Benefits of β blockers in patients with heart failure and reduced ejection fraction: network meta-analysis
BMJ 2013; 346 doi: https://doi.org/10.1136/bmj.f55 (Published 16 January 2013) Cite this as: BMJ 2013;346:f55
- Saurav Chatterjee, resident1,
- Giuseppe Biondi-Zoccai, assistant professor of cardiology2,
- Antonio Abbate, assistant professor of cardiology3,
- Fabrizio D’Ascenzo, fellow, interventional cardiology4,
- Davide Castagno, staff4,
- Benjamin Van Tassell, assistant professor3,
- Debabrata Mukherjee, chief of cardiology, and acting chairman of medicine5,
- Edgar Lichstein, chairman of medicine1
- 1Division of Internal Medicine, Maimonides Medical Center, New York, NY, USA
- 2Department of Medico-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Latina, Italy
- 3VCU Pauley Heart Center, Richmond, VA, USA
- 4Division of Cardiology, University of Turin, Turin, Italy
- 5Division of Cardiology, Texas Tech University, El Paso, TX, USA
- Correspondence to: S Chatterjee, 40 Roger Williams Green Apt 40 RWG, Providence, RI 02904, USA sauravchatterjeemd{at}gmail.com
- Accepted 28 December 2012
Abstract
Objective To clarify whether any particular β blocker is superior in patients with heart failure and reduced ejection fraction or whether the benefits of these agents are mainly due to a class effect.
Design Systematic review and network meta-analysis of efficacy of different β blockers in heart failure.
Data sources CINAHL(1982-2011), Cochrane Collaboration Central Register of Controlled Trials (-2011), Embase (1980-2011), Medline/PubMed (1966-2011), and Web of Science (1965-2011).
Study selection Randomized trials comparing β blockers with other β blockers or other treatments.
Data extraction The primary endpoint was all cause death at the longest available follow-up, assessed with odds ratios and Bayesian random effect 95% credible intervals, with independent extraction by observers.
Results 21 trials were included, focusing on atenolol, bisoprolol, bucindolol, carvedilol, metoprolol, and nebivolol. As expected, in the overall analysis, β blockers provided credible mortality benefits in comparison with placebo or standard treatment after a median of 12 months (odds ratio 0.69, 0.56 to 0.80). However, no obvious differences were found when comparing the different β blockers head to head for the risk of death, sudden cardiac death, death due to pump failure, or drug discontinuation. Accordingly, improvements in left ventricular ejection fraction were also similar irrespective of the individual study drug.
Conclusion The benefits of β blockers in patients with heart failure with reduced ejection fraction seem to be mainly due to a class effect, as no statistical evidence from current trials supports the superiority of any single agent over the others.
Introduction
According to the American Heart Association, heart failure affects nearly 8.26 million Americans and accounts for 32.8% of cardiovascular related deaths.1 β blockers have been one of the mainstays of treatment because of their ability to reverse the neurohumoral effects of the sympathetic nervous system, with ensuing prognostic and symptomatic benefits, and different societies have thus included them in guidelines for management of heart failure.2 3 4 Specifically, β adrenergic blockers have been shown in randomized trials to prolong survival, prevent arrhythmia, improve symptoms of heart failure and left ventricular ejection fraction, and control ventricular rate, especially in patients with chronic heart failure.5
However, controversy exists as to the optimal selection of a particular β blocker for management of heart failure, as the available β blockers differ in their selectivity for adrenergic receptors and their effects on the peripheral circulation.6 In addition, several of the available studies had a small sample size with a short duration of follow-up, thereby limiting their inferential capacity, and published meta-analyses have evaluated the role of β blockers in heart failure with reduced ejection fraction in terms of clinical and echocardiographic endpoints.7 8 9 Moreover, few studies have attempted to answer another crucial and debated question—that is, the tolerability of β blockers in heart failure. More importantly, the question of the superior efficacy of a given β blocker over others in preventing clinically relevant endpoints has never been assessed in the comprehensive setting of a systematic review, as only one trial has directly compared carvedilol and metoprolol tartrate.10
Network meta-analyses and mixed treatment comparisons exploit the totality of evidence stemming from randomized trials focusing on the same clinical topics and sharing, within the network frame, a common comparator. A network meta-analysis is thus the ideal design for head to head comparison of the different β blockers tested for heart failure. We therefore did a comprehensive systematic review and network meta-analysis to assess the efficacy of β blockers for heart failure with reduced ejection fraction with reference to participants (patients in heart failure), interventions (β blockers), comparisons (all pharmacologically active or inactive/placebo comparators), outcomes (specific clinical events), and study design (randomized trials).
Methods
This study was conducted according to the Cochrane Collaboration and PRISMA statements.11
Data sources and search
We searched for randomized trials in CINAHL (1982-2011), the Cochrane Collaboration Central Register of Controlled Trials (-2011), Embase (1980-2011), Medline/PubMed (1966-2011), and Web of Science (1965-2011). We restricted our searches to human studies, clinical trials, and controlled or randomized trials. We used the keywords and medical subject headings “adrenergic beta-antagonists,” “heart failure,” and “congestive,” as well as additional text words in combination with an established search strategy for Medline/PubMed.11 12 We also hand searched bibliographies of identified studies, recent meta-analyses of β blockers in heart failure, heart failure guidelines, and 2008-11 conference proceedings of the American College of Cardiology, American Heart Association, and European Society of Cardiology scientific sessions. We restricted our search to publications in the English language.
Study selection
Two independent reviewers (SC, GBZ) selected studies for inclusion, with divergences resolved by consensus. They first scanned citations at the title/abstract level and then retrieved shortlisted studies in full text. The reviewers considered these suitable for inclusion if they reported on randomized trials, compared β blockers versus another β blocker or comparator in patients with heart failure with reduced ejection fraction, and reported mortality. Studies were excluded if they were non-randomized, had less than 100 patients (to exclude small study effect), or had a follow-up of less than three months.
Data extraction and quality assessment
Two independent reviewers (SC, GBZ) abstracted data and appraised studies, with divergences resolved by consensus (κ statistic=0.9). They extracted key characteristics of studies and patients, including the following outcomes, reported at the longest available follow-up according to intention to treat principles: all cause mortality, cardiovascular death, sudden death, drug discontinuation, and change in left ventricular ejection fraction from baseline to follow-up. In addition, they appraised study validity according to the risk of bias tool recommended by the Cochrane Collaboration.
Data synthesis and analysis
We report categorical outcomes as numbers and continuous outcomes as median (interquartile range). We derived the raw event rates from individual studies and constructed 2×2 tables with raw number of events and total population of the trial. In trials that did not report raw event rates, investigators reported the percentage or proportion of patients having the event under consideration, which we rounded off to whole numbers by using the sample size of the population; we then calculated the risk difference by using the formula 1/(1+%OR), where OR=odds ratio. We calculated number needed to treat and corresponding absolute risk reduction from the 2×2 tables. We abstracted data in duplicate, and the inter-rater agreement was good (κ statistic=0.88). Considering different lengths of follow-up for individual trials, and to account for censored data, we obtained the rates of outcomes for all trials with follow-up longer than 12 months and calculated the log hazard ratios (assuming a constant rate of hazards for individual trials) from the event rates reported and mean duration of follow-up. We did standard pair-wise meta-analysis comparing β blockers with comparators, with 95% confidence intervals. We also used a random effect model (DerSimonian and Laird) to calculate prediction intervals for all cause mortality, using RevMan v5.1 and Stata version 11. We assessed and quantified heterogeneity with the help of the I2 statistic computed with the Cochran Q test.
We did network meta-analysis with random effect models by using WinBUGS 1.4.3 (MRC Biostatistics Unit, Cambridge, UK). Each analysis was based on vague priors for effect sizes (to yield results that are not too different from conventional statistical analysis). We checked and confirmed convergence and lack of autocorrelation after a 100 000 simulation burn-in phase; finally, we based direct probability statements on an additional 500 000 simulation phase to identify the best and most representative data, assuming comparable inter-study variances for all treatment effects for the same outcomes. We used deviance and the deviance information criterion to appraise model fit. We report results of network meta-analysis as odds ratios with 95% credible intervals for categorical outcomes and weighted mean differences with 95% credible intervals for continuous outcomes. We assessed extent of small study effects/publication bias by visual inspection of funnel plots and the Harbord’s regression modification of Eggers test, and we used a trim and fill method to estimate and adjust for any missing studies, and to calculate an adjusted odds ratio, as if the studies were present. We also calculated the absolute risk reduction and the number needed to treat to prevent one death.
We also attempted to evaluate if the different dosages of the individual β blockers used in a particular trial influenced the outcomes to a significant extent, as previous studies have been criticized for non-optimal dosing on various occasions.10 To assess for this, we identified the different target dosages of a particular drug used in trials, as well as the different mean achieved dosages, and then did a weighted meta-regression analysis using the least squares method, against the log odds ratios for the mortality outcomes to compute an adjusted odds ratio. As an additional sensitivity analysis, we did a network meta-analysis computing hazard ratios with a Poisson regression model and random effects method, as such analyses explicitly exploit differences in follow-up between studies, thus maximizing precision and validity. We used a random effects rather than a fixed effects model as this is probably the most appropriate and conservative analysis to account for variance within and between studies. For the purpose of analysis, given the variability in the length of follow-up for each of these trials, we used the rate of outcomes per 1000 person years to obtain the log hazard ratio of one β blocker relative to another, assuming a constant rate of hazard. We considered rates, rather than number of events, as the most appropriate outcome for these analyses because they incorporate the duration of the trials, which was variable. We calculated patient years of follow-up for each trial by multiplying the trial’s sample size by the mean duration of follow-up of the trial. We estimated hazard ratios from the median and the accompanying 95% credibility intervals from the 2.5th and 97.5th centiles of the posterior distribution, assuming a constant rate of hazard for the individual trials.
Results
After screening 720 citations (fig 1⇓), we included 21 studies,10 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 with a total of 23 122 patients, treated with atenolol, bisoprolol, bucindolol, carvedilol, metoprolol, nebivolol, or placebo/standard treatment. Patients had a median age of 61 years, 77% were male, ischemic heart failure was present in 57%, baseline left ventricular ejection fraction was 25%, and patients were followed for a median of 12 months. In addition to standard anti-heart failure treatment except β blockers, the control group received placebo in all but two trials (in which the control group received an angiotensin converting enzyme inhibitor but no β blocker) (fig 2⇓).16 21 One study compared carvedilol and metoprolol tartrate directly,10 although that has been criticized for under-dosing of metoprolol and for the use of a short acting formulation instead of an extended release form. Characteristics of studies are summarized in table 1⇓ and appendix table A. All trials had a low risk of bias according to Cochrane metrics (appendix table B).34

Fig 1 Review profile. RCT=randomized controlled trial

{kind=link}
{kind=link}
Key features of included studies
Overall pair-wise meta-analysis confirmed a significant reduction in mortality with use of β blockers versus all comparators (both active and placebo)—odds ratio 0.71, 95% credible interval 0.64 to 0.80; P<0.001 (fig 3⇓). Separate meta-analyses incorporating odds ratios from individual trials with shorter duration of follow-up (<12 months) (odds ratio 0.57, 0.46 to 0.70) and hazard ratios from trials with longer duration of follow-up (>12 months) (hazard ratio 0.70, 0.60 to 0.81) to account for the differential follow-up periods showed effect sizes consistent with the results of the overall primary pair-wise meta-analysis (appendix figures A and B). We further corroborated this with another separate network meta-analysis of hazard ratios using a random effects Poisson regression model (appendix table C).
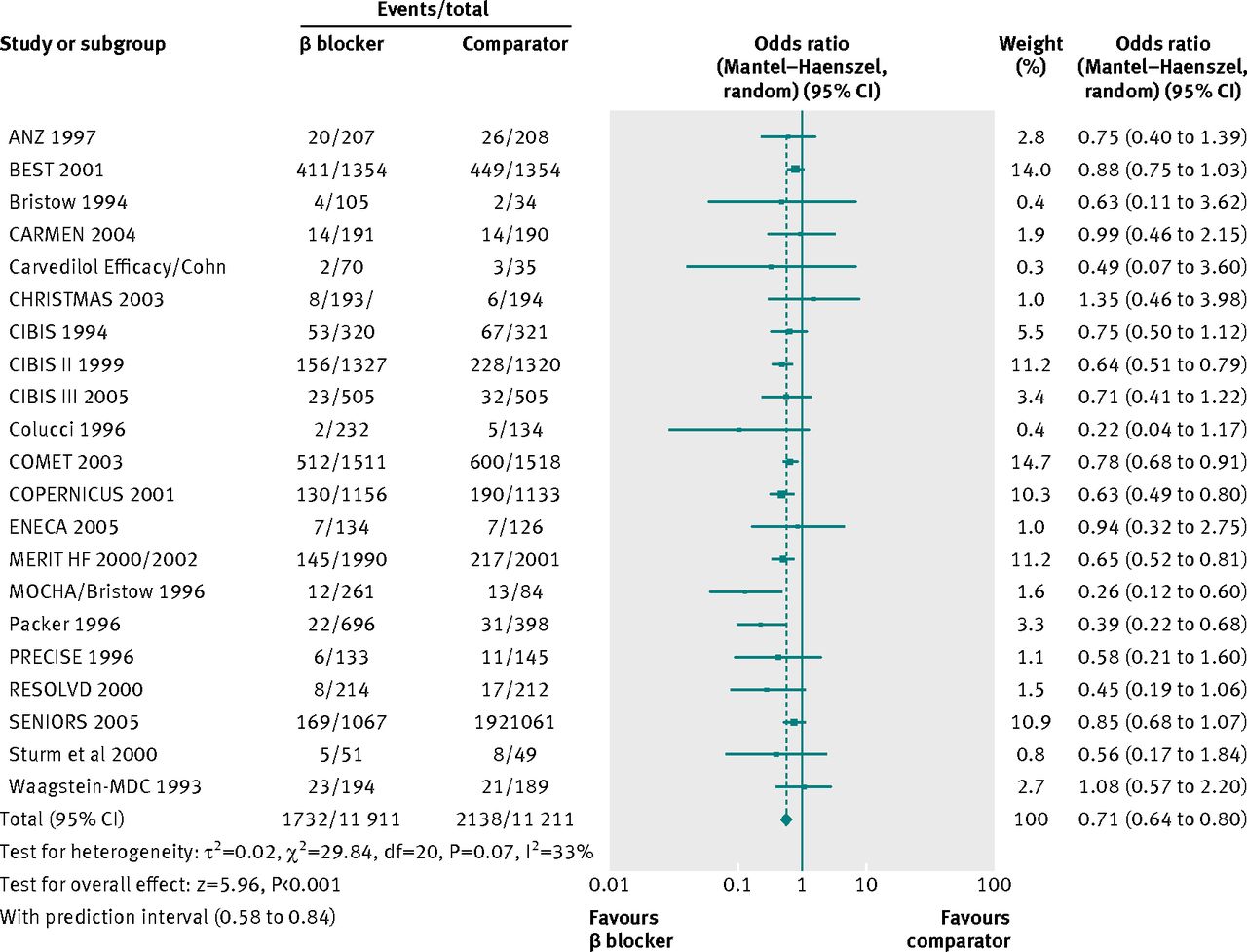
Fig 3 Standard pair-wise meta-analysis of β blockers and effect on mortality in chronic heart failure
{kind=link}
No publication bias was apparent on the funnel plot, or with the Harbord’s regression modification of Eggers test (two tailed P value of 0.13), and a trim and fill adjusted odds ratio was consistent with the primary analysis (0.76, 0.66 to 0.86) (fig 4⇓). We detected no significant heterogeneity for the appropriately weighted analysis of risk difference (P=0.25; I2=16%). Sensitivity analysis performed by exclusion of one study at a time showed consistent mortality benefit with use of β blockers in heart failure with reduced ejection fraction. Bayesian analyses confirmed, as expected, that β blockers were associated with a highly credible reduction in mortality compared with placebo/standard therapy (odds ratio 0.69, 0.56 to 0.80). β blockers also significantly reduced deaths from cardiovascular disease as well as sudden deaths, while increasing ejection fraction by a mean of 4.1% and having a tolerability profile similar to the comparators (we postulated that drug discontinuation rates might be a surrogate endpoint reflecting tolerability of the individual β blockers) (table 2⇓). Similarity in the directions of the effect size estimates and the overlap of the 95% confidence intervals of both the standard pair-wise frequentist and the Bayesian network meta-analyses corroborated our assumptions of consistency.

Fig 4 Trim and fill adjusted odds ratio (calculated by imputing effect of possible missing studies)—shown to be less than 1, indicating robust and conclusive evidence in favor of mortality benefit with β blocker use in heart failure
{kind=link}
Head to head comparisons between different β blockers (reported as point estimates of odds ratios or weighted mean differences with 95% credible intervals, with number of studies contributing to network)
All β blockers showed improvements in mortality; the numerically largest effect was seen with carvedilol (lowest odds ratio). However, when we made a comparison between the individual β blockers, the mortality advantage conferred by each was not statistically different from another. Carvedilol also had the best numerical advantage in tolerability (lowest pooled discontinuation rates), while not being statistically superior to other β blockers. Bucindolol improved the ejection fraction to the greatest extent in our analysis, but it was not significantly superior to the other drugs in its class. Exclusion of trials with pharmacologically active comparators did not alter our findings to a significant effect.10 16 21 We also determined the absolute risk reductions and the numbers needed to treat to prevent one death for each of the β blockers assessed (appendix table D). Congruent with our primary analysis, the absolute risk reduction for mortality was greatest with carvedilol—6.6% reduction, with a number needed to treat of 15 to prevent one death. Our analysis also showed that different target dosages of individual β blockers used in the randomized trials, as well as the mean doses achieved, did not influence the logarithm of the odds ratio of mortality, as determined by weighted meta-regression analysis. An exploratory sub-analysis of trials conducted in the United States only showed significant reduction in mortality with β blocker use in the US (odds ratio 0.48, 0.29 to 0.82) (appendix figure C). The consistency and directionality of the effect persisted even when we relaxed our inclusion criteria to include smaller studies of sample size 50 or above (appendix figure D).
Discussion
β blockers, as a class, provided credible mortality benefits in comparison with placebo or standard treatment in patients with heart failure, and the beneficial effects on mortality persisted irrespective of the duration of treatment. However, we found no obvious differences when comparing the different β blockers head to head for the risk of death, sudden cardiac death, death due to pump failure, or drug discontinuation by way of a network meta-analysis or mixed treatment comparison. Accordingly, improvements in left ventricular ejection fraction were also similar irrespective of the individual study drug.
β blockers have long been shown to have unequivocal mortality benefits in chronic heart failure, especially with long term follow-up, although this is slightly controversial as most of the landmark randomized controlled trials of β blockers have been stopped prematurely.35 Several large trials and meta-analyses have assessed the mortality benefit of β blockers in chronic heart failure with reduced ejection fraction and have shown a mortality benefit of β blocker use in chronic heart failure as well as in ischemic and non-ischemic cardiomyopathy.36 Various studies have looked at important reduction in clinically relevant endpoints such as sudden death, pump failure, and hospital readmission rates with β blockers in heart failure.37 38 39 Retrospective analyses have compared different β blockers and their effect on clinical endpoints in chronic heart failure, and no superiority was found for one individual class over another in reducing mortality or readmissions.40 41 When the surrogate endpoint of improvement in ejection fraction has been investigated, superiority of any one class of β blockers could not be definitely established.42 With this robust evidence in favor of β blockers in chronic heart failure, we decided to assess the efficacy of one β blocker over another by comparing them using a Bayesian network meta-analysis, in view of paucity of head to head trial data, except for the COMET study.10
Also, to our knowledge, the question of tolerability and premature discontinuation of β blockers in chronic heart failure has not been investigated, except in isolated trials, so we decided to pool the data from different trials to assess the important question of tolerability and the discontinuation rates of different β blockers in heart failure with reduced ejection fraction.43 Our analysis reassuringly shows that overall, the tolerability, as indicated by discontinuation rates in different randomized trials, of β blockers as a class of drugs is generally good and comparable to a range of pharmacologically active and inactive comparators.
Our analysis shows that among the different β blockers in current use, bisoprolol, carvedilol, and metoprolol all had significant mortality benefit compared with placebo/standard heart failure treatment. However, our data additionally indicate that carvedilol was not only superior to placebo/standard heart failure treatment for all cause mortality but also had the lowest cardiac mortality numerically among all β blockers tested, although this was not statistically significant, indicating a benefit for its use in patients with cardiovascular comorbidities as an empiric initial treatment of choice. This finding was congruent in our analysis with the results and subgroup analyses from COMET,10 44 possibly as a result of a beneficial effect of carvedilol on endothelial function, its stimulatory effects on β arresting signaling, and its anti-oxidant properties.45 46 47 Carvedilol has also been found to be superior to metoprolol in maintaining a favorable glycemic profile in patients with diabetes, improved insulin sensitivity, and decreased progression to microalbuminuria, all of which have been shown to have cardioprotective effects.48 Considering the lack of differences in improvement of mortality with use of individual β blockers in chronic heart failure, as shown in our data, we consider it pragmatic to infer that, although the data may be limited, we have three agents (bisoprolol, sustained release metoprolol succinate, and carvedilol) that have been tested more extensively and have been shown to be superior to placebo in our analysis (95% credible interval did not include 1). Hence, one of these three agents should be chosen as the empiric drug of choice in treatment of chronic heart failure with reduced ejection fraction.
Our analysis indicates that the cost of individual β blocker treatment for patients can possibly be reduced by choosing the least expensive agent. Another significant finding was that tolerability, as measured by premature discontinuation rates in trials, was also numerically the best with carvedilol (although again the difference did not reach statistical significance), making a case for its increased use among sicker patients needing a β blocker. This could be a crucial point in patients taking many different drugs, as non-adherence to treatment is the most frequent reason for hospital admission for acute heart failure, with important implications for clinical management and potentially for prognosis.49 In harmony with the current American College of Cardiology/American Heart Association recommendations, and a previous Bayesian analysis,50 51 our analysis shows mortality benefit with use of β blockers in chronic heart failure—especially for bisoprolol, carvedilol, and sustained release metoprolol succinate—and their use should be recommended for all stable patients with current or previous symptoms of heart failure and reduced left ventricular ejection fraction, unless contraindicated.
Limitations of study
Our analysis was limited by the data in the included studies and the structure of the reported data. Meta-analysis of rare events is known to produce erroneous results. This is further compounded in network meta-analysis if few trials per comparison are available, as was the case with a few of the β blockers. Therefore, extra caution should be exercised when interpreting the treatment rankings for the primary outcome (mortality). Furthermore, outcomes were not consistently reported across the ensemble of trials. An individual participant meta-analysis might overcome this limitation, even if this might reduce the sample size. Although we feel reasonably confident of our search strategy, some trials, such as potentially some non-English language trials, may not have been included. The results may also be limited by the modeling assumptions. Because of the multitude of doses used for many trials, we did a weighted meta-regression analysis by target and achieved doses of individual drugs and their effects on the natural log of the calculated odds ratio, which did not alter the outcomes.
Another potential limitation of our study stems from the interesting analysis in a recent paper,52 which suggested that β blockade was associated with a lower magnitude of survival benefit in the United States than was seen in the rest of the world. Non-availability of patient level data prevents us from commenting definitively on the effect of geographic distribution on the outcomes seen with β blockers; however, our preliminary analysis using trial level data does refute the phenomenon. In the absence of patient level data, an adequately rigorous analysis to assess the effect of geographic location with use of β blockers is extremely difficult to do, and future efforts should focus on explaining or refuting this interesting phenomenon.
Comparison with other studies
A previous retrospective study attempted to compare different β blockers in clinical use by using data from an administrative database.53 The authors concluded that atenolol and acebutolol were superior to metoprolol in reducing mortality in patients, whereas carvedilol and bisoprolol were not superior to metoprolol in improving survival. The population studied in that analysis was quite different from the population of randomized trials assessed in our study—the mean age of the population of that study was 77 years, whereas the mean age of the population in our analysis was 61 years, and the percentage of male patients was 49% in the study, whereas male patients comprised 76% of the population in our analysis. Also, ejection fraction was not accounted for in the analysis of the retrospective study, whereas the mean ejection fraction of the population in our analysis was 26%. Hence, the difference from our study, which pooled data from randomized trials only, can likely be explained by differences in the population studied and differences in the analytic methods.
Conclusions
Our analysis, using one of the largest sample sizes of β blockers in chronic heart failure with reduced ejection fraction and a novel analytic method of comparing individual β blockers by using Bayesian network meta-analysis, suggests that β blockers are safe and tolerable for patients with chronic heart failure and that the mortality benefit and other clinically relevant effects, as well as the improvement in ejection fraction, are a class effect of β blockers and superiority of one over another cannot be determined with the currently available data. More head to head comparisons of individual β blockers are needed to definitively answer the question of whether one agent is clearly superior.
What is already known on this topic
β blockers are useful in preventing deaths in patients with heart failure
Carvedilol, bucindolol, and metoprolol succinate are the only β blockers shown in randomized trials to be of benefit in lowering mortality in patients with heart failure
A previous study has contended that β blockers may not be as effective in preventing mortality in the US as in rest of the world
What this study adds
This study, using novel methods in the framework of a Bayesian analysis, computes the relative mortality benefit of β blockers in patients with heart failure as 20-35%
The mortality benefits observed with the individual β blockers seems to be largely due to a “class effect,” with no evidence of a clearly superior agent among individual β blockers
The extent of reduction in mortality seen in trials conducted solely in the US was comparable to that seen in trials conducted in the rest of the world
Notes
Cite this as: BMJ 2013;346:f55
Footnotes
Contributors: SC and GB-Z contributed equally to this work and were responsible for the study concept and design. SC, FD’A, and GB-Z acquired, analyzed, and interpreted the data. SC, AA, FD’A, DC, BVT, DM, and EL drafted the manuscript. AA, BVT, DM, and EL critically revised the manuscript for important intellectual content. SC and GB-Z did the statistical analysis. EL, GB-Z, and DM provided administrative, technical, and material support. EL, DM, and GB-Z provided study supervision. SC and GB-Z are the guarantors.
Funding: None.
Competing interests: All authors have completed the Unified Competing Interest form at http://www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Ethical approval: Not needed.
Data sharing: Technical appendix, statistical code, and dataset are available from the corresponding author at sauravchatterjeemd{at}gmail.com.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.