

Abstract
Objective. Rituximab (RTX) therapy is a treatment option in patients with refractory antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV). We investigated the tolerability and clinical efficacy of RTX in a cohort of patients with refractory AAV.
Methods. Clinical and safety data of patients with AAV treated with RTX were retrospectively assessed from the data of a German national registry.
Results. In total, 58 patients were included in this analysis (50/58 with granulomatosis with polyangiitis; 8/58 with microscopic polyangiitis who received at least 1 cycle, 17 patients who received 2 cycles, and 3 patients who received 3 cycles of RTX). Response was classified as complete and partial in 22 (40%) and in 29 cases (52.7%), respectively. Four patients (7.3%) were classified as nonresponders.
Conclusion. RTX was well tolerated with good clinical efficacy in patients with refractory AAV.
Rituximab (RTX) was recently approved in the United States for the treatment of antineutrophil cytoplasmic antibody (ANCA)-associated vasculitides (AAV), based on the results of the randomized RAVE trial, in which RTX was as effective as cyclophosphamide in inducing remission in patients with newly diagnosed or relapsing with generalized disease1. Apart from this situation no treatment recommendation based on controlled trials exists for refractory disease. However, uncontrolled studies and case reports on RTX in patients with AAV refractory to standard therapy also document significant clinical responses2,3,4,5. In 2008 the German Registry of Autoimmune Disease (GRAID) was established to provide further evidence for the effectiveness and safety of RTX in autoimmune diseases6. We describe the results of 58 patients with AAV who were mostly refractory to standard treatment and who received RTX in “real-life” clinical settings.
MATERIALS AND METHODS
Study design
Using the GRAID registry, data from patients with AAV from 42 German centers of rheumatology and nephrology were retrospectively collected with a Web-based electronic case report form. There was a protocol requirement that RTX must have been started on or before August 31, 2008, with the last followup before December 20, 2008, to prevent any influence on treatment decisions.
Patients’ characteristics and assessment of disease activity
A total of 58 patients (30 women, 28 men, mean age 50.2 ± 16.7 yrs) with AAV were documented in the registry and included in the current analysis. Fifty patients had granulomatosis with polyangiitis and 8 patients were diagnosed with microscopic polyangiitis. RTX was given at a mean time of 4.5 ± 6.1 years after diagnosis. The average observation time was 17.5 ± 13.7 months (median 16.8 mo, range 6–56.6). RTX was given twice at a dosage of 1 g two weeks apart (n = 27) or as 4 weekly infusions of 375 mg/m2 (n = 31). Response evaluation was classified based on the physicians’ discretion in 3 main categories: no response and partial and complete response.
Statistical analysis
All patients entered in the registry were included in the safety analysis. For calculation of the clinical outcome, patients had to have at least 1 control visit. Analysis was performed by standard descriptive statistics.
RESULTS
Clinical manifestations and treatment
At baseline, the most frequently reported manifestations were ear, nose, and throat, lung involvement, and fatigue, affecting 66%, 59%, and 60% of all patients, respectively (Figure 1).
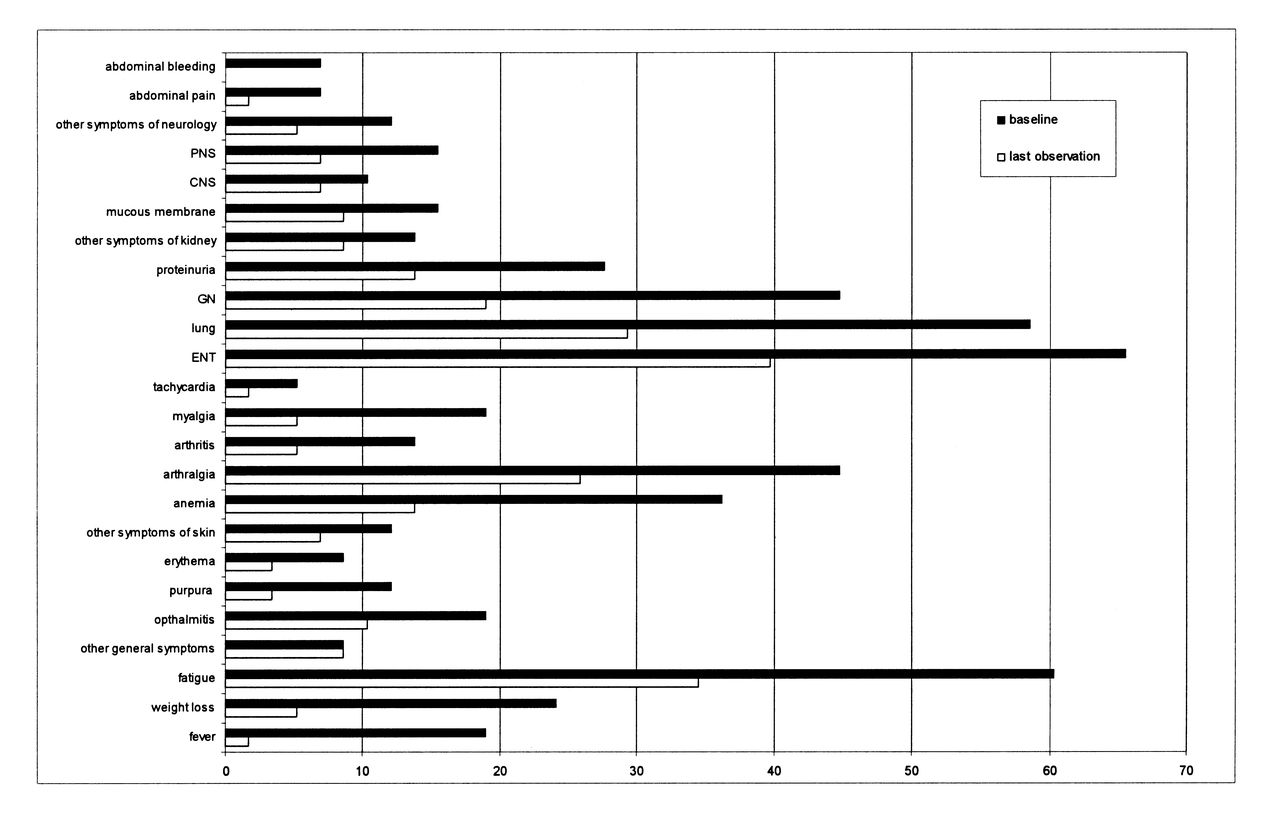
Clinical manifestations at baseline and last control visit of all patients with antineutrophil cytoplasmic antibody-associated vasculitis (n = 58). Data are percentages. PNS: peripheral nervous system; CNS: central nervous system; GN: glomerulonephritis; ENT: ear, nose, and throat.
Fifty-eight patients received at least 1 cycle, 17 patients 2, and 3 patients 3 cycles of RTX. The mean time between the first and second cycle was 17.1 ± 8.2 months, and between the second and third cycle, 12.53 ± 1 months. RTX therapy was discontinued in 11/58 patients: because of adverse events in 1 patient, incomplete response in 5, death in 4, and for other reasons in 1 patient. Previous and concomitant immunosuppressive medications are shown in Table 1.
Proportion of patients receiving immunosuppressive medication in the past, before and during rituximab (RTX), and after RTX treatment (n = 58). Data are number (%).
Clinical outcome
The overall therapeutic response at the end of the observation period was classified as complete remission in 22 cases (40%) and partial remission in 29 cases (52.7%). Four patients (7.3%) were classified as nonresponders. Global therapeutic response was 67% and 62% for renal and pulmonary involvement, respectively (Figure 1).
Safety
Infections were seen in 12/58 patients (20.7%) and were classified as mild in 4, moderate in 4, and severe in 4 patients (each 6.9%). Nine patients had 1 and 3 patients had 2 infections during treatment. The overall rate for infections was 24 per 100 patient-years within an observation time of 61.4 patient-years. For serious infections the overall rate was 6.5 per 100 patient-years. A herpes zoster reactivation was documented in 1 patient. Infusion reactions and allergic reactions leading to discontinuation of RTX therapy were seen in only 1 (1.7%) and 2 patients (3.4%), respectively, of the overall cohort.
Among the 58 patients, 4 deaths were reported following treatment with RTX. Detailed characteristics of these patients are provided in Table 2.
Data for 4 patients who died during therapy with rituximab (RTX).
DISCUSSION
Several uncontrolled studies have explored the use of RTX in patients with AAV refractory to standard treatment, and reported mostly some efficacy in this patient group3,5,7,8,9,10. Complete remission rates in retrospective studies varied between 9.3%7 and 75%8,9. In this report we provide further evidence of safety and clinical efficacy of RTX therapy in patients with AAV refractory to standard treatment, with 40% of patients achieving complete remission and 52.7% reaching a partial remission. Our data have some limitations because of the response evaluation at the physicians’ discretion. However, in a subgroup of 29 patients, a Birmingham Vasculitis Activity Score was available, which declined from a mean of 12.6 ± 7.4 at baseline to 5.4 ± 7.2 at the last control visit, affirming the clinical effect seen in the overall cohort.
In our study RTX was well tolerated, with only 3 patients experiencing an infusion (1 patient) or an allergic reaction (2 patients). The overall rates of infections and serious infections were similar to those reported in uncontrolled trials in AAV3,7,9. The comparable infection rates in our work and other retrospective studies in patients with AAV under standard of care therapy10 do not indicate an increased risk of infections under RTX therapy, considering the use of additional mostly intense immunosuppressive agents in this patient population with refractory disease.
Four deaths occurred, 6.41–13.8 months after the last RTX infusion. Three deaths were related to infection and 1 to fatal cardiovascular complication. However, patients included in this analysis had mostly longstanding and uncontrolled severe disease and were heavily pretreated. Also, randomized studies in AAV have reported a higher mortality rate soon after the start of therapy with RTX11.
Our study has several limitations, mostly related to the retrospective and descriptive study design. Patients in registries are usually a heterogeneous group with mainly difficult-to-treat disease courses and unstable comorbidities. This may reflect more closely the routine clinical spectrum and extend the observations to a broader patient population compared to patients in clinical trials.
Our data support the use of RTX in patients with refractory AAV; in our study the disease showed clinical improvement and RTX treatment was mainly well tolerated in a real-life clinical setting.
Footnotes
-
Supported by F. Hoffmann-La Roche Pharma Ltd.
- Accepted for publication June 28, 2012.








{kind=link}