Article Text

Abstract
Objectives Assess golimumab's long-term efficacy/safety in psoriatic arthritis (PsA).
Methods Adults with active PsA (≥3 swollen and tender joints, active psoriasis) were randomly assigned to subcutaneous placebo, golimumab 50 mg, or golimumab 100 mg every 4 weeks (q4wks) through wk20. All patients received golimumab 50 mg or 100 mg q4wks from wk24 forward. Methotrexate was allowed and taken by approximately half the patients. Findings through 5 years are reported herein. Efficacy assessments included ≥20% improvement in American College of Rheumatology (ACR20) response, C-reactive-protein-based, 28-joint-count Disease Activity Score (DAS28-CRP) response, ≥75% improvement in Psoriasis Area and Severity Index (PASI75) scores, and PsA-modified Sharp/van der Heijde scores (SHSs).
Results 126/405 (31%) randomised patients discontinued treatment through wk252. Golimumab was effective in maintaining clinical improvement through year-5 (ACR20: 62.8–69.9%, DAS28-CRP: 75.2-84.9% for randomised patients; PASI75: 60.8–72.2% among randomised patients with ≥3% body surface area involvement) and inhibiting radiographic progression (mean changes in PsA-modified SHS: 0.1–0.3) among patients with radiographic data. While concomitant methotrexate did not affect ACR20/PASI75, it appeared to reduce radiographic progression. No new safety signals were identified. Antibodies-to-golimumab occurred in 1.8%/10.0% of patients with/without methotrexate).
Conclusions Long-term golimumab safety/efficacy in PsA was demonstrated through 5 years.
Trial registration number NCT00265096.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Biologic anti-tumour necrosis factor-α (TNF) agents have demonstrated efficacy in psoriatic arthritis (PsA), in treating arthritic/dermatologic symptoms and inhibiting structural damage progression.1–5 The human anti-TNF monoclonal antibody golimumab (50/100 mg subcutaneously every 4 weeks (q4wks)) was evaluated in the GO-REVEAL Phase 3, randomised, double-blind, placebo-controlled trial in 405 patients with active PsA (NCT00265096). Study results through wk24 (placebo-controlled), wk52, and wk104 have been published.6–8 We now provide a final report of efficacy and safety data in PsA patients receiving golimumab through 5 years.
Patients and methods
Details of patient eligibility criteria, study design, and study endpoints have been reported.6–8 Briefly, patients were naive to anti-TNF therapy, had active PsA (≥3 swollen, ≥3 tender joints), and had plaque psoriasis (qualifying lesion diameter ≥2 cm) despite therapy with disease-modifying antirheumatic or non-steroidal anti-inflammatory drugs. Concomitant methotrexate was allowed but not required. Study design and analytical details specific to the GO-REVEAL long-term extension (LTE) are provided online.
Results
Patient disposition and baseline characteristics
Four hundred and five patients were randomised and treated. Consent was obtained for the first patient on 12 December 2005; the last patient completed wk268 (16 weeks after last study injection) on 13 January 2012. Patient disposition through wk24,6 wk527 and wk1048 have been reported. Among the 405 randomised patients, 126 (31%) discontinued study treatment through wk252 (see online supplementary table S1). Radiographic images/scores were available for 304 patients at baseline and wk104 and for 267 patients at wk256. For details of baseline patient and disease characteristics and concomitant medications, see online tables S1, S2, S3, and supplemental material.
Efficacy results
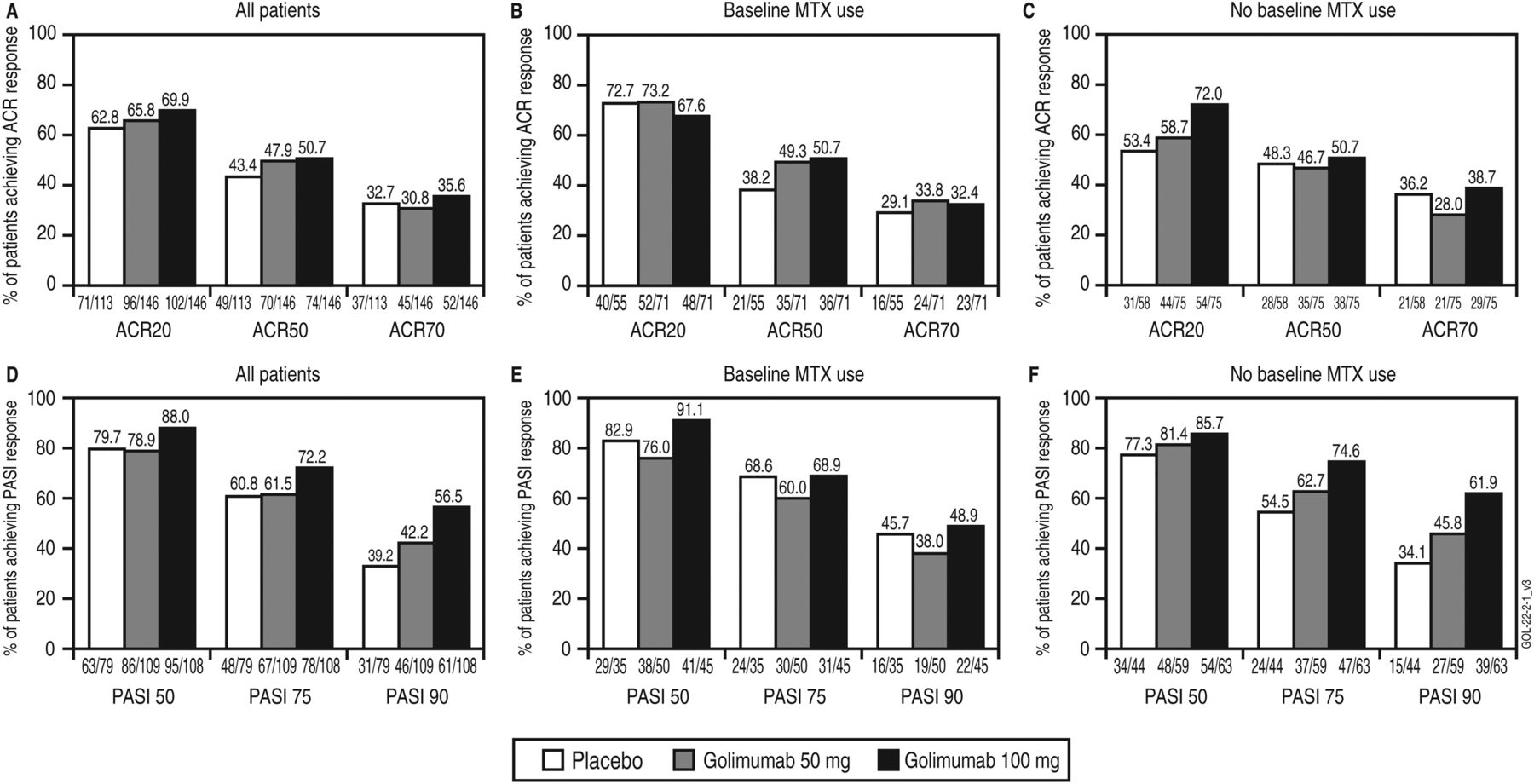
Among randomised patients, wk256 response rates were 62.8–69.9%, 43.4–50.7% and 30.8–35.6% for American College of Rheumatology ≥20%/50%/70% improvement criteria (American College of Rheumatology, ACR20, ACR50 and ACR70, respectively; figure 1A). No consistent differences in ACR response by baseline methotrexate use were observed (figures 1B,C). Mean C-reactive-protein-based, 28-joint-count Disease Activity Scores (DAS28-CRP) at wk256 were 2.8–3.0 versus baseline scores of 4.9–5.0 (table 1). DAS28-CRP responses and improvements in dactylitis and enthesitis scores are also summarised in table 1.
Summary of efficacy and concomitant medication use at week 256 by randomised treatment group
{kind=link}
The proportions of patients achieving clinical improvement at week 256, defined by at least 20%, 50% and/or 70% improvement in the American College of Rheumatology response criteria (ACR20, ACR50 and ACR70, respectively; A–C) or at least 50%, 75% and/or 90% improvement in the Psoriasis Area and Severity Index response criteria (PASI50, PASI75 and PASI90, respectively) among randomised patients with baseline psoriasis involving ≥3% body surface area (D–F) among all patients (A, D) patients with methotrexate (MTX) use at baseline (B, E), and patients with no MTX use at baseline (C, F). Analyses were based on intent-to-treat analyses by randomised group, irrespective of treatment changes during the study. The placebo group includes patients who were initially randomised to placebo and later early escaped/crossed over at week 16/24 to receive golimumab 50 mg, with the possibility to increase golimumab from 50 to 100 mg after the week-52 database lock. The golimumab 50 mg group includes patients who were initially randomised to golimumab 50 mg and later early escaped at week 16 or dose escalated after the week 52 database lock to receive golimumab 100 mg. All patients could decrease the golimumab dose from 100 to 50 mg after the week-52 database lock.
At least 75% improvement in the Psoriasis Area and Severity Index (PASI75) (figure 1D) was achieved at wk256 in 60.8–72.2% of randomised patients with baseline psoriasis involving ≥3% body surface area. No consistent differences in PASI responses by baseline methotrexate use were observed (figures 1E,F). Improvements in nail psoriasis severity were also evident (table 1).
Clinically meaningful improvements in physical function (Health Assessment Questionnaire Disability Index (HAQ-DI) decrease ≥0.3)9 were observed at wk256 for 52–58% of randomised patients. Mean wk256 HAQ-DI scores were 0.6–0.7 versus baseline scores of 1.0–1.1. Patients also experienced improvement in health-related quality of life (table 1).
The two radiographic readers demonstrated good agreement in radiographic image scoring (see online supplementary material). At wk256, observed changes (mean±SD) from baseline in PsA-modified radiographic scores were 0.3±3.8, 0.3±4.2, and 0.1±2.7 in the placebo, 50 mg and 100 mg groups, respectively (table 1, see online supplementary figure S1A). Patients receiving methotrexate at baseline demonstrated numerically less progression at wk256 than patients not receiving methotrexate based on mean changes in Sharp/van der Heijde score (SHS) (table 1, see online supplementary figures S1B,C). Estimated annual radiographic progression, calculated as baseline total score divided by baseline PsA duration, was markedly reduced over 5 years (see online supplementary figure S2).
The effect of golimumab dose escalation from 50 mg q4wks to 100 mg q4wks was evaluated for patients who had not achieved DAS28-CRP <2.6 or PASI75 response before dose escalation. Increasing the golimumab dose yielded approximately 18% and 44% improvement in DAS28-CRP and PASI scores, respectively (table 1).
For details of golimumab pharmacokinetic and antibody assessments, please see online supplementary materials. Antibodies-to-golimumab developed in 6% (20/335), including 1.8% (3/165) and 10.0% (17/170), respectively, of patients receiving and not receiving methotrexate at baseline.
Safety results
Per protocol, no patient received placebo beyond wk24. In general, no differences in the types of adverse events (AE) were observed between golimumab doses (table 2). See online supplementary material for summaries of AEs reported after initiation of commercial drug, injection-site reactions, and clinical laboratory findings.
Summary of safety through week 268
AEs leading to discontinuation observed in >1 golimumab-treated patient overall included basal cell carcinoma (basal cell carcinoma (BCC), 3–50 mg, 2–50+100 mg, 3–100 mg patients), increased alanine aminotransferase (5–50 mg, 1–50+100 mg), increased aspartate aminotransferase (3–50 mg, 1–50+100 mg), psoriatic arthropathy (1–50 mg, 2–50+100 mg), breast cancer (2–50 mg), and accidental death (1–50 mg, 1–100 mg).
Five patients died through wk268 (50 mg-climbing accident, 50 mg-small-cell lung cancer, 100 mg motor bike accident, 100 mg oesophageal cancer, 100 mg unknown cause).
Serious AEs observed in >1 golimumab-treated patient included 10 patients with BCC; five patients with myocardial infarction; three patients with cholelithiasis; and two patients each with breast cancer, abscess, cellulitis, pneumonia, arthritis, intervertebral disc degeneration, upper abdominal pain, vomiting, tibia fracture, accidental death, chest pain and superficial thrombophlebitis. Fifteen patients developed serious infections through wk268, with similar incidences across treatment groups. Few patients developed opportunistic infections, including one patient each with pulmonary tuberculosis plus legionella pneumonia, histoplasmosis and eye toxoplasmosis, all while receiving golimumab 100 mg. A patient receiving golimumab 100 mg developed non-serious herpes zoster involving the eye.
The incidence of major adverse cardiovascular events (MACE) through wk268 was similar across all treatment groups (table 2). Beyond MACE events, two golimumab patients (1–50 mg+100 mg, 1–100 mg only) had congestive heart/ventricular failure through wk268.
Malignancies were documented for 21 patients through wk268, including 10 patients with non-melanoma skin cancer (NMSC, 1 squamous cell+basal cell, 9 basal cell) and 11 with other non-lymphoma malignancies that included breast (2–50 mg), bladder (1–50+100 mg, 1–100 mg), colon (2–50 mg, 1–100 mg), oesophageal (1–100 mg), prostate (1–100 mg), and small-cell lung (1–50 mg, 1–100 mg) cancers. The incidences of malignancies per 100 patient-years are presented in table 2. In an analysis comparing incidences of malignancies (excluding NMSC) observed in GO-REVEAL and expected rates in the general US population,10 the standard incidence ratios ranged from 0.57 to 1.85 (table 2).
Discussion
We previously reported golimumab (subcutaneous 50 and 100 mg q4wks) efficacy/safety in patients with active PsA. Golimumab-treated patients displayed significant and/or clinically meaningful improvements in all aspects of PsA versus placebo.6 ,7 Despite no control arm, findings through wk104 of the LTE also supported golimumab's clinical and radiographic benefits.8 The current report extends the golimumab experience by 3 years, representing the longest available clinical trial data of chronic anti-TNF treatment of PsA patients.
The GO-REVEAL trial retained more than two-thirds of randomised patients through 5 years, and although lacking a control after wk24, data through 5 years provide further insight into golimumab efficacy and safety. At the last efficacy evaluation (wk256; assessed with intent-to-treat (ITT) methodology), 63–70% and 43–51% of patients across randomised groups were ACR20 and ACR50 responders, respectively, and mean baseline DAS28-CRP scores decreased from 4.9–5.0 to <3.2 across treatment groups. Meaningful improvements were also noted in physical function, enthesitis, dactylitis, and skin manifestations, including >60% of patients achieving PASI75 improvement at wk256. Importantly, minimal changes in radiographic scores occurred from baseline to wk256 (mean change in total SHS ≤0.3), suggesting a long-term effect of golimumab on inhibiting radiographic progression.
No meaningful differences in efficacy outcomes were observed between the 50 mg and 100 mg doses of golimumab administered q4wks; however, analyses were limited by allowed dose changes. Similarly, analyses of clinical response in arthritis and psoriasis after dose escalation from 50 to 100 mg q4wks suggesting improved efficacy, especially in PASI scores, were limited by lack of a control arm. Golimumab dose escalation occurred in approximately one-quarter of randomised patients and, given low discontinuation rates due to lack of golimumab efficacy, likely reflects a treat-to-target therapeutic approach in patients with residual disease activity.
Golimumab safety through 5 years was also consistent with those observed previously in this PsA patient population.6–8 Serious infections occurred in 15 patients; a limited number of patients had opportunistic infections, all while receiving golimumab 100 mg. The incidence of antibodies to golimumab was low across the golimumab treatment groups and did not appear to affect injection-site-reaction development. Consistent with earlier observations,6–8 fewer methotrexate-treated than untreated patients developed antibodies to golimumab. The incidences of all malignancies excluding NMSC observed in GO-REVEAL did not differ from those expected in the general US population. No meaningful differences in safety outcomes were observed between patients receiving golimumab 50 mg, 100 mg, or both doses, except opportunistic infections (all reported for golimumab 100 mg).
Limitations of long-term data presented herein include the lack of a long-term control arm and golimumab dose changes, restricting the ability to compare golimumab 50 mg with 100 mg. To compensate for such limitations, clinical efficacy data were evaluated on an ITT basis (randomised patients with imputation for missing data). However, to avoid imputation of radiographic data, radiographic analyses were based on patients who had available images at baseline/wk104/wk256, comprising ∼66% of randomised patients. Although radiographic analyses including patients with available data are possibly biased by including responders only, the alternative analyses employing all patients and imputation methodologies rely on assumptions made for patients with missing data, also possibly leading to biased estimates of radiographic progression. Baseline disease characteristics were similar between the radiographic patient subset and all randomised patients, indicating findings may be applicable to the overall study population.
Despite discussed limitations, the safety and efficacy of golimumab 50 mg and 100 mg administered subcutaneously q4wks to patients with active PsA were demonstrated through 5 years, as evidenced by sustained clinical and radiographic efficacy and a safety profile consistent with other anti-TNF agents used for PsA.11
Acknowledgments
The authors thank Michelle Perate, MS and Mary Whitman, PhD (Janssen Scientific Affairs, LLC) for writing and editorial support. A complete list of study investigators was previously reported.10
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online CONCISE
Footnotes
-
Handling editor Tore K Kvien
-
Correction notice This article has been corrected since it was published Online First. A minor change has been made to the title.
-
Contributors DG participated in the trial design and conduct and manuscript preparation. AK participated in the trial design and conduct and manuscript preparation. GGK participated in the trial design and conduct and manuscript preparation. PM participated in the trial design and conduct and manuscript preparation. IM participated in the trial design and conduct and manuscript preparation. DvdH participated in the trial design and manuscript preparation. YZ, JL, JHL all contributed to data analysis and interpretation and manuscript preparation, and NG and AB contributed to study design/ conduct, data interpretation, and manuscript preparation.
-
Funding The study was supported by Janssen Research & Development, LLC, Spring House, PA and Merck/Schering-Plough Corporation, Kenilworth, NJ.
-
Competing interests DG has received grant support, consultation fees and/or honoraria from Abbott, Amgen, Bristol-Myers Squibb, Genentech, Janssen, Merck/Schering-Plough and Wyeth. AK has received funding for clinical research sponsored by Abbott, Amgen, Janssen, and UCB. GGK has received fees as a consultant and/or advisory board member for Abbott, Almirall, Alza, Amgen, Anacor, Astellas, Barrier Therapeutics, Boehringer Ingleheim, Bristol-Myers Squibb, CombinatoRx, Exelixis, Genentech, Genzyme, Isis, Janssen, L'Oreal, Lupin Limited, Magen Biosciences, MedaCorp, Medicis, Merck/Schering-Plough, Novartis, Novo-Nordisk, Somagenics, theDerm.org, Synvista, Warner Chilcot, UCB, USANA Health Sciences and ZARS. GGK has received lecture fees from Abbott, Amgen, Astellas, Boehringer Ingleheim, Connetics, Janssen, National Psoriasis Foundation, The Foundation for Better Health Care and Warner Chilcot. PM has received research grant support, consultation fees, and speaker honoraria from Abbott, Amgen, Biogen-IDEC, Bristol-Myers Squibb, Genentech, Janssen, Pfizer, and UCB, and grant support and consultation fees from Celgene and Novartis. IM has received grant funding and honoraria from Abbott, Janssen, Roche, Merck/Schering-Plough, and Wyeth. DvdH has received consulting fees and/or research grants from AbbVie, Amgen, AstraZeneca, Augurex, BMS, Celgene, Chugai, Covagen, Daiichi, Eli-Lilly, GSK, Janssen Biologics, Merck, Novartis, Novo-Nordisk, Otsuka, Pfizer, Roche, Sanofi-Aventis, Schering-Plough, UCB, Vertex. YZ, JL, JHL, NG and AB are employees of Janssen Research & Development, LLC.
-
Ethics approval The study was conducted according to the Declaration of Helsinki and International Committee on Harmonisation good clinical practices. The protocol was reviewed and approved by each site's governing institutional review board or ethics committee, reflecting national requirements for study conduct approval. All patients provided written informed consent.
-
Provenance and peer review Not commissioned; externally peer reviewed.