

Abstract
Objective. To clarify the role of platelet-derived microparticles (PDMP), which are small vesicles with thrombotic and immunological properties, in systemic lupus erythematosus (SLE), systemic sclerosis (SSc), dermatomyositis/polymyositis (PM/DM), and mixed connective tissue disease (MCTD).
Methods. Plasma levels of PDMP were measured by ELISA, and compared among patients with one of the 4 diseases. Association of PDMP levels with clinical characteristics and medication of the patients was also examined.
Results. PDMP levels were higher in patients with MCTD and SSc than in controls. Multiple linear regression analysis revealed that patients with Raynaud’s phenomenon (RP) showed higher PDMP levels than those without. PDMP levels in individual patients did not fluctuate significantly over several months.
Conclusion. PDMP level is associated with MCTD, SSc, and RP, and could be a novel marker for RP.
Microparticles are small membranes, 0.2–2.0 nm in size, that are released from the plasma membrane following cell activation and apoptosis by various stimuli such as cytokines, thrombin, endotoxins, shear stress, and hypoxia. Microparticles are released by platelets, monocytes, endothelial cells, and erythrocytes, and each microparticle bears antigens from the originating cell. For example, platelet-derived microparticles (PDMP) express platelet-specific antigens, such as CD42b (GPIb) or CD41 (GPIIb/IIIa), while endothelial cell-derived microparticles express CD31 (PECAM-1). These expressions make it possible to identify microparticles originating from various cell types1,2,3,4.
PDMP are the most abundant microparticles in plasma and reflect platelet activation. They express an anionic phospholipid, such as phosphatidylserine, on their external surface because asymmetry of the lipid bilayer becomes dysregulated during microparticle formation2,5. Phosphatidylserine on the outer surface facilitates the formation of coagulation complexes and also initiates coagulation by enhancing the capability of tissue factor6. PDMP thus play an important role in coagulation and thrombosis5. Plasma PDMP levels have been shown to be higher than normal under various clinical conditions, including heparin-induced thrombocytopenia, diabetes, chronic renal failure, acute coronary syndrome, stroke, deep vein thrombosis, sepsis, and atherosclerosis1,2,3,6.
Connective tissue diseases are autoimmune inflammatory diseases accompanied by various vascular lesions including vasculitis, thrombosis, atherosclerosis, and Raynaud’s phenomenon (RP). Recent advances have revealed that microparticles have widespread effects on the immune system, including inactivation of pathogens, release of anaphylatoxins, and induction of cytokine production7,8,9. It has also been demonstrated that microparticles affect immune tolerance and angiogenesis10. It has thus been anticipated that microparticles may function as a biomarker of inflammatory and vascular diseases. As for PDMP, an increase in their numbers has been reported in patients with antiphospholipid antibody syndrome (APS), systemic lupus erythematosus (SLE), vasculitides, and rheumatoid arthritis. This suggests that PDMP play a pathological role in vascular lesions as well as immune disorders11,12,13,14.
Most studies in this area have measured PDMP levels by means of flow cytometry, which is widely used for studying PDMP. However, the flow cytometry method cannot be used in a variety of clinical situations. For this reason, the enzyme-linked immunosorbent assay (ELISA) for PDMP has been developed, and results from the 2 methods have been shown to correlate well (R = 0.722)15,16. ELISA is more effective for quantitative measurement of a large number of samples and the samples can be stored until assayed. In an attempt to use ELISA in clinical settings, we reevaluated the role of PDMP in patients with SLE, SSc, mixed connective tissue disease (MCTD), and dermatomyositis/polymyositis (PM/DM) by ELISA; we found that RP is associated with elevated levels of PDMP.
MATERIALS AND METHODS
Patients
Blood samples were obtained from patients attending the out-patient clinic of Kobe University Hospital; all had provided informed consent. Sample collection was undertaken between February 9 and March 18, 2009. All patients met the criteria for their disease: SLE (n = 88); SSc (n = 33); MCTD (n = 14); and PM/DM (n = 18)17,18,19,20. Serial samples were collected from 18 randomly selected patients with SLE (n = 9), SSc (n = 3), PM/DM (n = 2), and MCTD (n = 4). RP was positive for 9 patients. The control group consisted of 34 healthy volunteers (age 43.7 ± 9.2 yrs, 25 women, 9 men), who provided informed consent. Clinical manifestations and laboratory data were obtained from the medical charts. Characteristics of patients are summarized in Table 1. RP was considered to be present in 41.6% of the patients, determined on the basis of patients’ reports, and defined as positive if it occurred within about a month before the blood draw. Antiplatelet drugs for medication included low-dose aspirin (n = 28), sarpogrelate (n = 26), cilostazol (n = 4), ticlopidine (n = 1), and ethyl icosapentate (n = 1). Vasodilators used included beraprost sodium (n = 18), calcium channel blocker (n = 12), limaprost alfadex (n = 3), and kalliginogenase (kalliginogenase, n = 1).
Patient characteristics.
Sample preparation
Two milliliters of blood was drawn with a 21-G needle inserted into an antecubital vein. Samples were mixed with acid-citrate-dextrose ethylenediaminetetraacetic acid in a Neo-Tube (Nipro, Osaka, Japan), and 1.5 ml of each sample was centrifuged at 8000 ×g for 5 min. Next, 0.5 ml of the supernatant was carefully collected and stored at −20°C. Samples were centrifuged at 8000 ×g for 5 min again before assay, and 200 μl from the upper part of the supernatant layer was used for ELISA to determine PDMP levels.
PDMP measurement
PDMP levels were measured using an ELISA kit (Jimro, Gunma, Japan) in accord with the manufacturer’s instructions15. Samples were incubated in wells precoated with anti-GPIX monoclonal antibody for 3 h. The plates were then washed and incubated with peroxidase-conjugated anti-GPIb monoclonal antibody. Color reaction was measured at 450 nm, assay sensitivity was 31.3–300 U/ml, and maximum PDMP level was set at 300 U/ml.
Statistical analysis
All statistical analyses were performed using Stat Flex version 6.0 (Artech, Osaka, Japan) and R version 2.10.1 (R Foundation for Statistical Computing, Vienna, Austria). For normalization, PDMP levels were raised to the power of −0.5. Differences in PDMP values between categorical characteristics (e.g., male vs female) were assessed with the t test. The relationship of PDMP levels and continuous characteristics (e.g., age) were evaluated by univariate linear regression analysis. Multiple linear regression analysis was also performed to identify independent predictors of PDMP levels. Candidate predictors were age, sex, disease, platelet count, steroid therapy, RP, fingertip ulcer, and the use of antiplatelet drugs and vasodilators. Values of p < 0.05 were considered statistically significant.
RESULTS
PDMP levels in connective tissue diseases
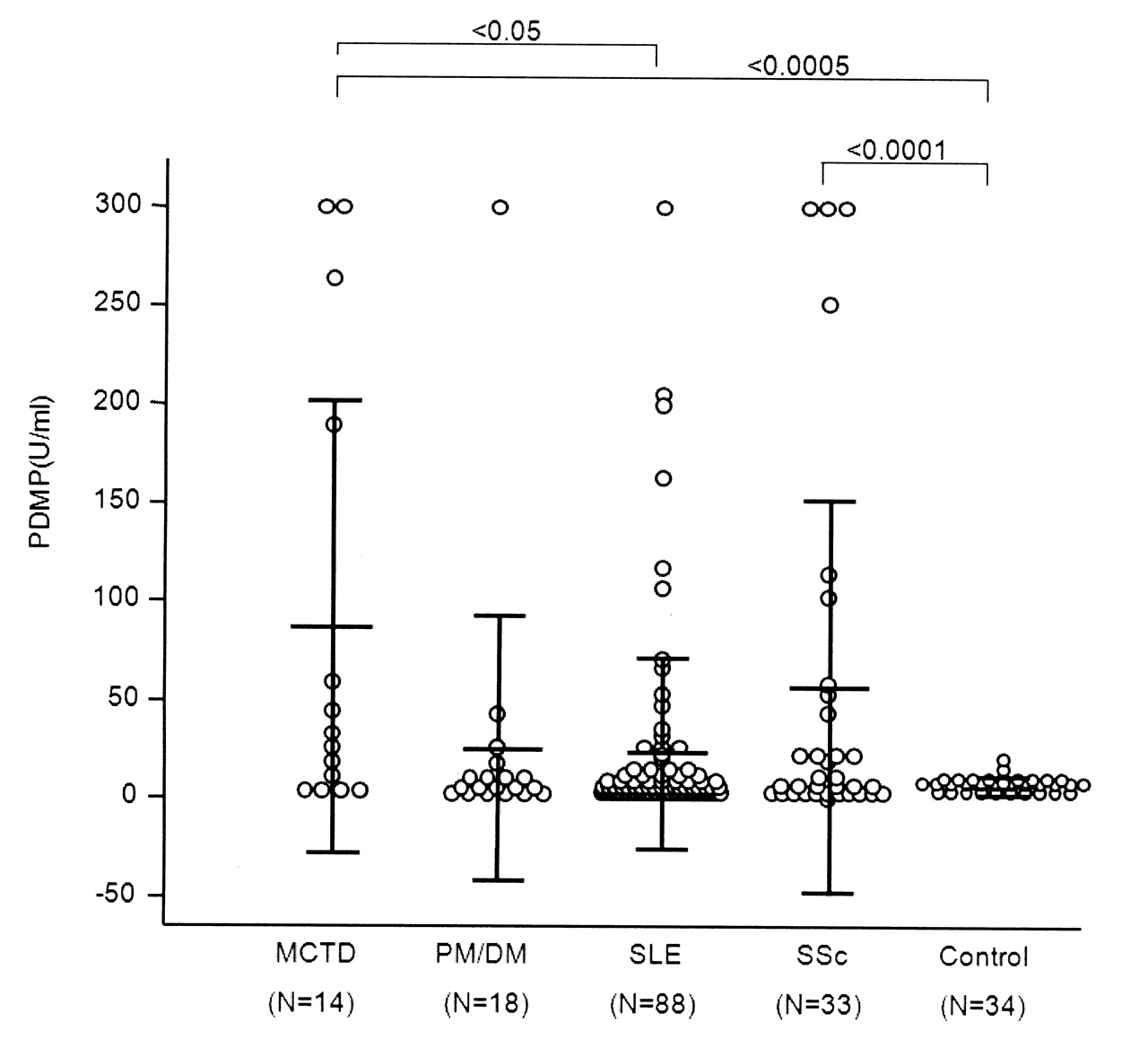
PDMP levels in patients are shown in Figure 1. The mean (± SD) levels for each disease group and controls were MCTD, 90.6 ± 117.1 U/ml; PM/DM, 27.0 ± 68.91 U/ml; SLE, 23.1 ± 48.3 U/ml; SSc, 52.2 ± 92.8 U/ml; and controls, 7.0 ± 4.6 U/ml. PDMP levels were significantly higher for patients with MCTD and SSc than those for controls. Patients with SLE and PM/DM did not show significantly elevated levels of PDMP, although levels tended to be higher compared to controls.
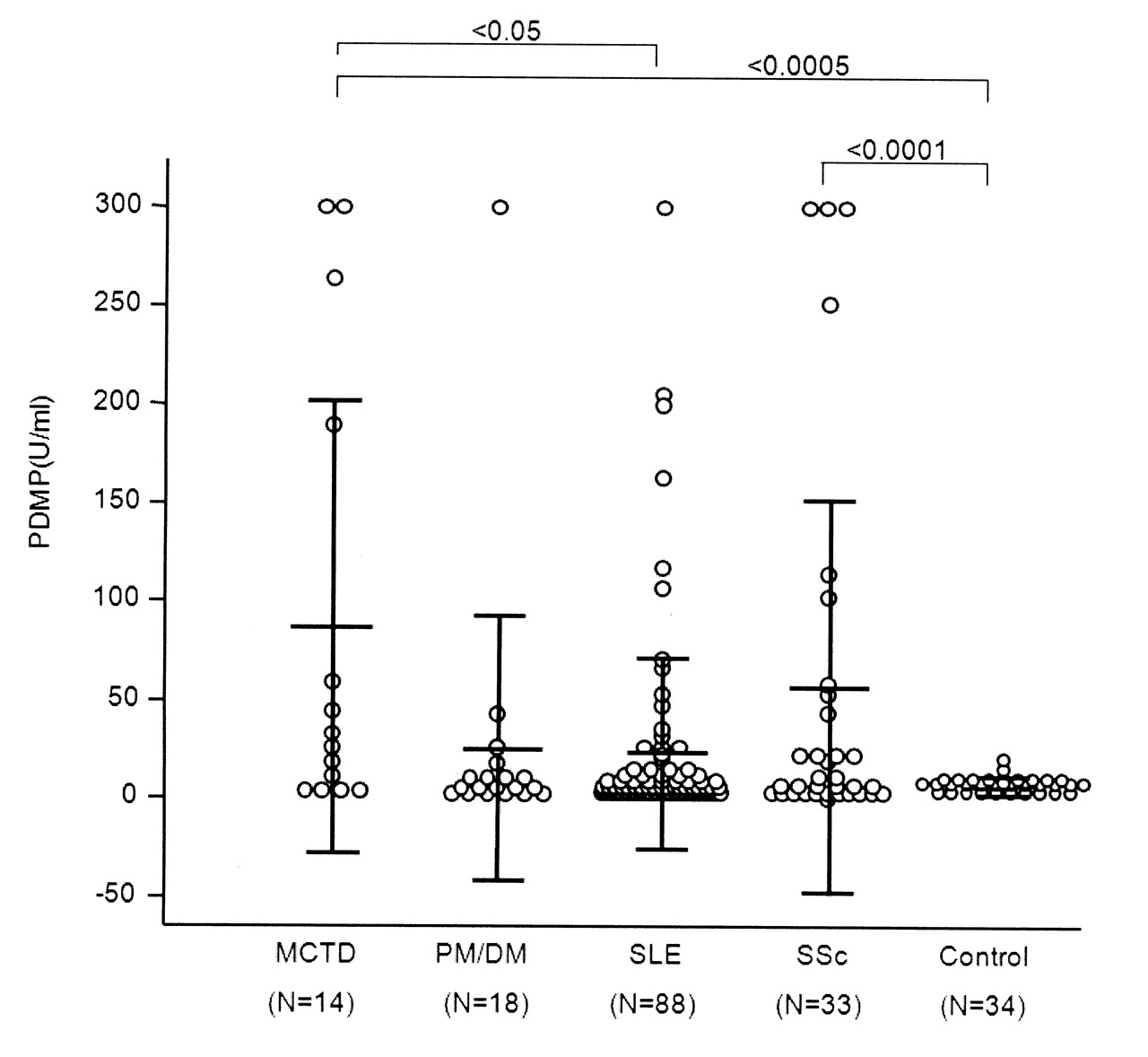
PDMP levels for each disease group. Values are mean ± SD for each group. MCTD: mixed connective tissue disease; PM/DM: dermatomyositis/polymyositis; SLE: systemic lupus erythematosus; SSc: systemic sclerosis.
Comparison of PDMP level and clinical characteristics
Clinical characteristics were assessed for associations with PDMP levels in the patient groups (Table 2). Since RP is a common feature of both MCTD and SSc, we focused on RP and use of antiplatelet drugs when evaluating clinical symptoms. Patients with RP showed significantly higher PDMP levels than those without in univariate analysis (t test, p = 0.005). Other factors, such as age, sex, disease, platelet count, steroid therapy, fingertip ulcer, and antiplatelet therapy, were not associated with level of PDMP. Multiple linear regression analysis identified the presence of RP as the only significant predictor of PDMP levels (p < 0.01; data not shown). PDMP levels for patients with or without RP and for healthy controls are shown in Figure 2 (58.9 ± 97.5 U/ml, 20.4 ± 43.4 U/ml, and 7.0 ± 4.6 U/ml, respectively). Patients with RP showed significantly higher PDMP levels than those without and controls (p < 0.005). Finally, PDMP levels for patients without RP were not higher than those for controls, again substantiating the association of RP with plasma PDMP levels.

PDMP levels for patients with and without Raynaud’s phenomenon. Values are mean ± SD for each group.
Difference of levels of platelet-derived microparticles (PDMP) by patient characteristic.
Time-course analysis of PDMP levels
Serial studies of PDMP levels over several months were conducted in 18 patients to evaluate fluctuations in PDMP levels. Eleven of these patients showed low PDMP levels (≤ 25 IU/ml) and 7 had high levels (> 25 IU/ml), indicating that PDMP levels are relatively stable within individuals (Figure 3). Although PDMP levels fluctuated within each individual, these changes did not show any clear overall trend. One patient with extremely high PDMP levels (> 300 U/ml) always showed similarly high titers. Investigations to determine whether the levels were higher in the cold season and lower in the warm season could not detect any significant differences.

Changes in PDMP levels, measured over 6 months for 18 patients. A. 11 patients showed low levels of PDMP (≤ 25 U/ml); B. 7 patients showed high levels of PDMP (> 25 U/ml).
DISCUSSION
Previous studies, most using flow cytometry, have reported enhanced plasma PDMP levels in patients with SLE, SSc, PM/DM, and other connective tissue diseases1,14. We used a different assay system but found similar results, thus confirming previous findings. We found the highest PDMP levels in patients with MCTD, and this makes ours the first report of enhancement of PDMP levels in patients with MCTD. Consistent with our results, previous studies reported increased PDMP levels for patients with SSc13,21. Guiducci, et al13 reported that PDMP levels are more elevated in patients with limited-type disease than in patients with diffuse disease; and Nomura, et al21 reported that PDMP levels are elevated in patients with interstitial pneumonia. These conflicting results indicate that the role of PDMP in SSc remains unclear.
We found that PDMP level is associated with RP, which is a common feature of SSc and MCTD. Factors contributing to RP include vasoconstriction, vasodilation, endothelial cell damage, and procoagulant tendencies, including platelet activation22. Since PDMP have been reported to cause vasoconstriction and inhibit nitric oxide-dependent vasodilation in animal models23,24, high PDMP levels may be involved in RP through their effect on vasoconstriction. Although we expected that PDMP might contribute to fingertip ulcers because of their thrombotic capacity, we did not find any such association. Consistent with our results, Guiducci, et al reported an inverse association of PDMP with skin sclerosis and fingertip ulcer, implying a possibly negative immunoregulatory effect of PDMP13. However, the difference between involvement of PDMP in RP and in fingertip ulcers remains to be elucidated.
The causes of high PDMP levels in patients with RP remain unclear. PDMP are released when platelets are activated, and platelet activation in patients with connective tissue diseases has been thoroughly reported. One possible cause is therefore that PDMP are released by increased shear stress or reduced blood flow during activation of RP. However, our results show that PDMP levels are relatively stable over long periods and regardless of climate change, indicating that platelets are continuously activated in these patients. We thus speculate that chronic vascular damage in patients with RP may contribute to the release of PDMP, and that PDMP, in turn, could contribute to the occurrence of this phenomenon.
High levels of PDMP appear to be associated with RP rather than with specific diseases because 2 different diseases, SSc and MCTD, are associated with PDMP. On the other hand, we could not find any association of PDMP levels with RP among patients with SLE (positive vs negative: 25.5 ± 53.4 vs 22.6 ± 47.7 U/ml, respectively). One limitation of our study is that other factors related to PDMP could not be fully evaluated. For example, we could not assess whether there is a link between PDMP levels and atherosclerosis in our patients. Further examination is therefore needed to determine the influence of RP on levels of PDMP.
Both ß-thromboglobulin and platelet factor 4 (PF4) are known to reflect platelet activation. An advantage of PDMP as a marker is that, unlike ß-thromboglobulin or platelet factor 4, PDMP are not activated by blood collection. The effect of antiplatelet therapy, including the use of selective serotonin reuptake inhibitor, on PDMP levels remains an interesting question for future studies. Finally, our findings lead us to conclude that PDMP may be an effective marker for monitoring platelet activation, and that ELISA is a quick and easily administered assay for PDMP.
- Accepted for publication November 18, 2010.








{kind=link}
{kind=link}
{kind=link}