

Abstract
Objective. To evaluate the involvement of intraarticular (IA) infliximab (IFX) in the management of temporomandibular joint (TMJ) arthritis associated with juvenile idiopathic arthritis (JIA) that is refractory to systemic treatment and IA corticosteroid therapy.
Methods. Ours was a retrospective study of children with JIA who received IA IFX into the TMJ. The effectiveness of treatment on the progression of acute and chronic changes was assessed by a quantitative magnetic resonance imaging scoring system.
Results. Median acute and chronic scores worsened by 0.25 and 0.75, respectively. In multivariate analysis, worsening acute scores and passage of time predicted worsening of the chronic scores.
Conclusion. IA IFX allowed for progression of refractory TMJ arthritis in most but not all children with JIA.
- TEMPOROMANDIBULAR JOINT
- INFLIXIMAB
- INTRAARTICULAR INJECTIONS
- JUVENILE IDIOPATHIC ARTHRITIS
- MAGNETIC RESONANCE IMAGING
Optimal management of inflammatory temporomandibular joint (TMJ) arthritis remains unclear. Present in up to 80% of children with juvenile idiopathic arthritis (JIA), it can lead to longterm destructive changes, with effects on function, discomfort, and cosmetic appearance1. Intraarticular (IA) corticosteroids (CS) have demonstrated a good short-term safety and efficacy profile, but may be effective only in 50% of cases2,3,4,5,6,7. We previously reported the outcome of 24 JIA subjects with recalcitrant TMJ arthritis treated with 1–3 rounds of bilateral IA infliximab (IFX), a tumor necrosis factor inhibitor (TNFi)8. We demonstrated short-term safety, but outcome assessment was hampered by lack of an objective imaging measurement system. Subsequently, we proposed a scoring system for magnetic resonance imaging (MRI) examination of TMJ arthritis that quantifies acute (or active) and chronic findings9. Herein, we applied this MRI scoring system to a larger cohort of children with progressive TMJ arthritis treated with IA IFX to quantify the effectiveness of therapy and further evaluate the MRI scoring system.
MATERIALS AND METHODS
Patients
This was a retrospective single-center study [Children’s of Alabama (CoA), Birmingham, Alabama, USA]. A single oral and maxillofacial surgery group at the University of Alabama at Birmingham (UAB) performed all IA therapy involving the TMJ and maintained a patient file. Inclusion criteria were the diagnosis of JIA according to the International League of Associations for Rheumatology criteria10 and the completion of at least 1 dose of IA IFX therapy. Subjects in our previous study were included in our current study if additional data were available from subsequent injections and MRI. Exclusion criteria were the absence of contrast administration and uninterpretable MRI images from motion artifact. IA IFX therapy was used in children who had refractory TMJ arthritis as evidenced by ongoing inflammation detected by MRI despite therapy with IA CS, and in most cases, systemic immunosuppressive therapy as well.
IFX injections
Injections were performed as described8. Briefly, a 23-g needle was inserted into the superior joint space with location confirmed by positive jaw thrust or return of saline. Up to 1 ml of IFX was injected with the actual amount determined by the joint space such that children typically received 5–10 mg each side (0.5–1 ml). All subjects received bilateral injections even if 1 side was read as normal by MRI because these patients often also had signs and symptoms of TMJ dysfunction bilaterally. In addition, the major risks and discomforts associated with the procedure were the sedation and intravenous placement, which posed the same risk whether 1 side or both were injected. Finally, unlike IA CS, which may itself pose a risk of damage to the TMJ11, IA IFX may not carry the same risks, and the risks associated with systemic exposure are minimal because of the low dose administered. Treatment was approved by the UAB Hospital Pharmacy and Therapeutics Committee. The UAB Institutional Review Board approved our retrospective study.
Data collection
Electronic medical charts were abstracted for clinical and demographic data. Maximal incisal opening (MIO) was measured using the Therabite Measuring Scale (Atos Medical). Baseline MIO was taken at the office visit just prior to initial IA IFX, and followup MIO was done at the visit following completion of therapy.
MRI
All MRI prior to August 2012 (28/33 pre-MRI) were performed with an Ingenia or Avanto 1.5 Tesla (T) scanner (Philips Medical Systems and Seimens Healthcare, respectively) as described12. Afterward, they were performed with a 1.5 or an Ingenia 3T scanner (Philips Medical Systems). TMJ-specific head coils were used with the 1.5T device only. The MRI immediately prior to the first dose of IA IFX was used as the baseline study, and the most recent MRI was used to assess the response to therapy. In-plane resolution (pixel size) varied from 0.5–0.8, and slice thickness was 2 mm with no gap. An illustration of a TMJ MRI with acute and chronic changes is shown in Figure 1.
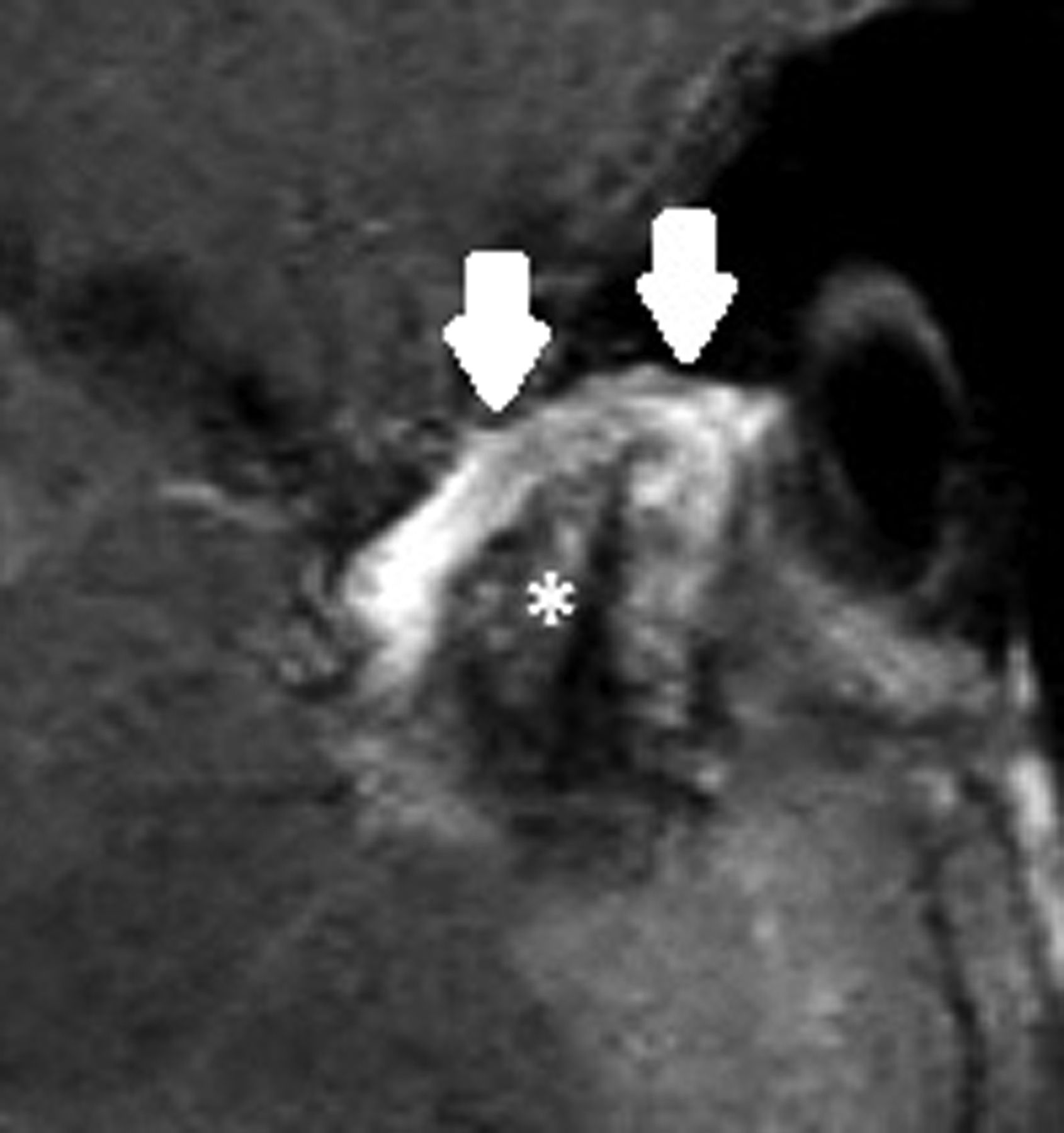
Sagittal postcontract image of active and chronic TMJ arthritis in a 13-year-old female with extended oligoarticular JIA. Condylar head erosions are evident (asterisk), as is a thickened and enhancing synovial lining (pannus, as depicted by arrows). The patient’s acute score for this joint (averaged from the 2 radiologists) was 3.5 out of a possible 7, while her chronic score was 13 out of 14. TMJ: temporomandibular joint; JIA: juvenile idiopathic arthritis.
Scoring of reads
Scoring of MRI was performed largely as previously described9, with 1 minor modification: altering the score range for joint effusions from 0–4 to 0–3. Two separate radiologists graded each TMJ separately for each of 3 findings indicative of acute arthritis and each of 5 indicative of chronic arthritis (Table 1). For each variable, 0 was the best possible score (no disease), and an increase in score over time represented worsening arthritis. The 2 scores were averaged to generate a single score. The 2 radiologists (SG, YV) were blinded to the other’s reads, but not to diagnosis or timing (pre- vs post-IA IFX). YV had 26 years of experience posttraining and helped design the scoring system used herein9. SG had 10 years of experience. Additionally, the Radiology Department at CoA interprets about 500 MRI of the TMJ annually.
TMJ MRI scoring system.
Statistical analyses
Proportional data are reported as percentiles and continuous data as median (range). Interrater characteristics of the scoring method were examined. Each pre- and post-IA IFX MRI of all subjects were reviewed by 2 radiologists (YV, SG) blinded to the other’s ratings. Acute and chronic scores for individual joints (132 in total) were compared between the 2 raters using the κ statistic. To account for nonidentical similar scores, a weighted κ statistic was performed13:

Scores for each of the MRI findings were averaged between the 2 radiologists for further analysis. Preinjection MRI findings, time between MRI, and MIO measurements were assessed for association with changes in acute or chronic scores following injection using univariate linear regression. Multivariable analysis was performed using significant (p ≤ 0.05) predictors identified in univariate regression.
RESULTS
Patients
Fifty-two children with JIA were eligible. Five were excluded because of the absence of followup MRI at the time of review, 1 subject was excluded for contrast allergy, and another was for motion artifact. Twelve additional subjects previously reported without new data were excluded8. Thus, 33 subjects were included who underwent 1–7 rounds of TMJ IA IFX over a 1-year period (Table 2). Decisions regarding the number of injections to perform were based upon a variety of factors, including the extent of symptoms of TMJ arthritis, postoperative MRI findings, patient/parent preference, recommendations from the treating rheumatologist, response to prior injections, and ability to obtain insurance approval. Thirty of the 33 patients (91%) had been exposed to systemic biologics with or without conventional disease-modifying antirheumatic drugs (DMARD) prior to the first IA IFX dose, while 2 others were treated with methotrexate (MTX) alone. During the period in which patients received IA IFX, systemic therapies were unchanged in 29/33 subjects; of the other 4, 1 switched from IFX to abatacept (ABA), another from ABA to IFX, 1 switched conventional DMARD from MTX to leflunomide, and 1 other discontinued MTX.
Study participants. Values are n (%) or median (range) unless otherwise specified.
Effectiveness
Changes in acute and chronic scores are shown in Figure 2. Overall, the median acute score increased by 0.25 points while the median chronic score increased by 0.75, indicating worsening of both acute and chronic findings over time. Overall, 17 subjects demonstrated worsening of acute findings compared with 3 on net unchanged and 13 improved. Corresponding numbers for chronic findings were 24 worsened, 4 unchanged, and 5 improved. In 10/66 TMJ, there were no chronic changes at baseline; of those, 7 were absent of chronic changes at followup. The remaining 3 TMJ had active arthritis in the interim. In 4 of the 66 TMJ, including both in 1 patient, the radiologists were in agreement that there were no acute changes at baseline; importantly, in 2 of those, including 1 of the 2 in the patient with 2 normal TMJ per the scoring system, the official report did indicate mild enhancement. This patient underwent a change in her systemic medication from IFX to ABA around the same time as when the IA IFX injections were performed, and at followup, had worsening acute and chronic changes bilaterally. Neither of the other 2 patients underwent changes in their systemic medications, and in both of them, the acute findings changed from 0 to 1 while the chronic findings were stable.

TMJ MRI scores before and after IA IFX therapy to the TMJ for 33 children with JIA. Changes in (A) acute and (B) chronic TMJ MRI score before and after IA IFX injections. The wider grey lines represent the regression lines. TMJ: temporomandibular joint; MRI: magnetic resonance imaging; IA: intraarticular; IFX: infliximab; JIA: juvenile idiopathic arthritis.
Agreement between the radiologists
Of the 132 TMJ examined, the 2 radiologists had agreement in 30% of acute scores and 25% of chronic scores (κ statistic 0.16 and 0.15, respectively). The weighted κ method accounted for degree of similarity between the 2 reviewers’ scores; using this method, the κ statistic increased to 0.49 for acute scores and 0.67 for chronic scores, both nearly identical to previously published results9.
Predictors of disease progression
MIO measurements were generally stable during this time frame, decreasing from 4.29 cm to 4.24 cm (means) among 32 subjects with paired data available. Univariate linear regression analysis demonstrated that the change in MIO was associated with worsening chronic but not acute score, with a 1-mm decrease in MIO associated with an increase (worsening) of MRI chronicity score of 1.1 (p = 0.052). Additional predictors of change in MRI chronicity score were worsening acute findings (on average: a 1-point increase in acute score predicted a 0.7-point increase in chronic score, p = 0.001) and time between MRI studies, with each additional month associated with a 0.4-point increase (worsening) in chronicity score (p < 0.001). When these factors were inputted into a multivariable model, worsening acuity score and duration of time between MRI examinations, but not change in MIO, retained significance.
None of the preinjection acute MRI findings (bone marrow edema, joint effusion, synovial enhancement, or acute total score) were univariate predictors of subsequent chronic changes on MRI. The preinjection chronic score was not associated with changes in acute score following IA IFX.
DISCUSSION
Thirty-three subjects received 1–7 rounds of bilateral IA IFX as therapy for TMJ arthritis refractory to aggressive systemic therapy and IA CS. Using a semiquantifiable and internally reliable TMJ MRI scoring system, our data show that overall IA IFX after IA CS does not appear to improve acute or chronic findings of advanced TMJ arthritis on subsequent MRI. Nevertheless, as previously reported8, some individual patients improved, sometimes substantially, following this therapy (Figure 2). We did not identify any predictors of treatment response. Likewise, the change in MIO in 22/32 subjects in whom paired measurements were available was at or below the threshold (4.9 mm) that was reported as the smallest detectable difference14, indicating minimal effect on this variable.
These data underscore challenges of treating inflammatory TMJ arthritis in JIA. Despite systemic TNFi in 30 of 33 subjects, acute changes worsened in 17/33 (52%) and chronic changes worsened in 24/33 (73%). This contrasts with response to systemic and local therapy among peripheral joints. However, these patients represent a distinct subgroup of children who already failed local therapy with IA CS, on top of aggressive systemic arthritis therapy. Thus, they may not represent patients with JIA in general. In light of potential risks of IA CS in the TMJ11, the risk-benefit profile of IA CS compared with IA IFX has yet to be elucidated. The mechanism by which IA delivery of a TNFi might offer an improved response when compared with systemic treatment is unclear. Conti, et al15 injected radiolabeled IFX into the knee of a patient with Behçet syndrome, demonstrating substantial uptake on the initial but not the second injection15; from this, they concluded that IA IFX can directly neutralize TNF present in the joint. Given the relatively small joint space as compared with the volume of distribution of 3–5 l in an adult for IFX, local delivery might be more effective than systemic delivery if local concentrations of TNF are high16. It is possible that higher doses of IA IFX would have been of benefit. Prior studies showing the effectiveness of IA IFX given at 100 mg per infusion in large joints16 showed more promising results than our current report, although no studies have directly evaluated this. Given the small volume of the TMJ, no more than 5–10 mg of IFX could be administered at a time. There could have been effects of dose within this range; however, precise volume administered was not documented. Additionally, a different TNFi that can be delivered in a higher effective concentration and/or with longer duration should be considered for future studies.
A strength of our study is the use of a semiquantifiable TMJ MRI scoring system. Agreement between the acute and chronic scores and between passage of time and changes in chronic score all support further use or refinement of the system. Our study also has limitations. Ours was a retrospective study, and the use of the 3T MRI in some subjects after August 2012 did not allow for blinding to pre- versus postinjection studies. In addition, use of the 3T scanner in some subjects post-IFX might have increased the sensitivity of the reads, although the majority were performed using the 1.5T scanner. Additionally, it bears emphasizing that the clinical significance of small changes in the scoring system is uncertain, although the results are largely in agreement with the prior published study8. Finally, there may be room for improvement in the scoring system itself, such as clarifying the extent to which enhancement in the TMJ can be considered normal and possibly incorporating additional sequelae of chronic TMJ arthritis (e.g., condylar hypoplasia, disc displacement).
The use of a semiquantitative MRI scoring system demonstrated that IA IFX in the TMJ in children with JIA did not improve acute or chronic TMJ arthritis changes for the overall cohort. However, any improvement, or no worsening, of acute or chronic changes on MRI observed in a substantial subset post-IA IFX is worthy of consideration in a cohort with refractory TMJ arthritis with a course of worsening disease/MRI findings despite aggressive systemic therapy and multiple rounds of IA CS. Future research should explore optimal treatment of refractory TMJ arthritis in JIA, including therapy comparison of IA TNFi with IA CS as first-line IA therapy, and identification of predictors of treatment response.
- Accepted for publication June 26, 2015.








{kind=link}
{kind=link}