

Abstract
Objective. To investigate the characteristics and outcomes of patients with systemic lupus erythematosus (SLE)–associated thrombotic microangiopathy (TMA) based on their ADAMTS13 inhibitor profiles.
Methods. The medical data of 31 SLE patients with clinically diagnosed TMA were analyzed. ADAMTS13 activity and ADAMTS13 inhibitor were measured in all patients.
Results. TMA was attributable to active SLE in 19 patients. ADAMTS13 inhibitor and severe ADAMTS13 deficiency were detected in 6 of them. Patients with ADAMTS13 inhibitor (n = 6) exhibited a lower platelet count (7.3 ± 5.1 vs 25.0 ± 17.8 × 109/l, p = 0.005) and more prevalent central nervous system (CNS) involvement (100.0% vs 23.1%, p = 0.003) than patients without ADAMTS13 inhibitor (n = 13). Patients with ADAMTS13 inhibitor also had mild renal involvement characterized by a higher estimated glomerular filtration rate (112.7 ± 18.0 vs 21.6 ± 12.0, p < 0.001), lower proteinuria level [0.6 (0.2–2.5) vs 8.1 (5.2–14.0) g/d, p = 0.011], and lower mean arterial pressure (95.3 ± 13.6 vs 117.5 ± 13.1 mmHg, p = 0.008) than was observed in patients without ADAMTS13 inhibitor. All patients with ADAMTS13 inhibitor achieved complete remission within 18.6 ± 8.7 days, while 3 patients (23.1%) without ADAMTS13 inhibitor achieved complete remission during a median followup of 5.0 months, even though more patients in this group received therapeutic apheresis (100.0% vs 50.0%, p = 0.021). The chance of complete remission increased by 10.8-fold (HR 10.8, 95% CI 1.8–65.5, p < 0.001) when ADAMTS13 inhibitor was present in SLE-associated TMA.
Conclusion. Acquired ADAMTS13 deficiency is associated with more severe thrombocytopenia and CNS involvement, mild renal involvement, rapid resolution, and relatively good treatment response in SLE-associated TMA.
Thrombotic microangiopathy (TMA) is an uncommon and usually severe manifestation of systemic lupus erythematosus (SLE), characterized by microangiopathic hemolytic anemia (MAHA), thrombocytopenia, organ injury, and pathological features of vascular damage. These features are manifested as arteriolar and capillary thrombosis with characteristic abnormalities in the endothelium and vessel wall1. TMA associated with SLE (SLE-TMA) is usually linked to high mortality and severe organ injury; however, the clinical course, organ injury profile, and outcome can be quite diverse, indicating that heterogeneous pathogeneses might be involved in the development of SLE-TMA2,3,4,5,6. TMA could be a consequence of coexisting antiphospholipid antibodies (aPL), overlapping syndrome, malignant hypertension (HTN), infection, and calcineurin inhibitor toxicity in patients with SLE and should be differentiated from TMA associated with active SLE7,8,9. When considering treatment and outcomes of SLE-TMA, it is necessary to look into the underlying causes.
ADAMTS13 (a disintegrin-like and metalloproteinase with thrombospondin type 1 motif 13) is a protease that cleaves von Willebrand factor multimers, and its deficiency results in unusually large von Willebrand factor multimers and the risk of platelet thrombi in small vessels with high shear rates10. Acquired deficiency of ADAMTS13 due to ADAMTS13 inhibitor results in thrombotic thrombocytopenic purpura (TTP), a life-threatening form of TMA. Reports of acquired ADAMTS13 deficiency in patients with SLE are limited, and the organ injury profile, treatment response, and outcomes of these patients have been described only in case reports11,12,13,14,15.
The aim of our study was to investigate the clinical characteristics of subgroups of patients with SLE-TMA with and without acquired ADAMTS13 deficiency.
MATERIALS AND METHODS
Patient selection
Patient eligibility criteria for the study included fulfilling the 1997 revised American College of Rheumatology classification criteria for the diagnosis of SLE16 and diagnosis of TMA. TMA was clinically defined as fulfilling the following criteria: (1) microangiopathic hemolytic anemia, defined as anemia (hemoglobin < 120 g/l in men and 110 g/l in women) with 2 or more schistocytes per microscopic field at a magnification of 100× and a concurrent increased serum lactate dehydrogenase (LDH) above institutional baseline; (2) thrombocytopenia (platelet count < 100 × 109/l); (3) organ dysfunction, including renal involvement, or involvement of the central nervous system (CNS); (4) normal fibrinogen; and (5) negative Coombs test5,11.
Exclusion criteria for the study included conditions other than active SLE that may cause TMA, such as overlapping syndrome, malignant HTN, drug toxicity, pregnancy, infection, malignancy, and positivity for either serum aPL, including anticardiolipin antibody (ACL), anti-β2-glycoprotein I antibody (anti-β2-GPI), or lupus anticoagulant (LAC)7,8,9. Specifically, total ACL and anti-β2-GPI were assayed with commercially available ELISA kit (Oumeng) according to the manufacturer’s instructions. LAC was assayed with dilute Russell’s viper venom time method, on IL coagulation system (IL), according to the manufacturer’s instructions.
TMA was considered SLE-related if no other causes of TMA were identified.
Blood sampling
At the time of clinical suspicion of TMA and before therapeutic apheresis (TPA) or plasma infusion, blood samples were collected from each patient into 2.7 ml sodium citrate blood collection tubes that contained 0.3 ml of 3.2% buffered sodium citrate solution (citrate concentration 109 mmol/l, BD). For further ADAMTS13 activity and ADAMTS13 inhibitor assays, the blood samples were transferred at 0–4°C to a central laboratory at the Thrombosis and Hemostasis Research Unit, First Affiliated Hospital of Soochow University, within 24 h.
ADAMTS13 activity assay
ADAMTS13 activity was assayed as previously described with modifications, by evaluating collagen binding activity (CBA)17,18. In brief, plasma samples from patients and normal individuals were placed in Slide-A-Lyzer minidialysis units (Pierce) and immersed in a prewarmed dialysis buffer made of 5 mmol/l Tris-HCl, 0.1% Tween 20, and 1.5 mol/l urea, with a pH of 8.3. Dialysis was performed at 37°C for 12 h. An equal volume of the same sample was removed before dialysis and kept at room temperature during the dialysis as a control. The collagen type III binding capacities of the samples were then detected by ELISA. The data were analyzed as the fraction of CBA remaining after dialysis compared with the CBA of the individuals’ baseline samples. One hundred percent minus the residual CBA was regarded as the ADAMTS13 activity. Because the dialysis period was extended to 12 h, the resulting ADAMTS13 activity detected was either 100% or 0%.
ADAMTS13 inhibitor assay
For the ADAMTS13 inhibitor assay, patient plasma was incubated with normal human plasma (9:1) at 37°C for 3 h, and the residual ADAMTS13 activity was measured as described in Zheng, et al19. ADAMTS13 inhibitor was considered positive if the residual ADAMTS13 activity was 0% and negative if the residual ADAMTS13 activity was 100%.
Data collection
The clinical, serologic, and medication data of patients with SLE-TMA were collected. Baseline demographic data were collected at the time of admission.
The study was undertaken in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Peking Union Medical College Hospital in Beijing, China (approval number SK-266). All patients provided fully informed written consent to participate in the study.
Definitions and outcomes
Disease activity was scored for each patient at the time of admission according to the Systemic Lupus Erythematosus Disease Activity Index (SLEDAI)-2000 index20. The glomerular filtration rate (GFR) was estimated according to the Chronic Kidney Disease Epidemiology Collaboration creatinine equation21. Mean arterial pressure (MAP) was calculated with systolic blood pressure and diastolic blood pressure as previously described22. Steroid pulse therapy was defined as administration of intravenous methylprednisolone 1 g/day for 3 consecutive days, followed by ≥ 1.0 mg of prednisone/kg/day. Complete remission was defined as normalization of hematologic variables (hemoglobin ≥ 100 g/l, thrombocytes ≥ 150 × 109/l, LDH < 450 U/l) and renal function [estimated GFR (eGFR) ≥ 80 ml/min/1.73 m2, proteinuria ≤ 0.2 g/d, or negative dipstick for urine protein], and resolution of CNS syndromes. Partial remission was defined as normalization of hematologic variables, but with CNS or renal sequelae23.
Statistical analysis
Quantitative variables were reported as the mean ± SD or median and interquartile range. Categorical variables were compared using Fisher’s exact test. Differences in mean or median values between defined patient groups were compared using Student t test or the nonparametric Mann–Whitney U test. The survival distribution (remission) was compared between groups with the log-rank test. All statistical tests were 2-sided, with significance defined as p < 0.05. All statistical analyses were performed using SPSS software, version 22.0 (IBM).
RESULTS
Baseline demographics and overall disease activities
From January 2015 to August 2017, 62 hospitalized patients with SLE were diagnosed with TMA according to the aforementioned criteria at Peking Union Medical College Hospital, and ADAMTS13 activity was assayed in 31 of these patients, and was 0% in 6 patients. For all patients tested for ADAMTS13 activity, ADAMTS13 inhibitor was further examined and was detected in all 6 patients with undetectable ADAMTS13 activity, and none among those with 100% ADAMTS13 activity. Of the 25 patients without ADAMTS13 inhibitor, TMA was considered SLE-related in 13, while it was attributed to causes other than SLE in 12 (Figure 1).
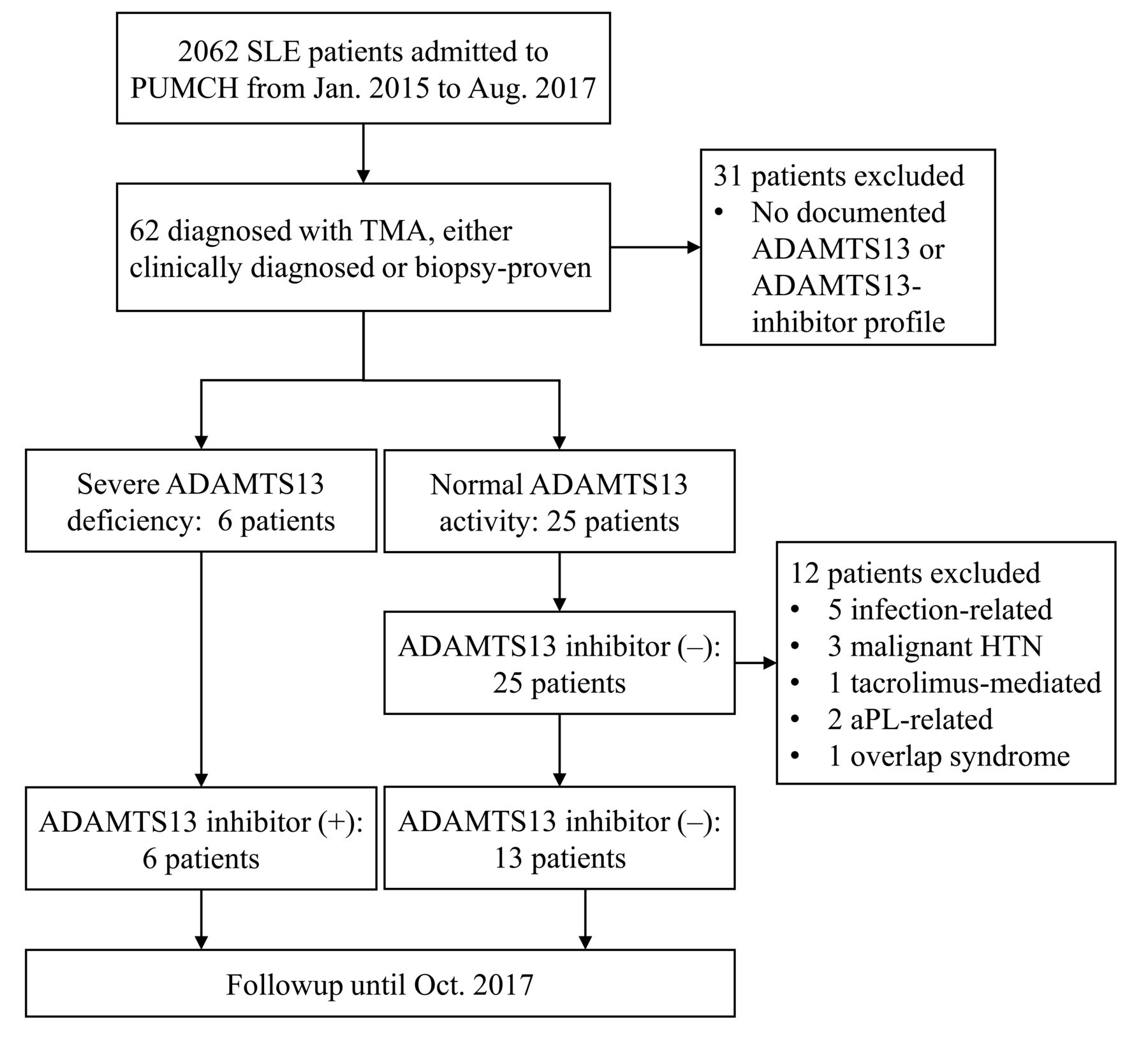
Flow chart of patient selection. aPL: antiphospholipid antibodies; PUMCH: Peking Union Medical College Hospital; TMA: thrombotic microangiopathy; HTN: hypertension.
The baseline characteristics of the 19 patients with SLE-TMA are listed in Table 1. Details of each patient are listed in Table 2. All patients also fulfilled the 2012 Systemic Lupus International Collaborating Clinics classification criteria24. Demographic data were similar between patient groups with and without detectable blood ADAMTS13 inhibitor. All patients had active disease, and there was no significant difference regarding disease activity assessed by SLEDAI between the 2 groups. However, the complement C3 level was significantly lower in patients without ADAMTS13 inhibitor (37.0 ± 17.3 vs 74.9 ± 14.4 mg/dl, p < 0.001).
Baseline characteristics of patients with thrombotic microangiopathy associated with SLE.
Summary of SLE patients with thrombotic microangiopathy.
Hematological abnormalities
ADAMTS13 activity was 0% in all patients with ADAMTS13 inhibitor and 100% in all patients without ADAMTS13 inhibitor. Patients positive for ADAMTS13 inhibitor had a significantly lower platelet count (7.3 ± 5.1 vs 25.0 ± 17.8 × 109/l, p = 0.005) and higher hemoglobin level (62.8 ± 8.0 vs 51.3 ± 11.8, p = 0.046) than patients without ADAMTS13 inhibitor. LDH levels were similar between the 2 groups (Table 1).
Kidney and CNS involvement
The organ involvement profiles were quite different between the 2 groups. Briefly, the patient subgroup with ADAMTS13 inhibitor was characterized by severe CNS involvement, while the kidneys were mostly spared. By contrast, the patient subgroup without ADAMTS13 inhibitor had severe renal involvement, while CNS involvement was relatively trivial (Table 1).
All patients positive for ADAMTS13 inhibitor had CNS involvement, and 5 (83.3%) had severe CNS involvement, including acute confusional states in 4 patients, epileptic seizure in 3 patients, and cerebral vascular disease in 2 patients. By contrast, only 3 patients (23.1%) without ADAMTS13 inhibitor developed CNS involvement.
The eGFR of the patients negative for ADAMTS13 inhibitor was significantly lower than that of patients positive for ADAMTS13 inhibitor (21.6 ± 12.0 vs 112.7 ± 18.0, p < 0.001). Notably, none of the patients with ADAMTS13 inhibitor developed renal insufficiency, and eGFR were above 90 ml/min/1.73 m2 in these individuals, while the eGFR were below 45 ml/min/1.73 m2 in all patients without ADAMTS13 inhibitor, and 4 patients (30.8%) needed renal replacement therapy. The MAP and proteinuria levels in patients without ADAMTS13 inhibitor were also significantly higher than those in patients with ADAMTS13 inhibitor (117.5 ± 13.1 vs 95.3 ± 13.6 mmHg, p = 0.008, and 8.1 (5.2–14.0) vs 0.6 (0.2–2.5) g/d, p = 0.011, respectively).
Treatment
The treatment and outcomes of patients with SLE-TMA are listed in Table 3. Generally, all patients were treated with corticosteroids, and 15/19 patients (78.9%) received steroid pulse therapy. Immunosuppressant regimens including cyclophosphamide or mycophenolate mofetil were adopted for all patients except 1 with ADAMTS13 inhibitor, who was treated with rituximab. There were no significant differences in corticosteroid therapy and immunosuppressants between the 2 groups.
Treatment and outcomes of SLE patients with TMA.
Sixteen patients (84.2%) received TPA, either plasma exchange or double filtrate plasmapheresis. More patients without ADAMTS13 inhibitor received TPA than patients with ADAMTS13 inhibitor (13/13 vs 3/6, p = 0.021). However, the median number of TPA sessions was not significantly different between the groups (Table 3).
Response to treatment
All patients with ADAMTS13 inhibitor achieved complete remission during their hospitalization. The average interval from diagnosis of TMA to complete remission was 18.6 ± 8.7 days. Four patients without ADAMTS13 inhibitor (31.7%) achieved partial remission, 1 (7.7%) achieved complete remission, and 2 (15.4%) died during hospitalization. During a median followup of 5.0 months, partial remission was observed in 6 patients without ADAMTS13 inhibitor (46.1%), and complete remission was observed in 3 (23.1%). When ADAMTS13 inhibitor was present, the chances of both complete remission and partial remission were increased (HR 10.8, 95% CI 1.8–65.5, p < 0.001, and HR 6.9, 95% CI 1.3–37.4, p < 0.001, respectively; Table 3, Figure 2).
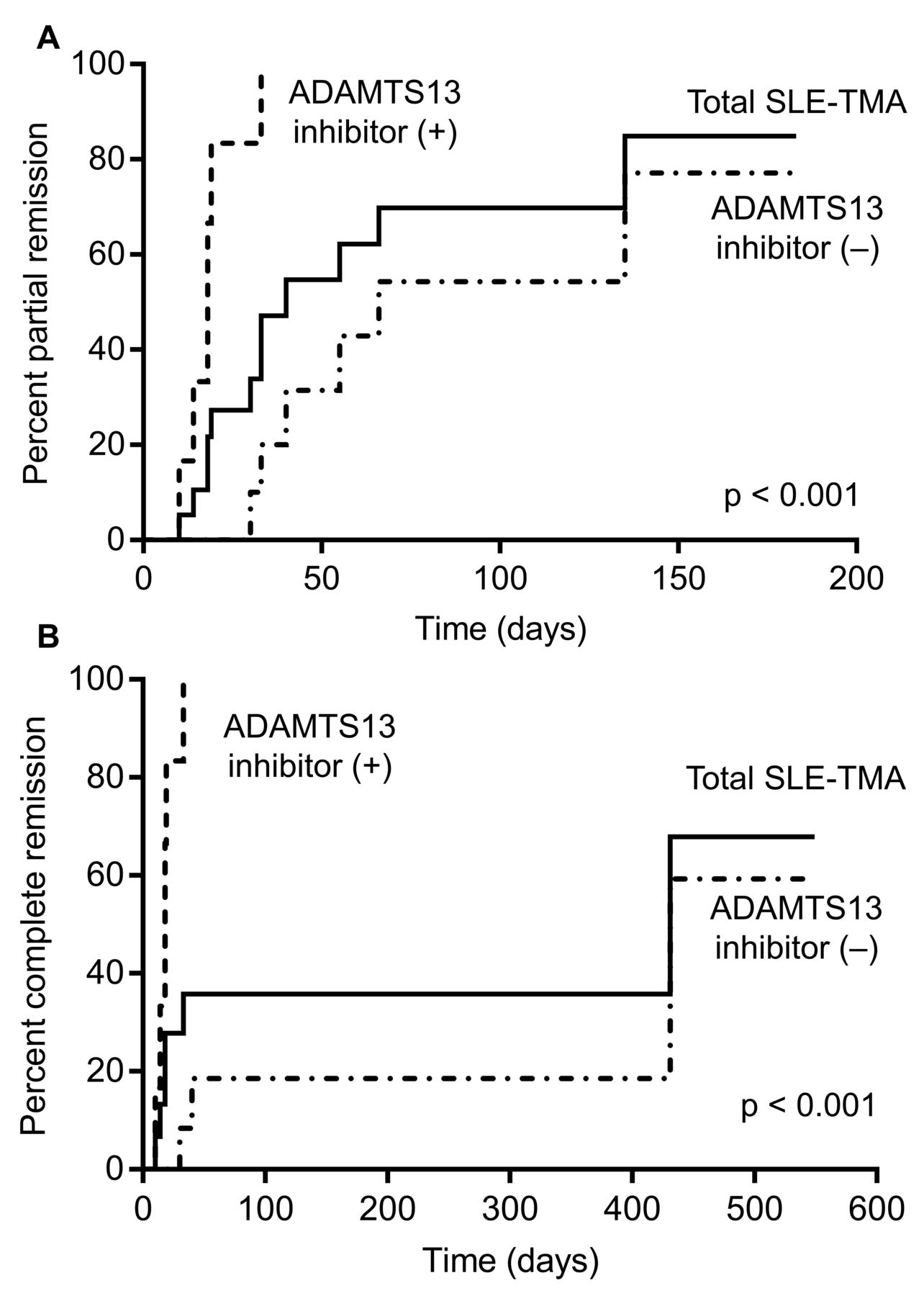
Cumulative incidence of endpoint events in SLE patients with TMA. A. Cumulative incidence of partial remission. B. Cumulative incidence of complete remission. SLE: systemic lupus erythematosus; TMA: thrombotic microangiopathy.
In addition, patients without ADAMTS13 inhibitor had longer hospitalizations (45.1 ± 13.4 vs 30.5 ± 3.4 days, p = 0.005). The hospitalization cost was also higher for patients without ADAMTS13 inhibitor (151.0 ± 78.5 vs 61.3 ± 44.2 × 1000 Chinese yuan, p = 0.019; Table 3).
DISCUSSION
In our study, we identified 2 subgroups of patients with TMA associated with active SLE based on the presence of ADAMTS13 inhibitor, each with unique characteristics. SLE-TMA patients with ADAMTS13 inhibitor were characterized by severe acquired ADAMTS13 deficiency, severe thrombocytopenia, CNS involvement, prompt response to treatment, and relatively good outcomes. By contrast, SLE-TMA patients without ADAMTS13 inhibitor were characterized by normal ADAMTS13 activity, more severe hypocomplementemia, severe renal involvement, and resistance to standard therapy.
Though the overall outcome of patients with SLE-TMA in our study was no better than previously reported, we identified a subgroup of patients (patients with acquired ADAMTS13 deficiency) with a relatively benign outcome, even though these patients presented with extremely low platelet counts and typically severe CNS symptoms. Our findings were consistent with previous research conducted by Matsuyama, et al, who concluded that severe acquired ADAMTS13 deficiency was associated with a lower platelet count and better outcomes in patients with TMA associated with connective tissue diseases (CTD)11. However, the mortality rate of this subgroup of patients in that study was as high as 24%, probably due to the pooled analysis of patients with various CTD11.
The clinical characteristics of SLE-TMA due to acquired ADAMTS13 deficiency strongly resemble those of idiopathic acquired TTP (ai-TTP)13. Considering the pathogenetic role of ADAMTS13 inhibitor in both disease conditions, ai-TTP and SLE-TMA due to acquired ADAMTS13 deficiency might be overlapping disease entities, and we prefer to use the term SLE-TTP to describe the subset of SLE patients with TMA due to acquired ADAMTS13 deficiency12,13,15. SLE-TTP was once considered one of the most fatal forms of SLE-TMA, was usually associated with severe renal insufficiency, and was refractory to treatment, and the reported mortality rate varied from 34% to 62%2,3,4,5,6. However, over time, the concept of TTP evolved significantly, from the original pentad of thrombocytopenia, MAHA, neurological abnormalities, renal abnormalities, and fever to the demonstration of an underlying mechanism of reduced ADAMTS131. Most previous studies addressing SLE-TTP adopted the more classical clinical diagnostic criteria without looking into ADAMTS13 inhibitor and ADAMTS13 levels. As demonstrated by our study, when ADAMTS13 activity and ADAMTS13 inhibitor are considered in the diagnosis of SLE-TTP, the clinical picture of this subgroup of patients can be quite different.
The typical organ injury pattern we observed in SLE-TMA with acquired ADAMTS13 deficiency (SLE-TTP) is consistent with previous reports. A review by Reese, et al reported on 10 children with SLE and acquired ADAMTS13 deficiency14. Renal insufficiency was not observed in any of these patients14. In another study conducted by Song, et al, severe ADAMTS13 deficiency was detected in none of the 36 SLE patients with biopsy-proven renal TMA25. These observations support our finding that SLE-TTP attributable to acquired ADAMTS13 deficiency, and SLE-TMA without ADAMTS13 inhibitor, are different disease entities with distinctive clinical features and pathogenesis.
The role of plasma exchange in SLE-TTP is not clear. Though guidance from randomized clinical trials is lacking, most authors agree that the TPA regimen beneficial in ai-TTP should be used in SLE-TTP26,27. However, in our observation, 3 patients (50.0%) resolved without TPA. The hematological remission was rapid, so TPA was not initiated. Patients with ai-TTP are unlikely to resolve without TPA. Could the difference be due to different underlying pathogeneses of SLE-TTP and ai-TTP? Further studies with larger sample sizes are needed to verify our findings.
Severe renal insufficiency with worsened outcomes in patients with SLE-TMA without acquired ADAMTS13 deficiency might be attributable to a different pathogenic mechanism that has not yet been defined. The nephrotic proteinuria in these patients could not be explained by TMA alone. Two patients (15.4%) underwent renal biopsy, and both showed diffuse proliferative lupus nephritis (LN), along with renal TMA. We assume that SLE-TMA without severe ADAMTS13 deficiency may share a similar pathogenesis with immune complex–mediated glomerular LN. Indeed, complement factor H deficiency has been associated both with the development of complement-mediated TMA with characteristic renal injury and with experimental LN25,28,29. We assume that complement overactivation through both classical and alternative pathways might play a key role in the pathogenesis of SLE-TMA without acquired ADAMTS13 deficiency. The use of a complement inhibitor such as eculizumab may be a promising treatment option for the management of these patients30,31.
Our study had several limitations. First, despite the potential pathogenetic effect of complement activation in patients with SLE-TMA and normal ADAMTS13 activity, complement factors, inhibitors, and potential genetic defects were not assayed in most of the patients. Second, the sample size was small. Considering the fulminant nature of SLE-TTP, the results of this study should be interpreted with caution regarding the treatment of SLE-TTP. These patients should still be treated with the greatest caution until our conclusions are further confirmed with more observations. Third, the followup periods were short. Further observations are needed to clarify the recurrence pattern and longterm outcomes of these patients.
Acquired ADAMTS13 deficiency due to ADAMTS13 inhibitor is associated with more severe thrombocytopenia and CNS involvement, mild renal involvement, rapid resolution, and relatively good treatment response in SLE patients with TMA.
Footnotes
Supported by the Chinese Academy of Medical Sciences (Grant No. 2017-I2M-2-001).
- Accepted for publication May 10, 2018.








{kind=link}
{kind=link}