Article Text

Abstract
Objectives In juvenile idiopathic arthritis (JIA), the efficacy of very early disease-modifying drug therapy, synthetic or biological, is not well known. Three alternative strategies were compared for treating recent‑onset polyarticular JIA.
Methods In a 54-week multicentre open-label clinical trial, 60 disease-modifying antirheumatic drug (DMARD)-naive patients aged 4–15 years were randomly assigned into three treatment arms. The efficacy of infliximab plus methotrexate (TNF) was compared to that of two synthetic therapies: methotrexate alone (MTX) and DMARD methotrexate, sulphasalazine and hydroxychloroquine in combination (COMBO). Primary endpoint was American College of Rheumatology paediatric 75% improvement (ACR Pedi 75). Secondary endpoints were inactive disease and safety.
Results In 59 patients, mean (±SE) age at baseline was 9.6±0.4 years, duration of JIA 1.9±0.2 months and number of active joints 18±1. ACR Pedi 75 was achieved in 100% (19/19) of patients receiving TNF, 65% (13/20) on COMBO (95% CI 44% to 86%) and 50% (10/20) on methotrexate (95% CI 28% to 72%) p<0.0001. Thirteen patients receiving TNF (68%; 95% CI 47% to 89%) achieved inactive disease, whereas eight (40%; 95% CI 22% to 63%) on COMBO and five (25%; 95% CI 6% to 44%) on methotrexate did (p=0.002). Patients on TNF spent a mean 26 weeks (95% CI 18 to 34) with inactive disease, longer than did those receiving COMBO (13 weeks; 95% CI 6 to 20), or methotrexate (6 weeks; 95% CI 2 to 10). Serious adverse events were rare.
Conclusion In early polyarticular JIA, targeting to achieve minimally active or inactive disease, infliximab plus methotrexate was superior to synthetic DMARD in combination and strikingly superior to methotrexate alone.
Statistics from Altmetric.com
Juvenile idiopathic arthritis (JIA), a heterogeneous group of chronic arthritides of unknown aetiology, is the most common rheumatic disease of childhood, with a global prevalence of 16–150 per 100 000.1 In up to 50% of patients, the disease course may be polyarticular, namely in the JIA subcategories of rheumatoid factor positive or negative polyarthritis, extended oligoarthritis, or enthesitis-related arthritis.1 2 In polyarticular disease, arthritis often remains active for longer periods than it does in persistent oligoarthritis,1 3 4 and patients may thus have disease of greater severity and higher risk prolonged.1 3,–,6 In recent studies, an early response to methotrexate at 6 months predicted better long-term outcome,7 and achieving inactive disease at least once within 5 years from onset also predicted less joint damage.8 Efforts to establish early effective therapies for polyarticular JIA should therefore be strengthened.
Until recently, the primary treatment of active juvenile polyarthritis has been a single disease-modifying antirheumatic drug (DMARD), most often methotrexate.9 10 Leflunomide11 or sulphasalazine12 have also proved to be feasible treatment options. In adult rheumatoid arthritis, in a number of controlled studies, synthetic DMARD combinations have proved more beneficial than monotherapy,13 especially when started early.14 To our knowledge, in JIA no controlled studies have reported on synthetic combination therapy, although in clinical practice, DMARD are commonly used in various combinations.
In DMARD-refractory JIA, the use of biological agents mainly with tumour necrosis factor antagonists began during the last decade.15,–,18 As the efficacy of these drugs has transformed the landscape of paediatric rheumatology, the goal of treatment in JIA has been changing from symptomatic relief and satisfactory improvement to complete remission.19 20 Taking into consideration both the high costs and possible long-term adverse events, determining the optimal use of biological agents in JIA is crucial.
We conducted this study to evaluate the efficacy of aggressive drug therapy in early polyarticular JIA, comparing biological combination therapy (infliximab plus methotrexate) with a conventional synthetic DMARD combination or methotrexate alone. Our aim was to find the optimal therapy in early polyarticular JIA when the endpoint is remission or at least low or minimal disease activity.
Methods
Patients
Eligible patients were aged 4–15 years with DMARD-naive early JIA and had received no systemic corticosteroid treatment. Arthritis had persisted for at least 6 weeks but not more than 6 months. The diagnosis and duration of JIA was confirmed by a paediatric rheumatologist. After extensive screening, arthritides other than of unknown origin (eg, Lyme disease, enteroarthritis, poststreptococcal arthritis) were excluded. Those with polyarthritis (at least five active joints and at least three joints with pain or tenderness and limitation of motion) were included. Patients with systemic JIA, any major concurrent medical condition, any abnormality in the haematopoietic or lymphatic system were excluded. For girls with reproductive capacity, pregnancy was excluded.
Study design
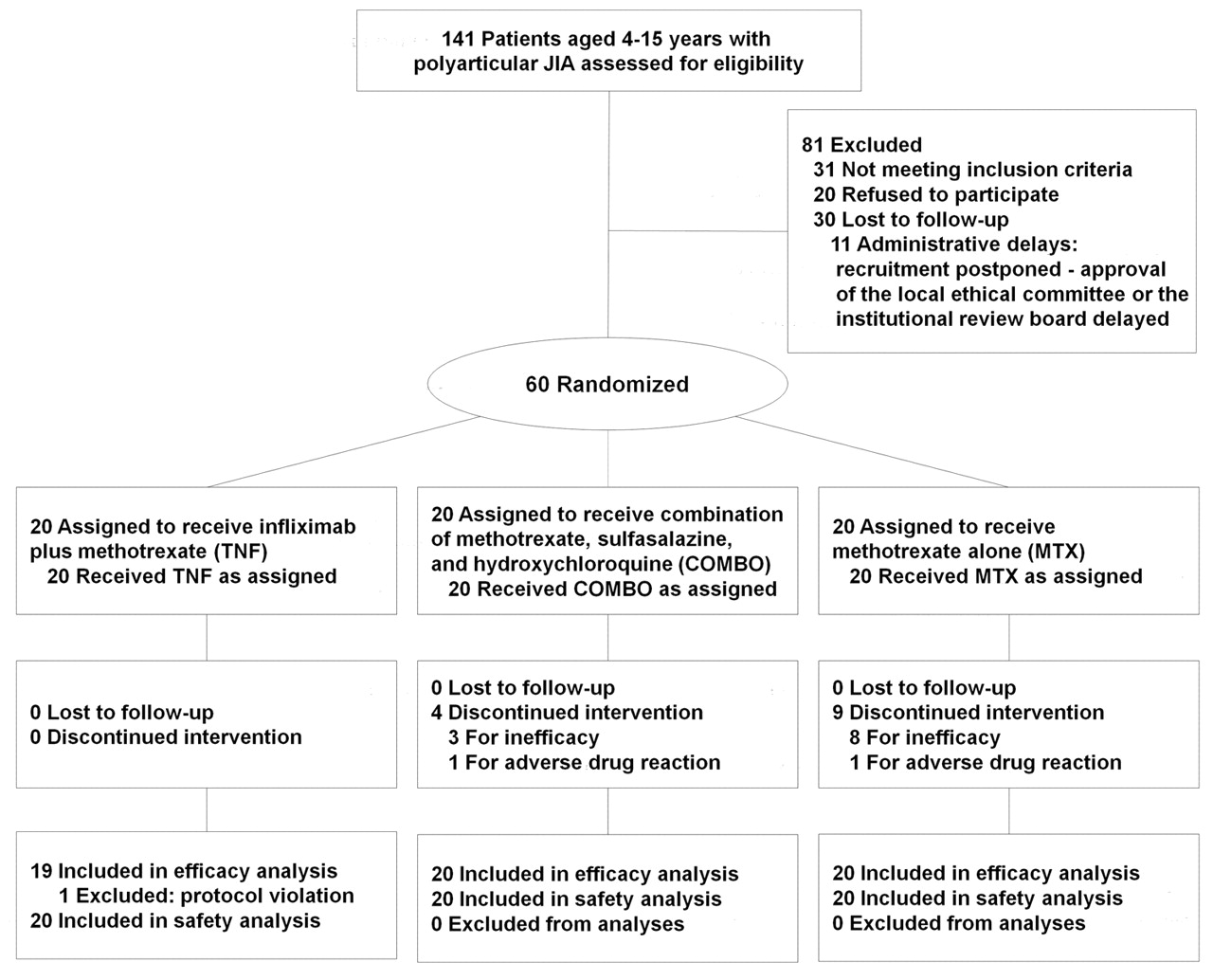
ACUTE–JIA was an investigator-initiated multicentre randomised open-label clinical trial, and was conducted based on the principles of the Declaration of Helsinki and Finnish regulatory requirements. The study protocol was approved by the Finnish Medicines Agency and by ethics committees at each study site. Informed consent was obtained from patients and their parents. Sixty patients from six Finnish tertiary care units were enrolled from May 2003 to November 2006 (figure 1) and were randomly assigned into one of three treatment arms: infliximab and methotrexate (TNF), a combination of methotrexate, sulphasalazine and hydroxychloroquine (COMBO), or methotrexate alone (MTX). Study visits occurred at baseline (0) and at 6, 12, 18, 24, 36, 48 and 54 weeks. The initial oral methotrexate dose was 15 mg/m2 weekly, up to 25 mg; for sulphasalazine, it was 40 mg/kg daily, up to 2000 mg; and for hydroxychloroquine, 5 mg/kg daily, up to 300 mg. Infliximab was given at 100 or 200 mg (3–5 mg/kg), based on the recommendations then in use, as were infusion intervals at 0, 2 and 6 weeks, and thereafter every 6 weeks. Intra-articular corticosteroids and non-steroidal anti-inflammatory drugs were permitted for symptomatic treatment of arthritis. To avoid subcutaneous atrophy, triamcinolone hexacetonide was used for larger and methylprednisolone acetate for smaller joints. For cumulative exposure to intra-articular steroids, each 1 mg of methylprednisolone was estimated to have the anti-inflammatory properties of 1 mg triamcinolone.21
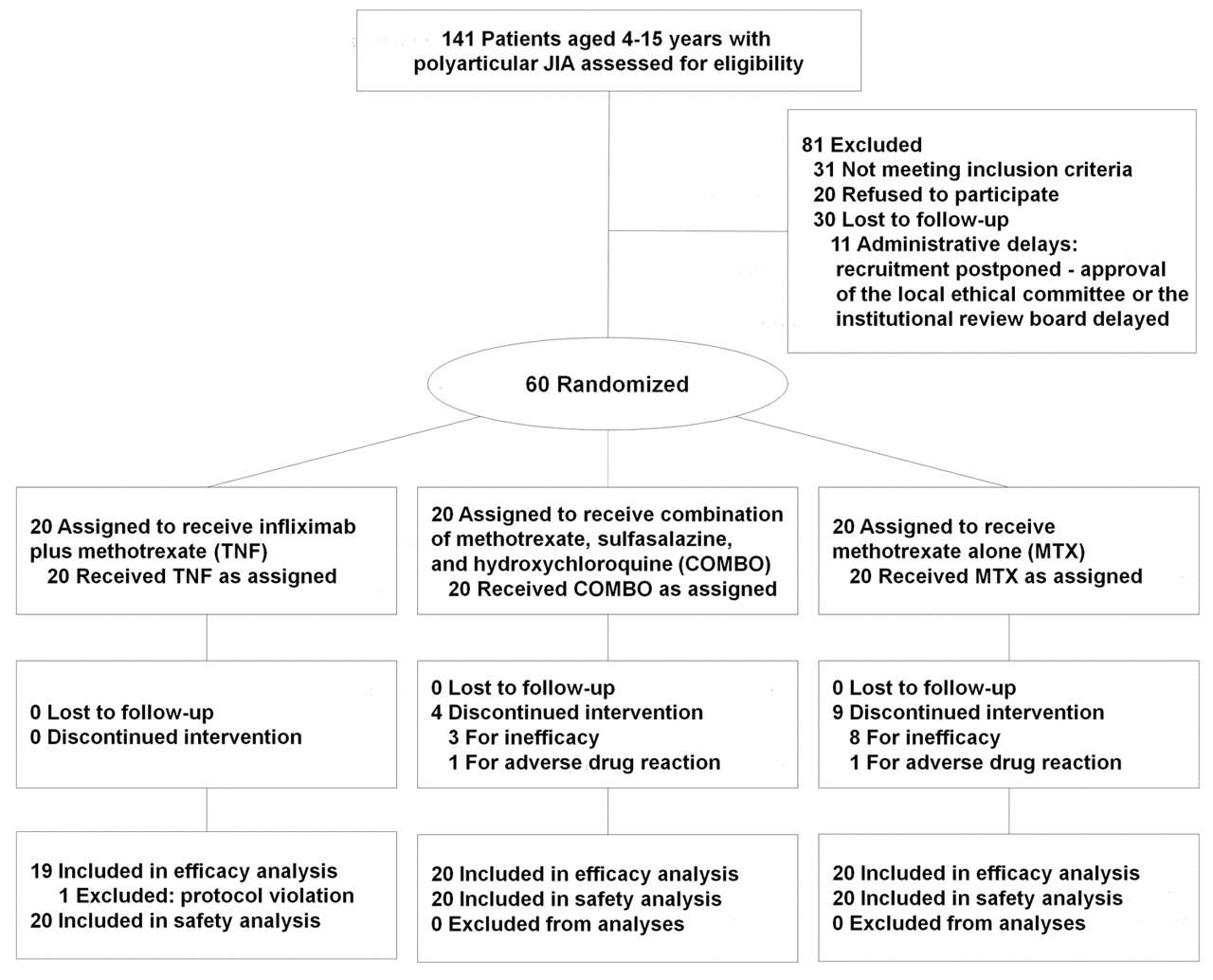
Enrolment and follow-up of 60 patients with polyarticular juvenile idiopathic arthritis (JIA) in three treatment arms. COMBO, methotrexate, sulphasalazine and hydroxychloroquine in combination; MTX, methotrexate alone; TNF, infliximab plus methotrexate.
American College of Rheumatology paediatric (ACR Pedi) responses were assessed at each study visit.22 If ACR Pedi 75 was not reached by 12 weeks or thereafter in any of the treatment arms, methotrexate was doubled to 30 mg/m2 weekly up to 25 mg and administered parenterally. Failure occurred if side-effects prevented the use of the study drug or if ACR Pedi 30 was not reached despite dose escalation.
Definition of improvement and inactive disease
In the modified ACR Pedi criteria, we used the following six core set variables obtained at each visit: erythrocyte sedimentation rate (ESR); number of active joints; number of joints with pain or tenderness and limitation of motion; physician's global assessment of disease severity, ie, the physician's visual analogue scale (VAS, range 0–100 mm); parents’ global assessment of the child's wellbeing, ie, the patient VAS; and assessment of the child's functional ability by the childhood health assessment questionnaire (CHAQ, range 0–3).15 22 ACR Pedi 30 was defined as an improvement of at least 30% in three of the six core criteria with no more than one of the criteria worsening by 30% or more. In ACR Pedi 50, 70, 75, 90 or 100, improvement had to be at least 50%, 70%, 75%, 90% or 100%, respectively, and no more than one of the core criteria worsening by 30% or more.
Inactive disease (on medication) was defined a priori as follows: no active synovitis, uveitis, fever, rash, serositis, or other manifestation of active rheumatic disease, ESR less than 20 mm/h, no need for oral steroids, and a minimum of 6 weeks from the last intra-articular corticosteroid injection. We used the current definition of inactive disease3 in post-hoc analyses.
Primary endpoint and secondary outcome measures
The primary endpoint at week 54 was ACR Pedi 75. Secondary outcomes were clinically inactive disease, time spent in a state of inactive disease or ACR Pedi 75, drug survival, frequency of adverse events or side-effects, and ACR Pedi 30, 50, 70, 90 and 100 responses.
Statistical methods
Block randomisation without stratification was centrally organised into three treatment arms with 20 patients each, which was estimated to provide 80–90% power to compare primary and secondary endpoints between TNF and methotrexate only, and TNF and COMBO. Baseline differences between groups were assessed by χ2, Fisher's exact or Kruskal–Wallis test when appropriate and differences within groups by Dunn's test. All comparisons were two-sided with a 0.05 significance level. Drug survival and reaching ACR Pedi 75 or inactive disease were performed by Kaplan–Meier and comparison of drugs by Mantel–Cox analyses. Longitudinal analysis of continuous ACR Pedi core criteria (with last observation carried forward if failure occurred during weeks 12–54) were performed by Friedman's test and multiple comparisons by Dunn's test. The comparison of the groups in reaching ACR Pedi 30–100 was analysed by generalised estimation equation models.
The trial was primarily registered with the Hospital District of Helsinki and Uusimaa (http://www.hus.fi) clinical trials number 211864, and recently with ClinicalTrials.gov, number NCT01015547.
Role of the funding source
Funding sources of the study were non-commercial and not involved in study design, data collection or analysis. Of the study drugs, infliximab was purchased by research funds of each hospital, or by research grants, and DMARD were reimbursed by national health insurance.
Results
Patient characteristics
All 60 patients completed the trial. One was excluded from the final efficacy analyses due to protocol violation. No significant differences in baseline demographics were evident between the treatment arms TNF, COMBO and MTX (table 1). Values in four out of the six ACR Pedi core criteria were comparable. Those receiving MTX had higher scores than those receiving TNF according to two parental reports: patient VAS (p=0.007) and CHAQ (p=0.02).
Baseline demographics and ACR Pedi core criteria in 59 patients with JIA, randomly assigned into three treatment arms: TNF, COMBO or MTX
The one excluded patient had received TNF and was a responder reaching ACR Pedi 75 at week 36 and inactive disease at week 54. Exclusion was due to the possible confounding effect of concurrent systemic steroids during weeks 30–54 (at the final visit, 0.1 mg/kg daily). Two other patients received low-dose corticosteroids only at the beginning of the study (mean 0.1 mg/kg; weeks 10–15 and 0–18), which was considered a minor protocol violation not affecting the results.
During the follow-up based on the study protocol, one patient on TNF, seven on COMBO and 14 on methotrexate only switched to a parenteral, escalated methotrexate dose.
ACR Pedi 75 response
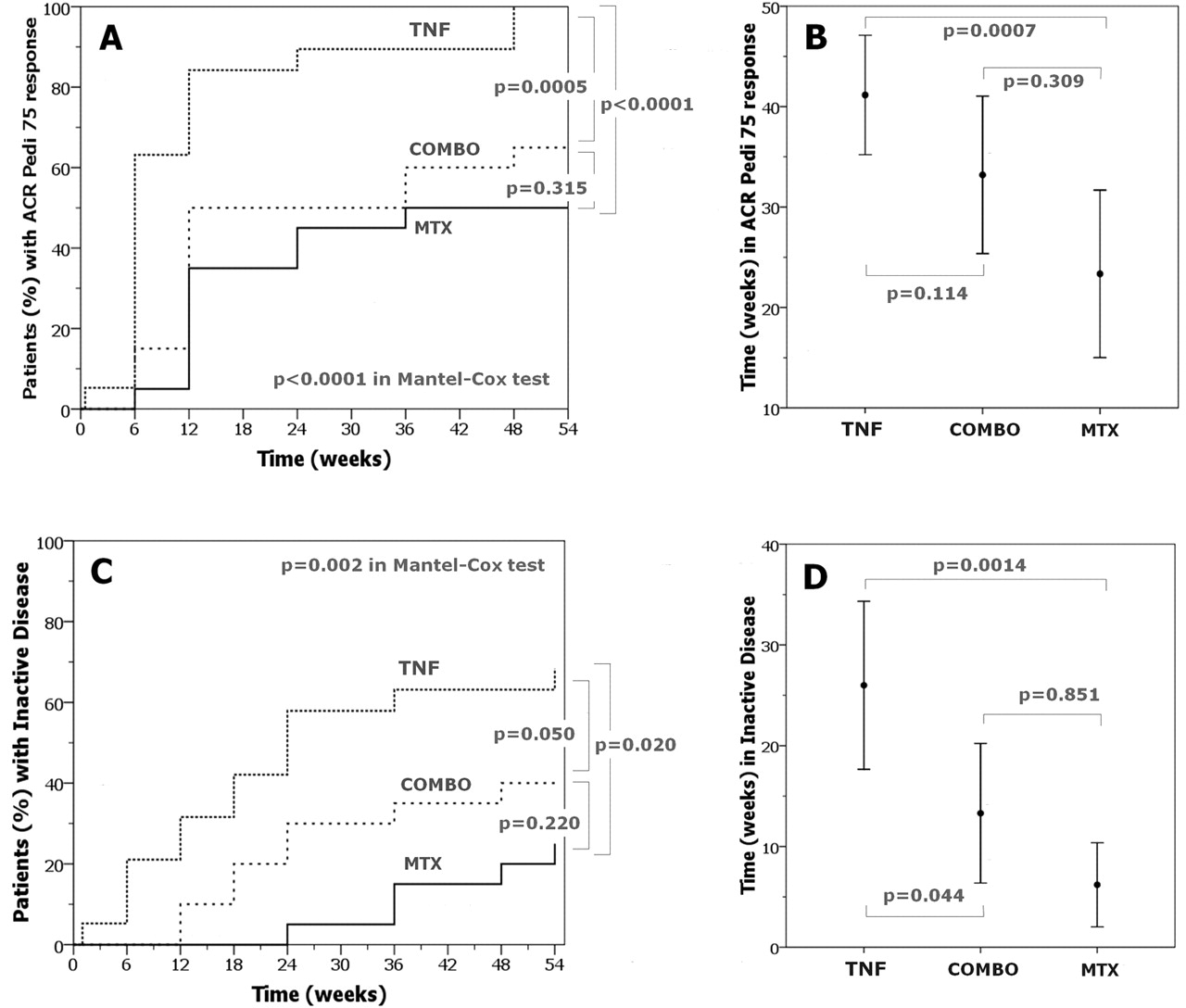
Of the 59 patients, 42 (71%) reached an ACR Pedi 75 response: 19/19 patients (100%) receiving TNF, 13/20 (65%; 95% CI 44% to 86%) on COMBO and 10/20 (50%; 95% CI 28% to 72%) on methotrexate, p<0.0001. Differences between TNF and MTX arms (p<0.0001), and TNF and COMBO arms (p=0.0005) were significant (figure 2A). During 54 weeks, patients receiving TNF experienced episodes of an ACR Pedi 75 response for a mean of 41 weeks (95% CI 35 to 47), those on COMBO for 33 (95% CI 25 to 41), and on methotrexate for 22 weeks (95% CI 15 to 32), p=0.001 (figure 2B).

Primary and secondary endpoints for patients treated with infliximab and methotrexate (TNF), methotrexate, sulphasalazine, hydroxychloroquine (COMBO) or methotrexate alone (MTX). Kaplan–Meier curves illustrate the proportion (%) of 59 patients with JIA achieving American College of Rheumatology paediatric (ACR Pedi) 75 response (A) or inactive disease (C) in the three treatment arms. Based on Mantel–Cox test, group comparisons in both panels A and C were significant; p<0.0001 and p=0.002, respectively. Error bars depict means and 95% CI of the time shown in low disease activity, ie, ACR Pedi 75 response (B), or inactive disease (D) during the 54-week trial. Differences between the treatment arms in both panels B and D in the Kruskal–Wallis test were significant (p=0.001).
Inactive disease
At 54 weeks, of those receiving TNF, 13 patients (68%; 95% CI 47% to 89%) achieved inactive disease, whereas eight (40%; 95% CI 22% to 63%) receiving COMBO and five (25%; 95% CI 6% to 44%) receiving methotrexate only achieved this target (p=0.002, figure 2C). Moreover, patients on TNF spent a mean of 26 weeks (95% CI 18 to 34), on COMBO 13 weeks (95% CI 6 to 20), and on MTX 6 weeks (95% CI 2 to 10) in a state of inactive disease (p=0.001, figure 2D). Post-hoc analyses, using the current definition of inactive disease3 strengthened the results in favour of the TNF arm (supplementary eTable, available online only).
Other ACR Pedi responses
The odds of reaching the ACR Pedi 30, 50, 70, 90 and 100 responses were superior for those receiving TNF compared with those on MTX. The odds of achieving the targeted ACR Pedi levels were higher in those on TNF than in those on COMBO, but reached statistical significance only in ACR Pedi 30 and 70 (figure 3, table 2). Values for individual ACR Pedi core criteria improved in all groups compared with baseline, excluding CHAQ in TNF and COMBO. Of note, ESR at baseline fell within the normal range in 42% of the patients.

{kind=link}
{kind=link}
{kind=link}
Proportion (%) of patients achieving American College of Rheumatology paediatric (ACR Pedi) 30, 50, 70, 90 and 100 responses in the three treatment arms (infliximab plus methotrexate (TNF), methotrexate, sulphasalazine, hydroxychloroquine (COMBO) and methotrexate alone (MTX) during the 54-week trial is shown in panels A–E.
ACR Pedi 30, 50, 70, 90 and 100 responses, and changes in individual ACR Pedi core criteria at 54 weeks in the three treatment arms
Intra-articular steroids
Especially at the beginning of the trial, intra-articular corticosteroid injections relieved inflammatory pain and swelling. Not only the cumulative amount of intra-articular steroids given but also the cumulative number of joints injected within 54 weeks was lower for TNF (median 8; range 0–53) than for MTX (22; 9–50) or COMBO (24; 5–64) (supplementary eFigure, available online only).
Drug survival
Altogether 80% of the patients (46/59) were able to continue their treatment strategy throughout the study. Drug survival (ie, continuation rate on drug) was 100% on TNF, 80% (95% CI 63% to 97%) on COMBO and 55% (95% CI 33% to 77%) on methotrexate (p=0.003). Drug survival rates were higher for TNF than for methotrexate (p=0.001) or COMBO (p=0.04).
With COMBO, four patients (20%) discontinued treatment; three due to inefficacy (ACR Pedi less than 30 in two, erosion of hip at week 12 in one) and one due to gastritis symptoms and weight loss. In those receiving MTX, nine patients (45%) discontinued treatment, eight due to inefficacy. Five of these did not achieve ACR Pedi 30. For the remaining four patients, uveitis occurred in one and multiple joint erosions at week 36 in another. The one with new-onset uveitis had received the maximal parenteral dose of MTX and had concurrent adrenal insufficiency due to multiple intra-articular corticosteroid injections. Two other patients on MTX failed in treatment compliance, one due to worsening of pain and the other due to intractable nausea.
Adverse events
The most frequently reported adverse events were infections in 51 patients (85%), gastrointestinal symptoms in 37 (56%), elevation of liver enzymes in 21 (36%) and changes in haematological parameters in 15 (25%) (table 3). Twenty-one events (7%) were considered severe. Of those, 18 events occurred in 13 patients receiving MTX. Gastrointestinal symptoms, nausea, loss of appetite and weight loss seemed to occur more commonly in COMBO than in other treatment groups.
Adverse events in 60 patients with JIA in three treatment arms: TNF, COMBO or MTX
Discussion
The present study is, to our knowledge, the first to introduce a clinically significant primary endpoint—the ACR Pedi 75—for efficacy evaluation of drug therapy in polyarticular JIA. Until now, the primary target response in major studies investigating the efficacy of conventional DMARD10 or biological agents15,–,17 23 has been ACR Pedi 30. This magnitude of improvement in the era of biological disease-modifiers can no longer be considered a sufficient therapeutic response. Over the past decade, alongside the introduction of new efficacious treatment options for JIA, increased emphasis has been focused on achieving complete disease control.
Achievement of at least ACR Pedi 75 usually indicates low disease activity.24 25 After 1 year of therapy, infliximab plus methotrexate proved to be superior to methotrexate alone. The greater efficacy of early biological therapy was also evident when compared with that of a synthetic DMARD combination. Among the most interesting and clinically important findings were striking differences in the time spent in an inactive versus an active state of disease. Those on TNF spent approximately 6 months with clinically inactive disease, whereas those on COMBO spent 3 and those on methotrexate only 1 month in such a state. Given the chronic nature of polyarticular JIA, the potential for long-term damage to joints and the deterioration of quality of life in the continually active disease, it is justifiable that the goal of treatment strategies should be inactive disease. This point of view is supported by a recent study reporting even mild clinical symptoms as being associated with suboptimal quality of life.26
Besides a clinically meaningful endpoint, another novelty of the present study was the timing of aggressive drug therapy for JIA. We were able to commence aggressive disease-modifying therapy very early on. This is possible in a healthcare system in which all children with persistent joint symptoms are referred to specialised care without delay. Evidence suggesting that early disease control determines long-term outcome in patients with arthritis has come mainly from adult studies.14 27 28 We demonstrated a clinically significant short-term outcome. Whether early remission of the disease is beneficial in the long run remains to be seen in ongoing follow-up studies.
In the current management of polyarticular JIA with traditional DMARD, non-steroidal medications and intra-articular steroids are effective in reducing symptoms of arthritis, but JIA has as yet no cure. Compared with biological therapy, the efficacy of methotrexate alone and even in combination with sulphasalazine and hydroxychloroquine was inferior. Our choice of a challenging primary endpoint (ACR Pedi 75) influenced outcomes because the achievement of ACR Pedi 30 would have been more feasible with methotrexate alone. A higher methotrexate dose also failed to result in clinical improvement; it only led to increased frequency of adverse events, which concurs with previous findings.10 Following a treat-to-target approach, the lower efficacy of conventional DMARD alone or in combination was reflected in a greater need for intra-articular steroids. However, their more frequent administration apparently failed to alter the disease course, but repeated injections were occasionally associated with temporary adrenal insufficiency. Of cautionary note, the amount of steroids—even as local injections—has to be balanced with other drugs when aiming at low disease activity or inactive disease. Because of the well-known negative long-term consequences of steroids for metabolism, growth and bone health,29 30 the study design allowed no systemic steroids.
Not only was the efficacy of infliximab plus methotrexate better, but adverse events also seemed more common with methotrexate alone, including serious adverse events relating to disease activity such as new-onset uveitis and joint erosion. In contrast, a combination of DMARD was reasonably well tolerated, although gastrointestinal symptoms in some individuals limited their use. It can, however, be speculated that long-term compliance with combination DMARD in children and adolescents may be easily compromised by the requirement for several drug doses daily.
The present study has obvious limitations. A non-blinded setting and drug infusions in one treatment arm only increased the possibility of bias in favour of biological therapy. We initially planned to start with etanercept, but its supply was insufficient before 2004, so we initiated infliximab instead. This monoclonal antibody against tumour necrosis factor was then and is still now used off-label for JIA. In one head-to-head comparison of etanercept and infliximab in DMARD-refractory JIA patients, outcomes were, however, comparable.24 Although we conducted a nationwide study, our recruitment phase took 2 years longer than expected mainly due to strict inclusion criteria, excluding a large group of JIA patients who are under the age of 4 years. Moreover, randomisation could not totally exclude differences in baseline characteristics. That those on methotrexate had higher scores for parent-derived core criteria may reflect some true baseline differences favouring the other treatment groups. The inclusion of all polyarticular forms of JIA enhanced the heterogeneity of the study population. Finally, our treatment groups were relatively small. Although the study was powered to detect differences between biological and synthetic DMARD, it was not powered to compare the two synthetic treatment arms. Whether the present results can be generalised to larger numbers, to those younger than 4 years, or to patient groups outside of Scandinavia with a higher incidence of rheumatoid factor-positive JIA31 is yet to be seen.
In conclusion, the present study introduced a completely new aggressive approach for the treatment of polyarticular JIA. Although early biological treatment was highly successful, our results do not necessarily imply that every new patient with polyarticular JIA should be treated with a biological agent. This conclusion can be supported by our finding that at 12 months half the patients on methotrexate alone had achieved an ACR Pedi 75 response. Predictors for good response to methotrexate would prove highly valuable. The recent US Food and Drug Administration concern about possible long-term malignancies in paediatric patients on tumour necrosis factor blockers also has to be taken into account,32 and biological agents may have still other unknown long-term side-effects. One possible treatment strategy for active polyarticular JIA may be the use of a biological agent early in the disease course to induce remission, and after achievement of inactive disease, treatment would continue with DMARD, thus possibly minimising both exposure to biological agents and the length of the active disease episode. Whether interfering early in the disease process with anti-TNF therapy would change the biology of the disease remains to be seen in ongoing follow-up studies. It is obvious that prospective and retrospective studies are necessary to optimise the treatment of polyarticular JIA.
Acknowledgments
The authors thank all patients and their parents who made this trial possible. Hannu Kautiainen is acknowledged for aid in study design and randomisation, and Drs Katarina Tamm and Eija Piippo-Savolainen for patient follow-up and research nurses for administrative aid.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
VH and PL contributed equally to this work.
-
Funding This study was funded by research grants from Hospital Districts of Helsinki and Uusimaa, Oulu, Kuopio, Turku and Päijät-Häme; the Rheumatism Foundation Hospital; the Päivikki and Sakari Sohlberg Foundation; the Foundation for Pediatric Research, Finland; and the Scandinavian Rheumatology Research Foundation.
-
Competing interests VH is a current employee of UCB Pharma and reports ownership of stock options.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Coordinating Ethical Committee, Helsinki University Central Hospital, Finland.
-
Provenance and peer review Not commissioned; externally peer reviewed.