Article Text

Abstract
Objective The aim of this pilot study was to assess peripheral blood perfusion (PBP) by a new technique, the laser speckle contrast analysis (LASCA), in systemic sclerosis (SSc) patients showing different patterns of nailfold microangiopathy. Correlations between LASCA and single laser Doppler flowmetry (LDF) analysis were also checked.
Methods Sixty-one SSc patients and 61 healthy subjects were enrolled. PBP was evaluated using LASCA and LDF. Scleroderma patterns and microangiopathy evolution score (MES) were assessed by nailfold videocapillaroscopy (NVC).
Results As detected by LASCA and LDF, PBP was lower in SSc patients than in healthy subjects (p<0.0001), showing SSc patients with the ‘Early’, ‘Active’ or ‘Late’ NVC pattern a progressively lower PBP (p=0.04 and p=0.002, respectively). There was a negative correlation between PBP and MES values (p=0.006 and p=0.002 for LASCA and LDF, respectively). A positive correlation was detected between LASCA and LDF values, in all subjects (p<0.0001). However, LASCA evaluates larger skin areas, is significantly less time consuming, is more accepted by patients and shows lower intra-operator variability than LDF.
Conclusions LASCA detected lower PBP in SSc patients than in healthy subjects, and for the first time, LASCA perfusion values were found correlated with progression of NVC patterns of microangiopathy.
- Systemic Sclerosis
- Autoimmune Diseases
- Qualitative Research
Statistics from Altmetric.com
Introduction
The microvascular alteration in systemic sclerosis (SSc) may be assessed by nailfold videocapillaroscopy (NVC), single laser Doppler flowmetry (LDF), or more recently by laser speckle contrast analysis (LASCA).1–3
NVC can easily detect peripheral microvascular morphology, as well as classify and score the capillary abnormalities into different patterns of microangiopathy.4–7 LDF is a common technique for assessment and quantification of blood perfusion at peripheral sites.2 ,8 LASCA is an innovative method able to assess and quantify the whole blood perfusion at different skin areas.9–11
The major aim of this study was to evaluate the efficacy of LASCA in the assessment of peripheral blood perfusion (PBP) in SSc patients with different patterns of nailfold microangiopathy and to correlate results with LDF analysis.12 ,13
Methods
Sixty-one consecutive SSc patients (mean age 63±11SD years, 54 women and 7 men, mean Raynaud's phenomenon duration 12±11 years, mean SSc duration 6±5 years) and 61 sex-matched and age-matched healthy subjects were enrolled after having obtained written informed consent. SSc patients met either the American College of Rheumatology criteria for SSc, or the Le Roy's criteria for the classification of early SSc.14
Assessments were performed during the treatment-free period (at least 1 month) from prostanoids, endothelin-1 receptor antagonists, ACE-inhibitors, calcium channel blockers. All SSc patients were on aspirin, and patients on drugs that could potentially and directly influence PBP were excluded. Complete medical history and clinical examination were collected. Patients stayed in a waiting room (at 22–23 °C) for at least 30 min before all the assessments.
Laser speckle contrast analysis
PBP was analysed by LASCA (Pericam PSI, Perimed, Jarfalla), in both SSc patients and healthy subjects. The principle of the LASCA technique and study methodology are reported in online supplementary table S1.11 The PBP was registered at the level of the whole volar region of the hands for 30 s each one, and the values were recorded as perfusion units (PU) (figure 1). Subsequently, regions of interest (ROIs) were created at 2nd, 3rd, 4th and 5th fingertips bilaterally, and the average PU calculated.

Laser speckle contrast analysis image of right hands and related nailfold videocapillaroscopy (NVC) pictures in a healthy subject (A), and in SSc patients with a ‘Early’ (B), ‘Active’ (C) or ‘Late’ (D) pattern of microangiopathy (NVC picture magnification 200×).
Laser Doppler flowmetry
LDF was performed in SSc patients and healthy subjects by using the Periflux System 5000 (Perimed, Milan, Italy) at the level of 2nd, 3rd, 4th and 5th fingertips bilaterally (on the volar aspect of the finger pad).2 See online supplementary table S2 for LDF methodology. The average blood perfusion from the II to V fingers bilaterally was calculated by summing the perfusion values of the eight fingers together and then dividing the final value by the number of fingers. The results were expressed as PUs.
Nailfold videocapillaroscopy
NVC was performed in each patient to assess any morphological microvascular damage using a videocapillaroscopy optical probe, equipped with a 200× contact lens, connected to image analysis software (Videocap, DS Medica, Milan, Italy). The same operator performed the NVC examination in all SSc patients the same day of LDF and LASCA, according to previously published methods.1 ,4–7 Each capillary abnormality was scored by a validated semiquantitative rating scale by considering the average of the eight fingers.5 ,7 The appropriate NVC pattern of microangiopathy was assigned to the SSc patients: ‘Early’ NVC pattern (16 patients), ‘Active’ NVC pattern (19 patients) or ‘Late’ NVC pattern (26 patients) (figure 1).1 ,4 ,7 The microangiopathy evolution score (MES) was calculated as previously reported.5
Compliance of patients with instrumental examinations
Patients’ compliance was evaluated by a visual analogic scale (VAS, score 0–100), by asking the patients the following question: ‘By considering time of execution, ability to keep the position of your hand steady, and your feeling in general, how do you score this instrumental examination?’.
Statistical analysis
Statistical analysis was carried out by non-parametric tests. The Mann–Whitney U test was performed to compare unpaired groups of variables, and the Kruskal–Wallis test was used to compare continuous variables with nominal variables with more than two levels. The Spearman rank correlation test was employed to search for any relationships between variables, along with linear regression tests. Any p values lower than 0.05 were considered statistically significant. The results are reported as median and IQR.
Intraobserver variability
LDF and LASCA were performed twice within 1 h in both patients and controls by the same operator (blinded to disease status), and the reproducibility of the techniques was measured using the intraclass correlation coefficient (ICC) with 95% lower and 95% upper CI.
Results
Clinical characteristics of enrolled subjects are reported in online supplementary table S3.
PBP was significantly lower in SSc patients than in healthy subjects, as evaluated by both LASCA and LDF techniques (median PBP by LASCA 85[IQR25] vs 187[69] PU, respectively; median PBP by LDF 71[32] vs 185[72] PU, respectively) (p<0.0001). PBP was progressively decreasing in those SSc patients with an ‘Early’, ‘Active’ or ‘Late’ NVC pattern of microangiopathy, as evaluated by both LASCA and LDF techniques (median PBP by LASCA 90[67], 84[20] and 78[44] PU, respectively; median PBP by LDF 86[44], 75[18] and 63[29] PU, respectively) (p=0.04 and p=0.002, respectively) (figure 2). A statistically significant negative correlation between PBP values and MES, as evaluated by both LASCA (r=−0.41, p=0.002) and LDF (r=−0.40, p=0.002) was detected (figure 3). Patients with active or history of digital ulcers showed significantly lower PBP than those without (p=0.0003).
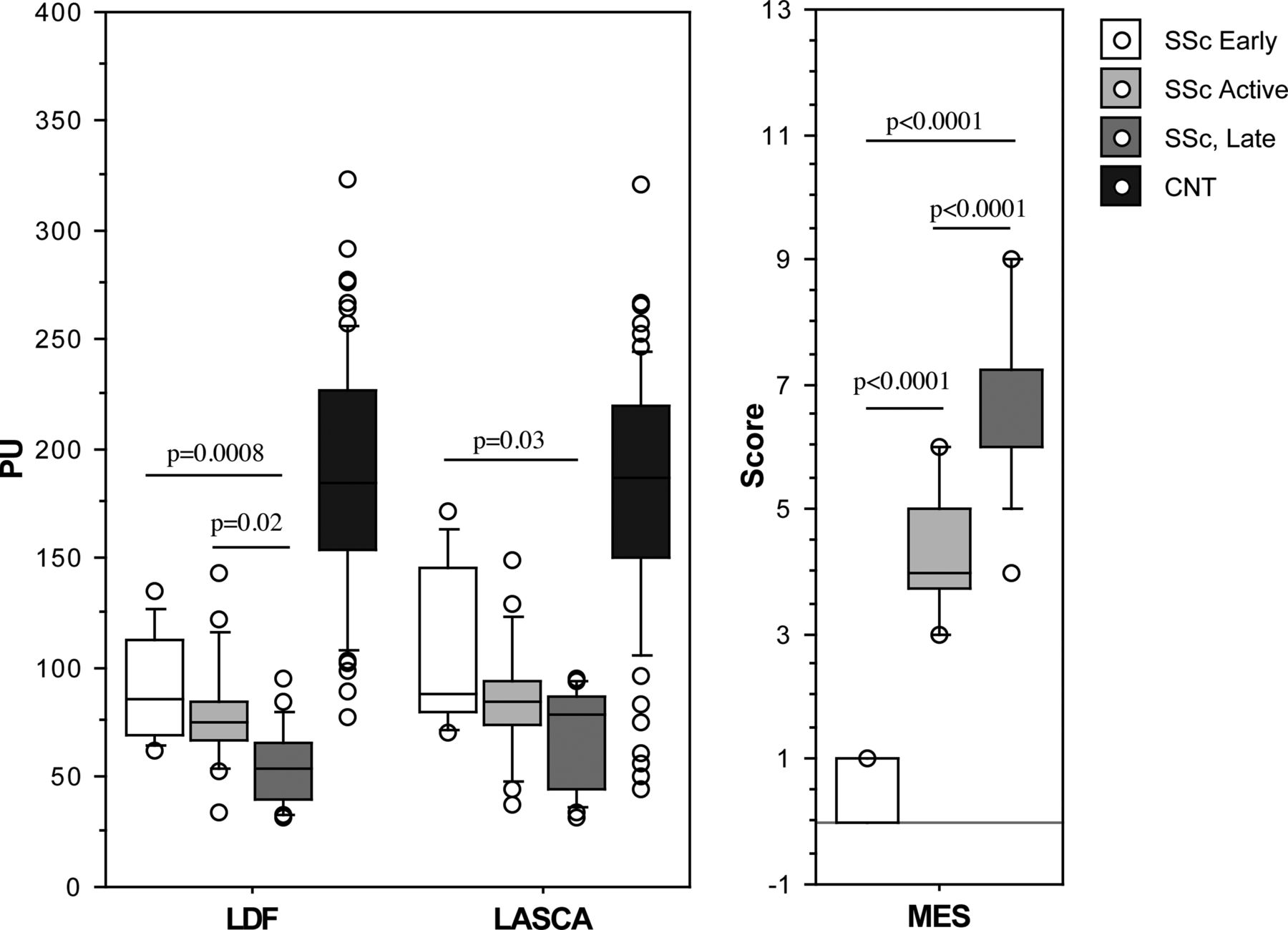
Fingertip blood perfusion, assessed by both laser speckle contrast analysis (LASCA) and laser Doppler flowmetry (LDF), in SSc patients showing different nailfold videocapillaroscopy patterns of microvascular damage (‘Early’, ‘Active’, ‘Late’ patterns), and in healthy subjects (CNT). The results are reported as perfusion units (PU). Data are given as box plots with the 5th, 10th, 50th (median), 90th, 95th percentiles. Microangiopathy evolution score (MES) in SSc patients is also reported. CNT, controls.

{kind=link}
{kind=link}
{kind=link}
Correlation between peripheral blood perfusion (PBP) values at level of fingertips, as evaluated with laser speckle contrast analysis (LASCA) and laser Doppler flowmetry (LDF) in both patients with systemic sclerosis (SSc) and healthy subjects (CNT), and correlation between PBP and microangiopathy evolution score (MES) evaluated by both LASCA and LDF.
A statistically significant positive correlation was detected between LASCA and LDF values in both SSc patients (r=0.91, p<0.0001) and healthy subjects (r=0.88, p<0.0001) (figure 3).
No statistical significant correlation was observed between PBP and age in either SSc patients or healthy subjects, as evaluated by LASCA (r=0.14, p=0.30; r=0.15, p=0.31, respectively) and LDF (r=0.10, p=0.47; r=0.11, p=0.35, respectively).
Patients with lcSSc showed higher PBP (median PBP by LASCA 87[26] PU, and by LDF 74[26] PU) than those with dcSSc (median PBP by LASCA 80[43] PU, and by LDF 58[39] PU) (p=0.05 for both LASCA and LDF).
The reproducibility was 88% for LDF (ICC 0.88, 95% CI 0.83 to 0.91) and 95% for LASCA technique (ICC 0.95, 95% CI 0.94 to 0.97).
Concerning patient compliance with instrumental examinations, VAS score resulted 89.8 for LASCA and 30.4 for LDF technique.
Discussion
LASCA may be considered a reliable tool in detecting PBP in SSc patients, as well as in healthy subjects. As detected by LASCA for the first time, PBP was found to decrease in SSc patients in correlation with progressive severity of nailfold pattern of microangiopathy, and in agreement with previous results obtained by the laser Doppler analysis.2 ,15 ,16 In particular, SSc patients showed the lowest PBP when they were characterised by the worst ‘Late’ NVC pattern of microangiopathy, when compared with the ‘Early’ less severe NVC.
Interestingly, the study reports a positive correlation between LASCA and LDF values (p<0.0001), supporting the working hypothesis that both methods are useful to assess PBP in SSc patients according to the severity of the microvascular damage.
On the other hand, recent analyses suggest that skin blood flow measurements obtained by LASCA and LDF techniques cannot be compared directly even after classical normalisation procedure.12 ,13 This technical problem is generated by the non-linear relationship existing between LASCA and LDF flow data. For example, due to the absence of contact between tissue and sensors, it is likely that different technical and environmental conditions may interfere with LASCA recordings versus the direct contact necessary with LDF analysis.13
LASCA was found significantly less time consuming than LDF, as PBP is registered at the level of the whole palm of the hands versus single fingers, (60 vs 480 seconds for LASCA vs LDF for both hands: 87% less time consuming) and therefore PBP values are recorded as PU in a large ROI. Additionally, LASCA shows lower intraoperator variability versus LDF analysis and is much better accepted by patients (patient compliance of 90% LASCA vs 30% LDF).
A recent study investigated PBP and microvascular reactivity by LASCA in consecutive patients affected by Raynaud's phenomenon at baseline and following dynamic stimulations.3 The study suggested, within SSc patients, a significant difference in ischaemic challenge between patients with early versus patients with definite disease, but the morphological status of the microvascular bed was not analysed in relation to LASCA values.3 Unlike this study, our investigation evaluated by LASCA the PBP in relation to different patterns of nailfold microvascular damage, showing a progressive decrease of PBP in SSc patients with a worse microangiopathy extent (‘Early’, ‘Active’, or ‘Late’ NVC patterns). This finding has a high relevance, since microvascular damage extent was further related to other clinical parameters involved in SSc activity/severity (PBP in this case), suggesting a putative role of NVC as a biomarker, as recently suggested.17
Furthermore, novel objective measures to assess peripheral perfusion might allow early identification of patients with critical ischaemia or early assessment of response to therapy, which might be helpful for clinical practice and studies.
In conclusion, LASCA provides, in a safe and fast way, more comprehensive information than single LDF analysis since it may assesses the PBP at different larger sites, such as the palm and dorsum of the hands and face in SSc patients. LASCA values linearly decrease with increase severity of microvascular alterations, as recently just supposed.18
The reliability and sensitivity of both LDF and LASCA assessment were not evaluated in this study. The evaluation of a larger and more homogeneous sample size might detect further statistically significant differences of PBP between SSc patients with different patterns of nailfold microangiopathy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
- Data supplement 3 - Online table 3
Footnotes
Handling editor Tore K Kvien
-
Contributors The manuscript has been seen and approved by all the authors that have given necessary attention to ensure the integrity of the work.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Obtained from Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.