Article Text

Abstract
Objective To assess the progression of radiographic sacroiliitis in a cohort of patients with early axial spondyloarthritis over a period of 2 years and to explore predictors of progression.
Methods 210 patients with axial spondyloarthritis from the German Spondyloarthritis Inception Cohort have been selected for this analysis based on availability of radiographs at baseline and after 2 years of follow-up. Radiographs were centrally digitised and the sacroiliac joints were scored independently according to the grading system of the modified New York criteria for ankylosing spondylitis (AS) by two trained readers. The readers scored both time points simultaneously but were blinded for the time point and for all clinical data.
Results 115 patients (54.8%) fulfilled the modified New York criteria for AS in their radiographic part in the opinion of both readers at baseline, while 95 patients (45.2%) were classified as non-radiographic axial spondyloarthritis. More patients with non-radiographic spondyloarthritis (10.5%) compared with AS (4.4%) showed an estimated ‘true’ progression by at least one grade according to both readers, although the difference between the two groups was statistically non-significant. The rate of progression from non-radiographic axial spondyloarthritis to AS was 11.6% over 2 years. An elevated level of C-reactive protein (CRP) at baseline was a strong positive predictor of radiographic sacroiliitis progression in non-radiographic axial spondyloarthritis and AS (OR 3.65 and 5.08, respectively, p<0.05).
Conclusion Progression of radiographic sacroiliitis by at least one grade after 2 years occurs only in a small percentage of patients with early axial spondyloarthritis. An elevated level of CRP was found to be a strong positive predictor of sacroiliitis progression.
Statistics from Altmetric.com
It has been known for many years that inflammation in axial spondyloarthritis starts in the sacroiliac joints,1 a fact that had given radiographic sacroiliitis a dominant role in the modified New York classification criteria for ankylosing spondylitis (AS)2 and, more recently, also active inflammation of the sacroiliac joints on MRI in the new assessment of spondyloarthritis international society classification criteria for axial spondyloarthritis.3 4 The current concept of axial spondyloarthritis considers non-radiographic axial spondyloarthritis and AS as two stages of one disease, implying that sacroiliitis as seen on x-rays is evolving over time.5 While there has been considerable interest recently in the rate of progression of structural damage in the spine of AS patients, only limited data are available regarding the rate of progression of radiographic sacroiliitis, as the rate of transition from non-radiographic axial spondyloarthritis to AS, and about predictors of progression.6,–,11 The current study investigated the rate of radiographic progression in the sacroiliac joints over 2 years in patients with non-radiographic axial spondyloarthritis and in patients with AS with a relatively short disease duration from the recently described German Spondyloarthritis Inception Cohort (GESPIC).12
Methods
Patients
The design of the GESPIC, inclusion and exclusion criteria were reported elsewhere.12 In brief, patients included in the GESPIC were required to have a definite clinical diagnosis of axial spondyloarthritis according to the local rheumatologist. Patients were further classified based on the radiographic findings, and irrespectively of the presence of concomitant psoriasis or inflammatory bowel disease, as AS or as non-radiographic axial spondyloarthritis. Patients with AS ought to fulfil the modified New York criteria2 and the duration of symptoms was restricted to 10 years or less at the time of inclusion. Patients with non-radiographic axial spondyloarthritis ought to fulfil European Spondylarthropathy Study Group criteria, which were slightly modified,12 13 and had to have a duration of symptoms of 5 years or less. If both x-ray readers (see below) concordantly classified patients as AS or non-radiographic axial spondyloarthritis, based on the grade of radiographic sacroiliitis, and if this judgement differed from that of the local rheumatologist, the classification of the readers was used.
Altogether, 210 patients (115 patients with AS and 95 with non-radiographic axial spondyloarthritis) out of the previously reported 462 patients12 were included in the current study based on the availability of x-rays of sacroiliac joints obtained at baseline and after 2 years of follow-up. Baseline characteristics of the patient subsets are presented in table 1. There were no clear differences between the subset investigated here and the previously described whole cohort12 regarding baseline characteristics, except a lower percentage of men in the non-radiographic axial spondyloarthritis subgroup (33.7% in the current study vs 42.9% in the whole cohort).
Baseline characteristics of the included patients
Radiographs and scoring
x-Rays of sacroiliac joints (the rheumatologists were asked to perform standard anteroposterior pelvic radiographs) were performed locally at baseline and after 2 years of follow-up. Images were centrally collected, digitised, anonymised and subsequently scored independently by two trained readers (DP, HH). Grading of sacroiliitis was performed according to the established scoring system2 14:
▶ Grade 0—normal
▶ Grade 1—suspicious changes
▶ Grade 2—minimal abnormality, small localised areas with erosion or sclerosis, without alteration in the joint width
▶ Grade 3—unequivocal abnormality, moderate or advanced sacroiliitis with one or more of: erosions, evidence of sclerosis, widening, narrowing, or partial ankylosis
▶ Grade 4—severe abnormality, total ankylosis.
The readers scored the images of both time points from every patient simultaneously in a concealed randomly selected order and were blinded for all clinical data. The radiographic criterion of the modified New York criteria for AS was considered to be fulfilled if at least grade 2 sacroiliitis bilaterally or grade 3 unilaterally was evident.
Progression of radiographic sacroiliitis over 2 years was assessed on the level of sacroiliac joints as an absolute change of the grade (mean of two readers) and on the patients' level as a percentage of patients with progression. The latter was defined as worsening of sacroiliitis by at least one grade of either the right or left sacroiliac joint in the opinion of both readers. Similarly, regression of sacroiliitis on the patient's level was defined as an improvement by at least one grade in the opinion of both readers. As the true regression of structural changes of sacroiliac joints detected by x-rays is unlikely, the regression rate was used for the calculation of the estimated (‘true’) progression rate: observed progression rate minus observed regression rate.
Statistics
Scale variables are described as mean±SD. Agreement between two readers regarding radiographic sacroiliitis grade, fulfilment of the modified New York criteria and change in sacroiliitis grade over 2 years was assessed by means of the weighted κ value. Ninety-five per cent CI for the rates of sacroiliitis progression (Wilson's method) and differences in rates of progression (Jeffrey Parks' method) were calculated. The difference was considered to be statistically significant if the lower bound of the 95% CI was above zero. In order to identify predictors of sacroiliitis progression univariate and multivariate regression analyses were performed. OR and its 95% CI was calculated for each predictor candidate. A p value of less than 0.05 was considered to be statistically significant.
Results
At baseline, 115 patients (54.8%) fulfilled the radiological criterion of the modified New York criteria according to both readers and, therefore, were classified as patients with AS. Interestingly, among 117 patients who were classified initially (by the local rheumatologist) as AS, the presence of sacroiliitis satisfying the modified New York criteria was confirmed in 96 cases (82.1%) by both readers. Among patients who were classified initially as non-radiographic axial spondyloarthritis, 19 (20.4%) fulfilled the modified New York criteria for AS in the opinion of both readers and, therefore, were reclassified.
There was moderate agreement between the two readers regarding the grade of sacroiliitis at baseline (weighted κ value 0.51 (95% CI 0.44 to 0.59) and 0.59 (95% CI 0.52 to 0.66) for the left and right sacroiliac joints, respectively) and after 2 years of follow-up (weighted κ value 0.55 (95% CI 0.49 to 0.63) and 0.58 (95% CI 0.51 to 0.65) for the left and right sacroiliac joints, respectively). There was a similar level of agreement regarding the fulfilment of the modified New York criteria at baseline (κ=0.59) and after 2 years of follow-up (κ=0.67).
Among 122 sacroiliac joints from 61 AS patients with symptom duration of 5 years or less, sacroiliitis grades (mean of two readers' scores) were observed with the following frequencies: grade 1.5 in 1.6%, grade 2 in 20.5%, grade 2.5 in 30.3%, grade 3.0 in 32.0%, grade 3.5 in 9.0% and grade 4.0 in 6.6% of the joints. In 54 AS patients with symptom duration greater than 5 years (108 sacroiliac joints) sacroiliitis grade 3 and above was observed more frequently: grade 1.5 in 1.9%, grade 2 in 13.9%, grade 2.5 in 20.4%, grade 3.0 in 39.8%, grade 3.5 in 10.2% and grade 4.0 in 13.9% of the joints. The sacroiliitis grades in 95 non-radiographic axial spondyloarthritis patients (190 sacroiliac joints) were nearly normally distributed around grade 1: mean grade 0 sswas observed in 13.2% of the joints, grade 0.5 in 17.4%, grade 1 in 28.4%, grade 1.5 in 23.2%, grade 2 in 12.6% and grade 2.5 in 5.3% of the joints.
Sacroiliitis progression over 2 years
After 2 years of follow-up, changes of initial sacroiliitis grades were observed in the majority of patients in the non-radiographic axial spondyloarthritis group—figure 1A, whereas less than 50% of the AS group showed progression of sacroiliitis—figure 1B. The mean rate of progression of radiographic sacroiliitis over 2 years was low: 0.07 (95% CI −0.05 to 0.19) and 0.09 (95% CI −0.03 to 0.21) grades for the left and right sacroiliac joint, respectively, in non-radiographic axial spondyloarthritis, and with 0.06 (95% CI −0.01 to 0.13) and 0.05 (95% CI −0.04 to 0.14) grades for the left and right sacroiliac joint, respectively, in AS.
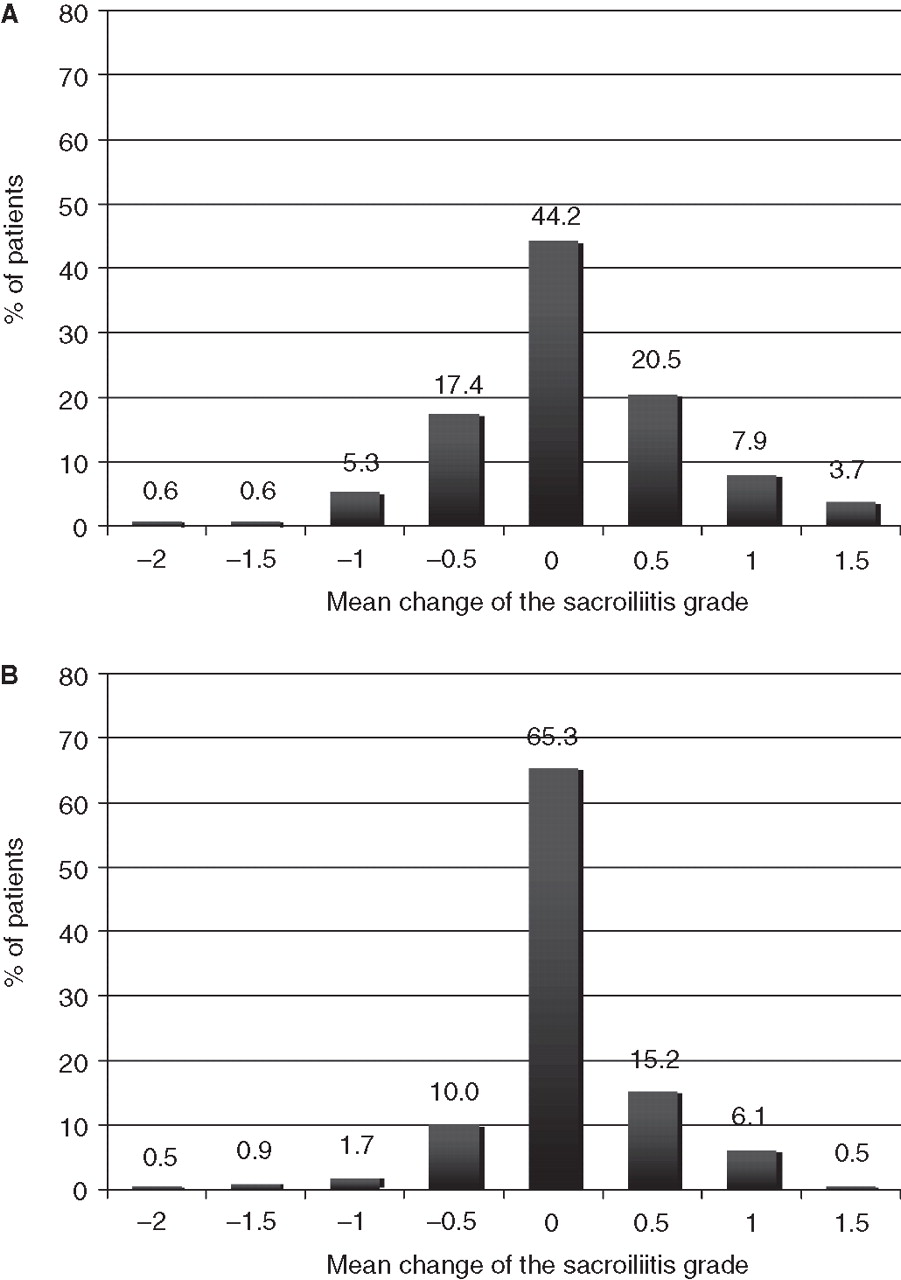
Rates of radiographic sacroiliitis grade change (mean of two scores) over 2 years in patients with non-radiographic (A) axial spondyloarthritis and (B) ankylosing spondylitis.
In patients with non-radiographic axial spondyloarthritis (n=95) progression of radiographic sacroiliitis by at least one grade in the opinion of both readers was observed in 16 patients (16.8%, 95% CI 10.6% to 25.6%). At the same time, sacroiliitis improvement by at least one grade was found in six patients (6.3%, 95% CI 2.9% to 13.1%). Therefore, the estimated ‘true’ sacroiliitis progression rate in non-radiographic axial spondyloarthritis was 10.5% (95% CI 1.3% to 19.3%)—figure 2.

{kind=link}
{kind=link}
Estimated ‘true’ progression rates (mean and 95% CI) of radiographic sacroiliitis in patients with ankylosing spondylitis and non-radiographic axial spondyloarthritis over 2 years. Estimated ‘true’ progression rate of radiographic sacroiliitis was calculated as a difference between observed progression (percentage of patients with worsening of radiographic sacroiliitis by at least one grade in opinion of both readers) and regression (percentage of patients with improvement of radiographic sacroiliitis by at least one grade in opinion of both readers) rates over 2 years.
Among 115 AS patients, the rate of radiographic progression in the sacroiliac joints was lower: 10 patients (8.7%, 95% CI 4.8% to 15.3%) showed worsening of sacroiliitis by at least one grade in the opinion of both readers, whereas regression of sacroiliitis was observed in five cases (4.35%, 95% CI 1.9% to 10.8%), resulting in an estimated ‘true’ sacroiliitis progression rate of 4.35% (95% CI −2.2% to 10.7%) in AS—figure 2. However, the observed difference in progression between non-radiographic axial spondyloarthritis and AS (6.2%, 95% CI −1.1% to 13.5%) was statistically non-significant. If the 21 patients with complete ankylosis of the sacroiliac joints were removed from the analysis the rates were similar: observed progression rate 10.6% (95% CI 5.9% to 18.5%), observed regression rate 4.3% (95% CI 1.7% to 10.4%), estimated ‘true’ progression rate 6.4% (95% CI −1.3% to 13.8%).
In the whole cohort of 210 patients with axial spondyloarthritis, 26 patients (12.4%, 95% CI 8.6% to 17.5%) showed progression of sacroiliitis by at least one grade over 2 years in the opinion of both readers. At the same time, 11 patients demonstrated an improvement of sacroiliitis by at least one grade, resulting in a rate of regression of 5.2% (95% CI 3.0% to 9.1%). Therefore, the estimated ‘true’ progression of radiographic sacroiliitis over 2 years was 7.1% (95% CI 1.7% to 12.5%) in the entire cohort—figure 2. Exclusion of the 21 patients with complete ankylosis of the sacroiliac joints in the opinion of one or both readers (ie, patients who could not show further sacroiliitis progression) did not change the rates substantially: observed progression rate 13.8% (95% CI 9.6% to 19.4%), observed regression rate 5.3% (95% CI 2.9% to 9.5%), estimated ‘true’ progression rate 8.5% (95% CI 2.5% to 14.3%). Importantly, axial spondyloarthritis patients who showed progression of radiographic sacroiliitis according to the predefined criteria had significantly lower grades of sacroiliitis at baseline (mean grade 1.5±1.1 and 1.6±1.0 for the right and left sacroiliac joint, respectively) compared with the patients without progression (2.1±1.1 and 2.1±1.0, p=0.014 and 0.018 for the right and left sacroiliac joint, respectively).
After 2 years, 11 out of 95 patients (11.6%, 95% CI 6.6% to 19.6%) classified at baseline as non-radiographic axial spondyloarthritis fulfilled the radiological criterion of the modified New York criteria for AS. At the same time, after 2 years of follow-up, three out of 115 patients (2.6%, 95% CI 0.9% to 7.4%) initially classified as AS did not fulfil the modified New York criteria for AS any more.
Predictors of sacroiliitis progression
Univariate regression analysis allowed the identification of several predictor candidates for the progression of sacroiliitis, which were entered into the multivariate model. The strongest predictor of radiographic sacroiliitis progression over 2 years by at least one grade in the opinion of both readers in both non-radiographic axial spondyloarthritis and AS was an elevated C-reactive protein (CRP) level at baseline (OR 3.65, 95% CI 1.19 to 11.15, p=0.023 in the non-radiographic axial spondyloarthritis group and OR 5.08, 95% CI 1.02 to 25.38, p=0.048 in AS)—table 2. Multivariate logistic regression analysis confirmed the predictive value of elevated CRP in non-radiographic axial spondyloarthritis (OR 3.59, 95% CI 1.12 to 11.55, p=0.032, included variables CRP and sex) and AS (OR 5.62, 95% CI 1.06 to 29.94, p=0.043, included variables CRP, sex and duration of symptoms).
OR for progression of radiographic sacroiliitis by at least one grade in the opinion of both readers over 2 years in patients with axial spondyloarthritis, univariate analysis
Male gender was associated with a lower probability of radiographic progression of sacroiliitis in the non-radiographic spondyloarthritis group (OR 0.10, 95% CI 0.01 to 0.82, p=0.032 in the univariate and OR 0.11, 95% CI 0.01 to 0.85, p=0.035 in the multivariate model), whereas in the AS group male gender was rather a positive predictor of sacroiliitis progression after 2 years (trend, OR 3.15, 95% CI 0.63 to 15.73, p=0.162 in the univariate and OR 4.63, 95% CI 0.82 to 26.08, p=0.082 in the multivariate analysis). There was also a trend towards the association of a higher sacroiliitis progression rate with a longer disease duration in AS. Notably, no clear association between radiographic sacroiliitis progression and human leucocyte antigen B27 (HLA-B27) status was found. Factors such as age, Bath Ankylosing Spondylitis Disease Activity Index and Bath Ankylosing Spondylitis Functional Index values, duration of symptoms, presence of peripheral arthritis, enthesitis, psoriasis, family history of spondyloarthritis, presence of inflammatory back pain, therapy with non-steroidal anti-inflammatory drugs, disease-modifying antirheumatic drugs and smoking status showed no clear association with the progression of radiographic sacroiliitis. Due to the low numbers of patients treated with systemic steroids and tumour necrosis factor alpha blockers, as well as patients with a history of inflammatory bowel disease, these factors were not included in the predictor analysis.
Importantly, the elevated level of CRP was also a significant predictor of progression of non-radiographic axial spondyloarthritis to AS fulfilling the modified New York criteria (OR 4.10, 95% CI 1.13 to 14.95, p=0.032 in the univariate and OR 4.74, 95% CI 1.23 to 18.25, p=0.024 in the multivariate model, included variables CRP and definite radiographic sacroiliitis at baseline). The presence of definite structural damage at baseline (sacroiliitis grade 2 unilaterally in the opinion of both readers) also showed an association with progression to AS, although the level of statistical significance was not reached (OR 3.00, 95% CI 0.84 to 10.77, p=0.092, univariate analysis and OR 3.55, 95% CI 0.92 to 13.67, p=0.065 in the multivariate analysis).
Discussion
In the current report we attempted to assess the rate of radiographic sacroiliitis progression and predictors of progression in patients with axial spondyloarthritis and a short duration of the disease. To our knowledge there have been no studies so far investigating the rate of sacroiliitis progression in patients with AS and non-radiographic axial spondyloarthritis. Previous studies concentrated on the progression from non-radiographic axial spondyloarthritis to AS, which is, of course, clinically relevant but captures only a relatively narrow time frame when transition from a non-radiographic to a radiographic stage, according to the definition, occurs. As a result, no predictors of radiographic sacroiliitis progression have been investigated so far.
Sampario-Barros et al6 reported that 10% of the patients progressed from undifferentiated spondyloarthritis to AS over 2 years and 24.3% of the patents progressed over 5–10 years.7 These data are consistent with the earlier report by Schattenkirchner and Krüger8 in which a 25% progression rate of undifferentiated spondyloarthritis to AS was observed after a period from 2 to 6 years. Similarly, 59% of the patients with no definite diagnosis of AS at baseline developed definite AS after 10 years of follow-up in the study by Mau et al.11 Therefore, based on these studies the rate of progression from non-radiographic axial spondyloarthritis to AS can be estimated as approximately 10% over 2 years, which was also confirmed by the 11.6% progression rate found in our study. Somewhat higher rates of progressions were found in the study by Sany et al9 (30% of the patients progressed to AS over the period from 1 to 4 years) and in the study by Huerta-Sil et al10 (42% of the patients with undifferentiated spondyloarthritis after 3 years fulfilled the modified New York criteria for AS).
The ‘true’ radiographic sacroiliitis progression rate (worsening by at least one grade in the opinion of both readers) over 2 years was estimated as 4.4% for AS patients and 10.5% for non-radiographic axial spondyloarthritis patients. Although the progression rate in non-radiographic axial spondyloarthritis was more than twice as high as in AS, this difference did not reach statistical significance. The observed difference might be due to rather qualitative than really quantitative differences between the grades. Like AS in general is determined by an overlap between inflammation and new bone formation, the scoring used for the sacroiliac joints is a mixture of erosive damage and new bone formation, with grade 2 reflecting rather erosions, grade 4 ankylosis and grade 3 both. Also, the currently mostly used scoring method for the spine, the modified Stoke Ankylosing Spondylitis Spinal Score, scores erosions of the vertebral bodies with grade 1 and syndesmophytes with grades 2 or 3. Therefore, it is difficult to split radiographic structural damage into erosive and ankylosing damage, especially if the sacroiliac joints are scored. The reading of pelvic x-rays and the recognition of sacroiliitis is generally difficult that is related, first of all, to the anatomical complexity of the sacroiliac joints and the suboptimal visualisation with standard x-rays. van Tubergen et al15 showed that both radiologists and rheumatologists demonstrate only modest sensitivity and specificity for sacroiliitis detection and sizeable intraobserver variation. Moreover, neither individual training nor workshops were able to improve performance in this study. General technical difficulties in sacroiliitis assessment are reflected in our study by a moderate level of agreement between the readers regarding the presence of sacroiliitis, and this is the most probable reason for the relatively high regression rates of radiographic sacroiliitis over 2 years. Therefore we chose a blinded approach of x-ray reading by two independent readers, which was not the case in the above-mentioned studies,6,–,11 and the conservative method of ‘true’ radiographic progression estimation as a difference between the observed progression and the regression rates in the opinion of both readers.
When we analysed predictors of radiographic sacroiliitis progression the only one strong predictor of such progression in patients with non-radiographic axial spondyloarthritis and AS was an increased level of CRP with an OR from 3.7 to 5.6. Elevated CRP was also found to be associated with the presence of radiographic sacroiliitis in our previous report concerning baseline characteristics of patients in the GESPIC.12 These data show the important role of the high inflammatory activity for progression of sacroiliitis and for transition from the non-radiographic to the radiographic stage of axial spondyloarthritis. An association between the CRP level and sacroiliitis progression was not reported in previous studies, because information about the CRP level was not available,6,–,9 11 with the exception of the study by Huerta-Sil et al,10 in which elevated CRP and erythrocyte sedimentation rate, whatever was available, were analysed together, but showed only a trend for the association with the progression from undifferentiated spondyloarthritis to AS. CRP has played only a limited role in the diagnosis and management of AS so far. This can partly be explained by the mixture of inflammation and new bone formation, which can be both, dependent on the stage of the disease, responsible for manifestations, but also because osteitis might not be as closely linked to systemic serological parameters of inflammation as synovitis.16 Indeed, only up to 60% of patients have been reported to have an elevated CRP despite high disease activity, as judged by the treating physician.17 Nonetheless, elevated CRP has been found recently to be a predictor of a good response to tumour necrosis factor blockade,18,–,20 CRP has been incorporated in a new ankylosing spondylitis disease activity score,21 and CRP is being used as one among several other spondyloarthritis-typical parameters in the assessment of spondyloarthritis international society classification criteria for axial spondyloarthritis.4 The data presented here add further evidence that an elevated CRP, reflecting systemic inflammation, is a relevant feature in AS and axial spondyloarthritis.
Sampario-Barros et al6 found an association of alternating buttock pain and HLA-B27 status with the progression from undifferentiated to differentiated spondyloarthritis. Long-term follow-up of the same cohort revealed additional factors associated with the progression to AS: ethnicity, inflammatory low back pain, ankle involvement, grade I sacroiliitis at the beginning of the study and the use of sulfasalazine.7 In the study by Huerta-Sil et al10 low-grade sacroiliitis and the presence of uveitis were associated with the progression of undifferentiated spondyloarthritis to AS. In our cohort we did not find a significant association between radiographic sacroiliitis progression and HLA-B27 status, history or presence of uveitis, history of arthritis as well as with alternating buttock pain or any other features of inflammatory back pain.
Somewhat surprising was the diverse predictive role of male gender in patients with non-radiographic axial spondyloarthritis (negative) and AS (positive). We suggest that factors such as a relatively small sample size could play a role. We also found a trend towards an association of unilateral grade 2 radiographic sacroiliitis at baseline with the progression from non-radiographic axial spondyloarthritis to definite AS. This suggests that patients with existing definite yet minor structural damage might be at higher risk of further progression.
Radiographic sacroiliitis has been used in the past mostly for diagnostic purposes while the assessment of ankylosis of the spine has been established as an important long-term outcome parameter in AS because of its correlation with spinal mobility and function.22 23 Whether advanced sacroiliitis with, for example, fused joints does have any impact on the mobility and function of the axial skeleton has not been well investigated until now. However, because axial spondyloarthritis normally starts in the sacroiliac joints and sacroiliitis continues over time while an affliction of the spine is found only in a subgroup of patients,12 24 radiographic progression of the sacroiliac joint might reflect the progress of the disease better and might be more sensitive to change. Nonetheless, because of the slow rate of progression (∼10% of the patients over 2 years) a large sample size would be necessary to show any treatment effect on radiographic sacroiliitis. It has to be shown whether chronic sacroiliac joint changes as depictured by MRI are more sensitive to change than x-ray changes.
Acknowledgments
The authors would like to thank Beate Buss and Petra Tietz for monitoring the cohort, Anja Weiss and Martina Niewerth for data management support, Janis Vahldiek and Georg Heine for x-ray images handling and for the development of the image scoring interface. The authors would further like to thank the following rheumatologists for inclusion and monitoring of their patients: H Brandt, J Brandt, G-R Burmester, H Deister, E Edelmann, J Emmerich, M Enderlein, A Gauliard, E Gromnica-Ihle, F Heldmann, S Hermann, U von Hinüber, Ü Hübner, K Karberg, C Kedor, H Nüsslein, R Pelle-Lohfink, D Pick, G Reichmuth, M Rihl, S Schnarr, U Schneider, I-H Song, I Spiller, U Syrbe, V Walz, S Wassenberg, H M Wisseler and S Zinke.
References
Footnotes
-
Funding As part of the German competence network in rheumatology (Kompetenznetz Rheuma), GESPIC has been financially supported by the German Ministry for Education and Research (Bundesministerium für Bildung und Forschung–BMBF), grant number: FKZ01G19946. As funding by BMBF was reduced according to schedule in 2005, complementary financial support in equal parts has been obtained since 2005 from Amgen, Centocor, Schering-Plough and Wyeth, and since 2006 also from Abbott Immunology.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study protocol was approved by the central ethical committee of the coordinating centre (Charité–Campus Benjamin Franklin, Berlin, Germany) and by all local ethical committees of the participating centres.
-
Provenance and peer review Not commissioned; externally peer reviewed.