

Abstract
Objective. Black Africans reportedly experience a distinctly low risk for atherosclerotic cardiovascular disease (CVD). We investigated whether this protection was present among Africans with established rheumatoid arthritis (RA).
Methods. We determined disparities in CVD risk factor profiles (major conventional: hypertension, dyslipidemia, smoking, and diabetes; other conventional: underweight, obesity, metabolic syndrome, chronic kidney disease, alcohol consumption, tension, depression, and body height; nonconventional: rheumatoid factor status and markers of inflammation) and arterial stiffness (brachial pulse pressure) between 291 black and 335 other (229 white, 64 Asian, and 42 mixed ancestry) consecutive Africans with RA in multivariable regression models.
Results. After adjusting for demographic characteristics and healthcare sector attendance, black Africans had more prevalent hypertension (OR 1.76, p = 0.01) and diabetes (OR 1.90, p = 0.07), smoked less frequently (OR 0.12, p < 0.0001), and had concurrent lower total and high-density lipoprotein cholesterol concentrations that resulted in unaltered atherogenic indices (p = 0.2) than the other participants in the study. These findings translated into global scores for major conventional risk factor-mediated future CVD event rates that were not reduced in black patients. Proportions of individual metabolic syndrome components differed between black and other patients but their total numbers of metabolic risk factors (p = 0.4) and metabolic syndrome frequencies (OR 1.44, p = 0.1) were similar. Black ethnicity did not independently associate with rheumatoid factor status, markers of inflammation, and brachial pulse pressures.
Conclusion. The overall conventional and nonconventional atherosclerotic CVD risk burdens and arterial stiffness were not reduced in black patients with RA. CVD risk should be assessed and managed independent of ethnic origin and epidemiological transition stage in RA.
- ATHEROSCLEROTIC CARDIOVASCULAR DISEASE RISK
- ETHNIC ORIGIN
- EPIDEMIOLOGICAL TRANSITION
- RHEUMATOID ARTHRITIS
The enhanced risk for cardiovascular disease (CVD) in patients with rheumatoid arthritis (RA) is well established1–13. Atherogenesis in RA is mediated by conventional cardiovascular risk factors and disease characteristics, particularly high-grade inflammation1–13. Additionally, interactions between RA characteristics and conventional cardiovascular risk factors can accelerate atherogenesis3,5,7.
In subjects without RA, the major conventional cardiovascular risk factors of hypertension, dyslipidemia, smoking, and diabetes predict the bulk of future cardiovascular events14,15. Most information on CVD originates in developed countries that are largely inhabited by white populations16. However, 80% of the CVD burden now arises in middle-income and low-income countries16. The current increase in incident CVD in poorer populations is attributable to the epidemiological transition induced by socioeconomic development that consists of the emergence of atherosclerotic cardiovascular risk, engendered by nascent hypertension followed by obesity, dyslipidemia, diabetes, and cigarette smoking17.
Until 30 years ago, CVD was reportedly less prevalent in blacks without RA compared to white Americans, but black Americans currently experience more adverse risk factor profiles for atherosclerosis and higher cardiovascular event rates than their white counterparts18–21. Black Africans are presently considered to be at an earlier stage of the epidemiological transition with particularly more favorable lipid profiles and thereby at lower risk for atherosclerosis compared to other Africans19,22. Nevertheless, a recent emergence of risk factors for atherosclerotic CVD has been well documented in this population22–24 and coronary artery disease is now diagnosed in 10% of black South Africans who present to hospital with heart disease25. South Africa is socioeconomically more developed than other sub-Saharan African countries but is further characterized by persistent, vast income and health inequities26.
The INTERHEART investigators recently documented that conventional cardiovascular risk factors associate with acute myocardial infarction (MI) to a similar extent in different ethnic groups and geographical locations worldwide including in Africa16,19. RA is as prevalent in black as in white urbanized Africans27,28. To our knowledge, whether ethnic origin and epidemiological transition stage affects cardiovascular risk in individuals who have developed RA has not been investigated. As part of a recently initiated study on atherogenesis in African populations with RA29, we studied conventional and nonconventional risk factor profiles for atherosclerosis and arterial stiffness. Our aim was to determine whether among Africans with RA, black patients experience a reduced risk burden for atherosclerotic cardiovascular disease.
MATERIALS AND METHODS
We enrolled consecutive patients who met the American College of Rheumatology criteria for RA30 at a public healthcare center (Charlotte Maxeke Johannesburg Academic Hospital) and a private one (Milpark Hospital; Table 1). All invited patients had previously been treated with disease-modifying agents and agreed to participate. The study was approved by the Ethics Committee for Research on Human Subjects (Medical) of the University of the Witwatersrand. Written informed consent was obtained from each patient.
Overall African patients with RA by gender and healthcare center.
Assessments
The recorded cardiovascular risk factor profiles are presented in Table 2 and Figure 1. All patients fasted for at least 8 hours prior to blood sampling. Hypertension was diagnosed in patients with a blood pressure > 140 mm Hg systolic and/or > 90 mm Hg diastolic, and when antihypertensives were prescribed. Dyslipidemia was diagnosed when the atherogenic index [total cholesterol/high-density lipoprotein cholesterol (HDL) ratio] was > 415,31. We assessed current smoking status. Patients with a fasting plasma glucose ≥ 7 mmol/l, or in whom glucose-lowering agents were prescribed, were diagnosed with diabetes. Patients with a body mass index (BMI) < 20 kg/m2 were considered to be underweight32. We used the recently reported RA-specific BMI threshold (> 28 kg/m2)33 in identifying cases with generalized obesity. Patients were classified as having the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATPIII)-defined metabolic syndrome (MetS) using the ethnicity-specific criteria as recently updated by the American Heart Association and the National Heart, Lung and Blood Institute34. The glomerular filtration rate (GFR) was estimated by the Modification of Diet in Renal Disease equation and chronic kidney disease (CKD) was diagnosed when the GFR was < 60 ml/min35. We assessed alcohol consumption (a protective cardiovascular risk factor in subjects without RA)16, and depression and tension were evaluated using the Arthritis Impact Measurement Scales (AIMS)36. Body height was recorded as a cardiovascular risk factor that originates in environmental and genetic factors acting early in life37.

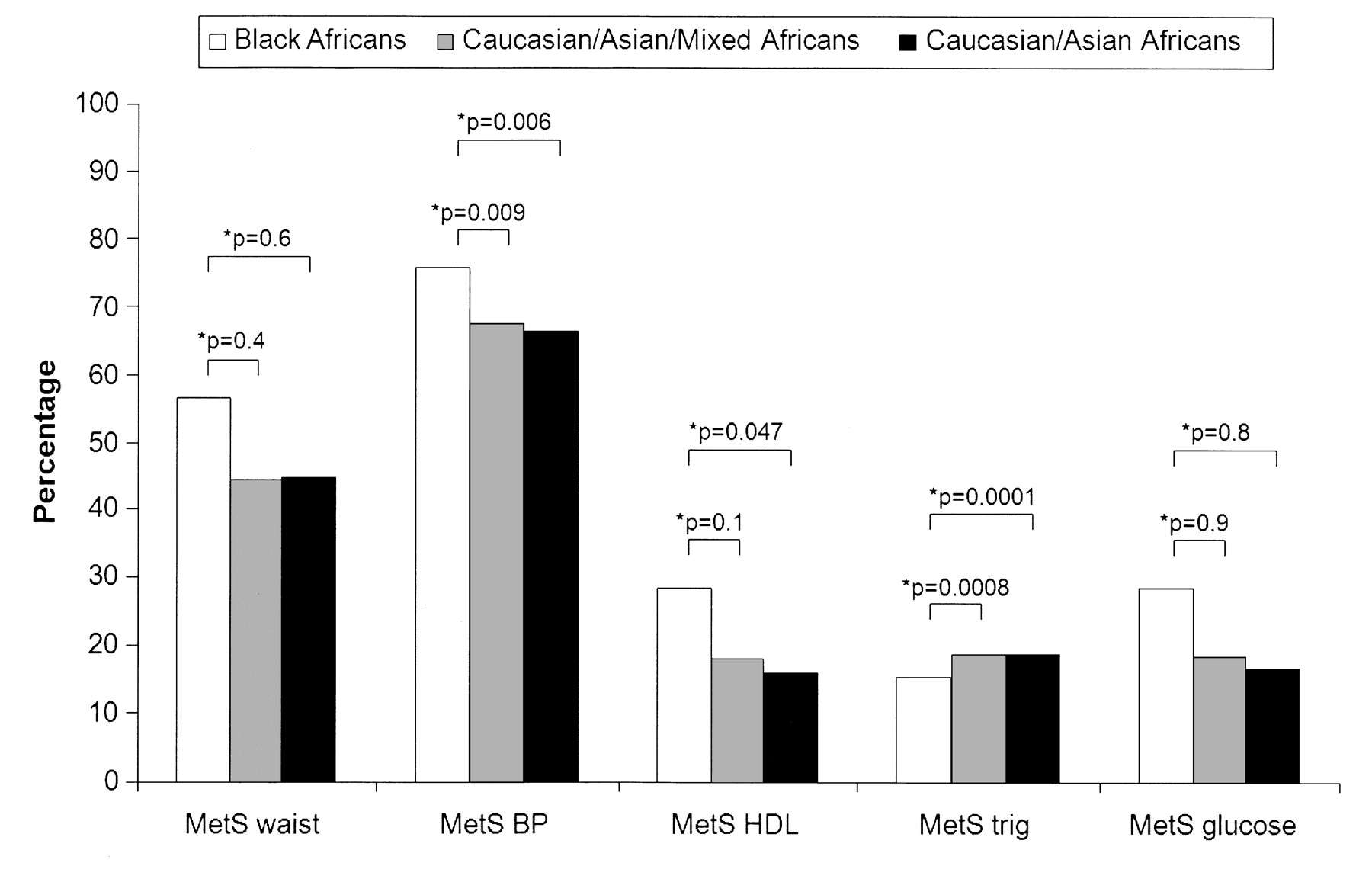
Proportions of the National Cholesterol Education Program Adult Treatment Panel III-defined metabolic cardiovascular risk factors in black and other Africans (before and after exclusion of subjects of mixed ancestry) with RA. MetS: metabolic syndrome; BP: blood pressure; HDL: high-density lipoprotein cholesterol; trig: triglycerides. *Analysis adjusted for age, gender, and healthcare sector.
Cardiovascular risk factor profiles in black compared to white, Asian, or mixed African patients with RA. Significant (p < 0.05) associations of black ethnicity with cardiovascular risk factors in logistic regression models are shown in bold type.
The evaluated RA characteristics considered as potential cardiovascular risk factors included rheumatoid factor status, C-reactive protein (CRP) concentrations, the 28-joint Disease Activity Score (DAS28), the Health Assessment Questionnaire disability index (HAQ-DI), and the number of deformed joints.
Brachial pulse pressure, a marker of arterial stiffness, was defined as the difference between systolic and diastolic blood pressure38–40.
Data management and analysis
We grouped the cardiovascular risk factors into 3 categories. The 1st was the major conventional cardiovascular risk factors, comprising the modifiable risk factors of hypertension, dyslipidemia, smoking, and diabetes, which form part of both the Framingham score14 and the Systematic COronary Risk Evaluation (SCORE)15. These risk factors are the most established ones in atherogenesis in the population without RA. As estimates of the overall major conventional cardiovascular risk burden, we evaluated the mean (SD) number of major risk factors and the proportions of patients who had at least 1 major risk factor as well as those who were at high risk (10-year risk ≥ 20%)14,15 for coronary heart disease (established CVD and/or diabetes and/or a Framingham score of ≥ 20)14 or fatal cardiovascular disease (established CVD and/or diabetes and/or a SCORE of ≥ 20)15. The 2nd risk category was other conventional cardiovascular risk factors, including underweight, generalized obesity, the MetS, alcohol use, CKD, depression, tension, and body height. The 3rd risk category was nonconventional cardiovascular risk factors, consisting of rheumatoid factor status and markers of current (DAS28, CRP, HAQ-DI) and cumulative inflammation (HAQ-DI and number of deformed joints). Except for alcohol use, tension, obesity, and body height, each of the assessed risk factors in this investigation was previously shown to enhance the risk for CVD in not only the general population but also in patients with RA1–13,41–43.
Dichotomous variables are expressed as proportions or percentages and continuous variables as mean (SD). Abnormally distributed characteristics were logarithmically transformed prior to statistical analysis and for these variables, geometric means (SD) are given.
Relationships between black ethnicity and CVD risk were investigated in multivariable logistic and linear regression models as appropriate and with consistent adjustment for age, gender, and healthcare center attendance. Prescribed antihypertensive therapy and statin use were further adjusted upon assessing associations with brachial pulse pressure and lipid values, respectively. Finally, the metabolic cardiovascular risk was further compared between black and other Africans by using the NCEP ATPIII MetS criteria definitions34.
Statistical computations were made using the GB Stat™ program (Dynamic Microsystems Inc., Silver Spring, MD, USA). Since many multivariable analyses were conducted, significance was set at p < 0.01.
RESULTS
A total of 626 patients were investigated, 424 in our public and 202 in our private healthcare center. Eighty-three percent of the patients were either black (46.5%) or white (36.5%; Table 1). Nine black and 168 white patients were seen in private healthcare (p < 0.0001 for each group compared to public healthcare attendance). Asian patients and those of mixed ancestry attended both centers with similar frequencies (p = 0.1 and p = 0.3, respectively). Black patients were more often women and on average 2.9 years younger (Table 2). In all patients, the mean (SD) disease duration was 9.1 (2.4) years, and disease-modifying agents, nonsteroidal antiinflammatory agents, prednisone [mean (SD) dose 4.7 (1.8) mg/day], and statins were currently prescribed in 97.8%, 18.4%, 4.8%, and 6.1% of cases, respectively. None of these characteristics differed in black compared to other patients. However, tumor necrosis factor-α blockers were used only in non-black patients who were seen in private healthcare (n = 6), cyclooxygenase inhibitors were less frequently used in black cases (n = 2 vs 17 in non-blacks), and antihypertensives were more often taken by black patients (53.3 vs 38.5%; OR 1.82, 95% CI 1.32–2.50).
Conventional and nonconventional cardiovascular risk factor profiles and arterial stiffness in black and other African patients with RA
Table 2 shows that hypertension and dyslipidemia were the most prevalent conventional risk factors. The 11% of subjects who used tobacco smoked 11 (SD 2) cigarettes daily and in the 15% who consumed alcohol, the daily intake was 0.9 (SD 0.3) units.
Adjusted for age, gender, and healthcare center attendance, and lipid-lowering agents and antihypertensives when appropriate (Table 2), black patients sustained more prevalent hypertension, less smoking, a trend toward higher diabetes prevalence (OR 1.90, p = 0.07), and lower total and low-density lipoprotein (LDL) cholesterol concentrations but similar cholesterol/HDL cholesterol ratios compared to other Africans. Estimates of the overall major conventional cardiovascular risk burden were consistently similar in black and other Africans with RA. Among the other conventional risk factors, triglyceride concentrations were lower and generalized obesity more prevalent, while the overall prevalence of the MetS did not differ in black compared to other Africans with RA. Alcohol use was less frequent in black patients. Nonconventional cardiovascular risk factor profiles were similar in black and other Africans. Finally, arterial stiffness did not differ in black compared to other Africans.
Mixed-ancestry Africans without RA reportedly still experience a somewhat lower risk for coronary heart disease than white and Asian Africans19. When we repeated these analyses after exclusion of Africans of mixed ancestry, our findings were unaltered (Table 3).
Cardiovascular risk factor profiles in black compared to white or Asian African patients with RA. Significant (p < 0.05) associations of black ethnicity with cardiovascular risk factors in logistic regression models are shown in bold type.
When all the analyses in Tables 2 and 3 were repeated with further adjustment for disease duration, the results were unaltered (data not shown).
NCEP ATPIII-defined metabolic cardiovascular risk in black compared to other Africans with RA
The previous analyses revealed that although black patients with RA experienced an overall similar prevalence of the MetS, the individual MetS risk factors of hypertension frequency and triglyceride concentrations differed in black compared to other Africans with RA. We further analyzed the data in order to clarify whether these relationships persisted once the NCEP ATPIII individual MetS criteria definitions34 were applied. These results are shown in Figure 1. After adjustments for age, gender, and healthcare center attendance, black African patients experienced more prevalent NCEP ATPIII-defined hypertension (OR 1.84 to 2.00), less often elevated triglyceride concentrations (OR 0.37 to 0.43), similar frequencies of abdominal obesity (OR 1.12 to 1.19), reduced HDL cholesterol concentrations (OR 1.46 to 1.71), and elevated plasma glucose concentrations (OR 1.02 to 1.07). The number of MetS criteria in black patients was 2.0 (1.1) compared to 1.7 (1.2) and 1.6 (1.2) in other patients before and after exclusion of people of mixed ancestry, respectively (p = 0.4 after adjustment for age, gender, and healthcare center).
DISCUSSION
Our study revealed disparities in several individual conventional risk factor profiles among black and other Africans with RA. Such findings reportedly reflect different epidemiological transition stages in subjects without RA17,19. Differences in conventional CVD risk factors included a higher prevalence of hypertension and lower smoking frequency in black patients that resulted in an unaltered overall major conventional CVD risk burden relative to other African patients. Similarly, black ethnicity was associated with a lower prevalence of MetS triglyceride concentrations and a higher frequency of MetS hypertension that together translated into a similar overall metabolic risk burden compared to other Africans with RA. Additionally, we found no disparities in nonconventional risk factor profiles between black and other African patients. Finally, and in keeping with an unaltered overall CVD risk burden, arterial stiffness was not reduced in blacks compared to other patients with RA.
Although data on atherosclerotic CVD in sub-Saharan Africa are few19, the increased prevalence of hypertension in our black patients with RA is reminiscent of what was published on black Africans without RA as well as on Americans19,44. Nevertheless, because of factors including a reduced intake of saturated fat, black subjects without RA in Africa reportedly have more favorable lipid profiles than other individuals on that continent19,22,45. It is the low total cholesterol and high HDL cholesterol concentrations in black Africans that are believed to account for the current low prevalence of ischemic heart disease in this population22. In our investigation, black patients had lower total and LDL cholesterol concentrations than other patients with RA. In the general population, the cholesterol/HDL cholesterol ratio exceeds total, HDL, and LDL cholesterol concentrations in predicting incident CVD31. We found that black patients with RA experienced not only lower total cholesterol but also concurrent lower HDL cholesterol concentrations and thereby atherogenic indices or total cholesterol/HDL cholesterol ratios that did not differ from those found in other Africans with RA. Additionally, although the prevalence of diabetes is increasing in black Africans, it is still reportedly lower than in whites living in Africa46. Among Africans with RA in our study, black patients experienced a trend (OR 1.76 to 1.90, p = 0.07) toward a higher prevalence of diabetes in age, gender, and healthcare sector adjusted analysis. Our results on individual major conventional CVD risk factors translated into an overall risk burden for atherosclerosis that was similar in black and other patients with RA, as estimated by the number or presence of one or more of the respective risk factors or being at high risk for incident coronary heart disease or fatal CVD. Importantly in the present context, hypertension is more strongly associated with acute MI in black Africans than in other populations19. Our findings suggest that an earlier epidemiological transition stage, as manifested by the presence of lower total and LDL cholesterol concentrations and less frequent smoking in black Africans with RA, fails to render immunity to the risk of atherosclerosis as it reportedly does in the general black African population19,22.
Other conventional risk factors for atherosclerotic CVD in not only the population at large but also in patients with RA include the MetS and its components6,9, being underweight32, CKD42, and depression41. In our multivariable analyses, black and other patients with RA exhibited similar prevalences of underweight and CKD, and AIMS depression. Except for NCEP ATPIII-defined raised glucose and reduced HDL cholesterol concentrations and abdominal obesity, the frequencies of MetS features differed in black compared to other Africans. This comprised a higher prevalence of elevated blood pressure and less frequently increased triglyceride concentrations. Notably, using the National Health and Nutrition Examination Survey, Sumner and Cowie recently reported that, compared to non-Hispanic whites and Mexican Americans, non-Hispanic blacks were more likely to be insulin-resistant despite experiencing lower triglyceride concentrations47. Reduced insulin sensitivity was also found in black Africans without RA48. Despite different individual metabolic risk factor profiles in black compared to other Africans with RA, black patients did not sustain an altered number of MetS criteria and prevalence of the MetS. Our findings indicate that the overall metabolic CVD risk is likely to be similar in black and other Africans with RA and certainly not lower in black patients.
The RA characteristics of current and cumulative inflammation markers constitute documented important nonconventional CVD risk factors in RA4,5,13,42. After adjusting for potential confounders including public healthcare attendance, a surrogate for socioeconomic disadvantage in our context26,49,50, the inflammatory burden did not differ in black compared to other Africans with RA. Interestingly, and in agreement with our findings, Iren and colleagues recently reported no differences in HAQ-DI and DAS28 in black compared to white Americans with RA, when adjusted for confounders including socioeconomic status51.
Increased brachial pulse pressure strongly associates with the prevalence and incidence of CVD, and its risk factors are generally similar to those for atherosclerosis38–40. We found that the mean brachial pulse pressure did not differ between black and other patients in multivariable analysis. These findings substantiate the notion that the overall risk for atherosclerotic CVD is unlikely to be reduced in black Africans with RA.
We prospectively evaluated detailed CVD risk factor profiles in 626 consecutive patients with RA. We did not perform a power analysis prior to the initiation of our study. However, based on our results, a minimum of 15, 34, 46, and 158 patients needed to be included in the 2 groups of African and other patients with RA in order to document a significant (p < 0.01) difference of 1, 1, 1, and 5 mm Hg in the number of major conventional CVD risk factors, the number of MetS components, DAS28, and pulse pressure, respectively, at 80% power. The cross-sectional design of our study precludes drawing inferences on the direction of causality. Also, although an increased brachial pulse pressure reflects arterial stiffness38–40, our current finding of a higher than expected risk for atherosclerosis in black patients with RA calls for the assessment by more direct measures of subclinical cardiovascular disease in future investigations that address the effect of ethnic origin on CVD risk in RA. We are currently addressing these issues.
Although black Africans with RA smoke less frequently and have lower MetS triglyceride concentrations than other Africans with this disease, they experience more frequent hypertension that therefore should be particularly targeted in CVD risk management. Despite potentially different epidemiological transition stages and/or biological factors among African populations, the overall conventional and nonconventional risk burdens for atherosclerotic CVD and arterial stiffness were not reduced in black compared to other patients with RA in our study. CVD risk should be comprehensively assessed and managed irrespective of ethnic origin in individuals who have contracted RA, including those in developing populations.
Footnotes
-
Supported in part by a Medical Research Council grant.
- Accepted for publication December 3, 2009.








{kind=link}