific training was provided to questionnaire completers, either children or parents. They were instructed only on the general scope and composition of the questionnaire at the time of first completion.
Main demographic and clinical features, physician-centered measures, and acute-phase reactants of the 618 study patients at study entry. Values are n (%), unless indicated otherwise.
Frequency of missing data in parent and child-reported questionnaires. Values are n (%).
Analysis of questionnaire data
Tables 3, 4, and 5 show results from the 618 questionnaires completed by parents at study entry (left column), and the results obtained at the time of first paired questionnaire completion by 332 children and parents (central and right columns). On average, patients had a low level of physical disability, with a median JAFS score of 0. The physical and psychosocial domains of HRQOL were involved with equal frequency, although, on average, PhH scores were higher (worse) than PsH scores. Only around one-third of patients had a well-being VAS score of 0, but a greater proportion (42.8%) had a pain VAS of 0. Morning stiffness was recorded in 38.3% of patients and 58.9% of patients were reported to have swelling or pain in 1 or more joints. The joints most frequently affected were the knees, followed by the ankles, fingers, wrists, toes, and elbows. The patient’s status at the time of the visit was judged as remission, persistent activity, or disease flare in 44.3%, 30.6%, and 25.1% of instances, respectively. At the second visit, 48.4% of parents rated the disease course from initial visit as improved (much or slightly), 33.4% as stable, and 18.2% as worsened (slightly or much).
Assessment of functional ability, health-related quality of life, overall well-being, pain, and disease activity in the whole questionnaires completed by the parents at study entry and in the first questionnaire completed simultaneously by parents and children. Except where indicated, values are n (%).
Assessment of morning stiffness, joint involvement, disease course from previous visit, disease status, and satisfaction with illness outcome in the questionnaire completed by the parents at study entry and in the first questionnaire completed simultaneously by parents and children. Values are n (%).
Assessment of drug therapies, side effects of medications, therapeutic compliance, and school problems in the questionnaires completed by the parents at study entry and in the first questionnaire completed simultaneously by parents and children. Values are n (%).
It was found that 59.7% of patients were receiving medications at the time of the visit: 33.0% were taking methotrexate, 30.4% nonsteroidal antiinflammatory drugs (NSAID), and 11.3% biologics (most frequently etanercept). Side effects of medications were noted in 27.5% of patients. The most common adverse event was nausea, followed by gastrointestinal discomfort, mood changes, and headache. Problems with therapeutic compliance were uncommon (3.9%). It was found that 30.5% of parents reported that the disease or its treatment caused difficulties at school; 65.9% of parents were satisfied with the outcome of the illness.
Comparison of parent proxy-reported and child self-reported data in paired questionnaires revealed a striking similarity for most items. The only significant difference concerned hypertrichosis as a side effect of medication, which was noted more commonly by parents.
To investigate whether child’s age affected the reliability of completion of the questionnaire, we stratified children into 3 age groups (< 10, 10–15, > 15 years) and compared the parent-child Spearman correlations of quantitative measures included in the JAMAR across age groups. Overall, correlations were comparable, with the exceptions of a lower correlation of functional ability assessment in the younger age group and of psychosocial HRQOL assessment in the older age group (Table 6).
Parent-child Spearman correlations of quantitative measures included in the JAMAR, by child’s age.
To evaluate whether the level of disease activity or disability affected the performance of the JAMAR, we stratified patients in 3 groups based on the number of active joints and the number of restricted joints. We then compared the values of quantitative and categorical measures included in the JAMAR across groups. As expected, the scores of functional ability and HRQOL tools and VAS scales increased (worsened) in parallel with the increase of the number of affected joints. Also as expected, the frequency of remission was lower, and the frequency of continued activity and disease flare higher, in patients with a higher number of affected joints (Table 7). These findings show that the JAMAR components characterize well the differences in level of disease activity and severity.
Values of quantitative and categorical measures included in the JAMAR, by severity of joint disease. Except where indicated, values are median (interquartile range).
DISCUSSION
We have described the development of a new multidimensional questionnaire that combines the traditional patient-reported outcomes used in the clinical evaluation of children with JIA, such as assessment of overall well-being, pain, functional status, and HRQOL, with other PRO not addressed by conventional instruments, including measurement of morning stiffness and overall level of disease activity, rating of disease status and course, proxy- or self-assessment of joint involvement and extraarticular symptoms, description of side effects of medications, and assessment of therapeutic compliance and satisfaction with outcome. The JAMAR enables the registration of all these data in a single instrument in a standardized manner. The questionnaire is not intended to serve as a “measure” for research or clinical trials. Rather, it has been specifically designed for regular administration in daily clinical practice. However, some components that yield quantitative scores (i.e., the physical function and HRQOL tools and the VAS scales) or that are categorical (i.e., assessment of disease state and course, and morning stiffness) can be used in clinical research.
The JAMAR is proposed for use as both a proxy-report and a patient self-report, with the suggested age range of 7–18 years for use as a self-report. The questionnaire format has been found to be very user-friendly, easy to understand, and readily answered by parents and patients. It is quick, taking less than 15 minutes to complete, and can be scanned by a health professional for a clinical overview in a few seconds. Scoring of components can be accomplished in less than 5 minutes and the data are immediately amenable to entry onto a patient’s chart.
Although a number of instruments are available for assessment of PRO in children with JIA9,10,11,12,13,14,15,16,17,18,19,20, most of these measures are not routinely administered in most pediatric rheumatology centers. This is partly explained by the concern that questionnaires may interfere with office routine and time management, with consequent increased costs and time. However, it has been suggested that data from a brief questionnaire designed for standard care can provide an important saving of time (after a brief “learning curve,” as required with any new activity)21. With administration of such a questionnaire, information concerning functional status, HRQOL, global status, pain, morning stiffness, burden of arthritis, disease course from previous visit, and medication side effects are already known by the physician at the start of the visit, rather than when acquiring basic data from the parent. This facilitates focus on matters that require attention, leading to more efficient and effective clinical care.
Over the last 2 years, a simple system has been implemented effectively at the study centers that can assure completion of the JAMAR by almost every parent/patient. In the case of inpatients, the questionnaire is completed the day of hospital admission in the ward room, whereas in outpatients the questionnaire is completed in the waiting area before the patient is called into an examining room. To enhance interest of parents and patients in the questionnaire, it is presented by staff in a cheerful and positive manner as an important component of medical care. Completion of the questionnaire helps the parent and the patient to focus on information needed for care and enhances their capacity to describe concerns in the limited time allotted for a clinical encounter.
The JAMAR has been designed specifically for busy clinical settings, with particular attention to feasibility and acceptability in daily care. To avoid making it too lengthy and complex, we selected 2 simple and short measures for assessment of the central domains of physical function and HRQOL. The VAS for pain, well-being, and disease activity are presented as 21-numbered circles, rather than in the traditional 10-cm horizontal line format, to facilitate scoring without a ruler. Use of the simpler 21-circle horizontal line VAS has been found to increase the precision of parent/patient ratings, particularly regarding definition of remission25. The JAMAR is the first questionnaire to include a proxy- or self-report assessment of articular symptoms.
Regular use of the JAMAR enables keeping a flow sheet of patient’s course over time. A flow sheet may facilitate the recognition of possible changes in functional capacity, pain, fatigue, and psychological status from previous visits22. This method of handling clinical data appears very useful in the management of a chronic disease such as JIA as it allows the clinician to record serial parent/patient data, together with joint examination findings, laboratory tests, medication regimen, and other information.
Our work should be viewed in the light of some potential limitations. The JAMAR may not provide sufficient detail regarding PRO of sleep disturbance, fatigue, coping, and family life. Further development of the JAMAR requires continuing research, with introduction of possible modifications based on clinical experience. We recognize that the way parents and children are asked about compliance may not be sufficiently accurate and that appropriate assessment of therapeutic compliance or adherence requires the use of a more specific and detailed instrument31. Children and parents were told to complete the questionnaire independently. However, since we could not watch all parent-child pairs during completion of questionnaires, we cannot exclude that some parents assisted their children. Although there were very few missing data in child-reported questionnaires, we cannot exclude that some questions/items in the JAMAR may be hard for accurate understanding by younger children. Since juvenile spondyloarthropathy is a particular form of JIA, some measures included in JAMAR may perform differently. Because children with enthesitis-related arthritis were underrepresented in the study sample (2.1%), our findings may be of limited value for this JIA subset. Although we present the English translation of the questionnaires, the instrument was tested in Italian parents and patients. It is possible that children and their parents elsewhere might respond differently to the JAMAR questions due to cultural and language differences. Thus, our results should be confirmed at other sites and in different cultural environments before the new questionnaire is widely adopted.
Development of the JAMAR provides a promising approach to quantitative measurement in standard pediatric rheumatology care. Availability of this new instrument may foster regular use of parent/patient questionnaires in routine practice and contribute to improved quality of care of children with JIA.
Appendix 1




Appendix 2




- Accepted for publication November 15, 2010.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}