Article Text

Abstract
Objective To investigate whether an intensive early rheumatoid arthritis (RA) treat-to-target (T2T) strategy could be improved through the use of musculoskeletal ultrasound (MSUS) assessment of disease activity.
Methods 111 newly diagnosed patients with RA or undifferentiated arthritis (symptom duration <1 year) were randomised to strategies that aimed to attain either DAS28-erythrocyte sedimentation rate (ESR)<3.2 (control) or a total power Doppler joint count≤1 during a combined DAS28-ESR/MSUS assessment (intervention). MSUS examination was indicated if: DAS28-ESR<3.2 or DAS28-ESR≥3.2 with two swollen joints. Step-up disease-modifying antirheumatic drug (DMARD) escalation was standardised: methotrexate monotherapy, triple therapy and then etanercept/triple therapy. American College of Rheumatology (ACR) core-set variables were assessed 3 monthly by a metrologist blinded to group allocation. MRI of dominant hand and wrist, and plain radiographs of hands and feet were undertaken at baseline and 18 months for grading by two readers using the Outcome Measures in Rheumatology (OMERACT) Rheumatoid Arthritis MRI Scoring System (RAMRIS) and van der Heijde/Sharp Score, respectively. The coprimary outcomes were mean change from baseline of DAS44 and RAMRIS erosion score.
Results Groups were matched for baseline clinical, demographic and radiographic features. The intervention group received more intensive DMARD therapy. Both groups demonstrated significant improvements in DAS44 (mean change: control −2.58, intervention −2.69; 95% CI difference between groups −0.70 to 0.48; p=0.72). There were no significant between-group differences for any ACR core-set variables, except DAS44 remission after 18 months (control 43%, intervention 66%; p=0.03). There was minimal progression of MRI and radiographic erosions and no difference in imaging outcomes or serious adverse event rates.
Conclusions In early RA, a MSUS-driven T2T strategy led to more intensive treatment, but was not associated with significantly better clinical or imaging outcomes than a DAS28-driven strategy.
Trial registration number NCT00920478.
- Early Rheumatoid Arthritis
- DAS28
- Ultrasonography
Statistics from Altmetric.com
Introduction
Early, intensive treatment of rheumatoid arthritis (RA) produces significant improvements in short-term to medium-term clinical, functional and imaging outcomes.1–6 Current treatment guidelines7 ,8 advocate the early use of disease-modifying antirheumatic drugs (DMARDs), singly or in combination, as part of ‘treat-to-target’ (T2T) strategies that aim to achieve low disease activity score (LDAS) or remission in all patients. T2T strategies use composite disease activity scores (eg, DAS44, DAS28, and Simplified Disease Activity Index (SDAI)), which incorporate tender and swollen joint counts, patient and physician assessments of disease activity and an acute phase reactant. However, these scores have limitations: patients with painful comorbidities can exhibit high scores that do not reflect active synovitis;9–11 conversely, many patients in remission exhibit subclinical synovitis that is associated with adverse outcomes. For example, during musculoskeletal ultrasound (MSUS) examination, the presence of intra-articular power Doppler (PD) signal predicts clinical flare12–14 and progressive radiographic damage.15
MSUS provides an attractive additional method for assessing RA disease activity since it avoids the use of ionising radiation, is more convenient than serial MRI assessments and allows multiple joint regions to be examined during a single consultation. We have previously reported that regular assessment by a limited MSUS joint set alters approximately 25% of all DAS28-based DMARD decisions.16 This could allow therapy to be more accurately tailored to patients' needs: those with subclinical synovitis could receive more intensive DMARD therapy to achieve ‘tighter’ overall disease control and potentially better outcomes. Conversely, symptomatic patients with elevated DAS28 assessments, but no MSUS evidence of synovitis, could avoid unnecessary treatment escalation. The Targeting Synovitis in Early Rheumatoid Arthritis (TaSER) study was designed to test the hypothesis that incorporating MSUS disease activity assessment into a T2T strategy would produce superior clinical and imaging outcomes compared with a strategy driven by a composite disease activity score.
Methods
The TaSER study was conducted within the Rheumatology Departments of three Scottish teaching hospitals between September 2009 and April 2013. The study protocol was approved by the NHS West of Scotland Research Ethics Committee and registered with ClinicalTrials.Gov (NCT00920478). All participants provided written informed consent.
Patients
Patients were eligible if they were aged over 18; had a new clinical diagnosis of RA or undifferentiated arthritis (UA) (defined as positive anti-cyclic citrillunated peptide (CCP) antibodies and ≥3 clinically swollen joints); had a symptom duration <12 months and active disease (DAS44>2.4). Patients were excluded if they had received more than 6 weeks DMARD therapy; had significant liver (transaminases >twice upper limit of normal) or renal (serum creatinine >200 μmol/L, estimated glomerular filtration rate (eGFR)<30 mL/min) dysfunction; significant cytopenias (white cell count <4×109/L, haemoglobin <10 g/dL, platelets <150×109/L); were pregnant or planning pregnancy or had a contraindication to aggressive DMARD escalation.
Design
The study was an open-label, randomised controlled trial with assessment of outcomes by investigators who were blind to group allocation and treatment. Patients were randomised 1:1 to a control group, in whom DMARD escalation decisions were based upon the DAS28-erythrocyte sedimentation rate (ESR) score, or an intervention group, in whom DMARD escalation decisions were based upon a combined DAS28-ESR and MSUS assessment. Randomisation used a telephone-administered interactive voice response system and was minimised using the patient's baseline DAS28 (<5.1/≥5.1), rheumatoid factor (positive/negative) and erosion (yes/no) status.
Treatment
Patients attended monthly review appointments for 18 months and were treated by the same rheumatologist (JD). Both groups followed the same step-up DMARD escalation sequence. DMARD doses were optimised to a target (or highest tolerated) dose. Treatment was escalated if the patient's disease activity target had not been reached, and ≥3 months had elapsed since the previous escalation.
Step 1: methotrexate (MTX) up to 20 mg/week (or sulfasalazine (SSZ) 40 mg/kg/day if MTX was contraindicated);
Step 2: MTX, SSZ and hydroxychloroquine (HCQ, <6.5 mg/kg/day up to maximum 400 mg/day)
Step 3: subcutaneous MTX (up to 25 mg/week), SSZ and HCQ;
Step 4: subcutaneous MTX, SSZ, HCQ and etanercept 50 mg/week.
Patients could receive up to 120 mg of triamcinolone acetonide during any consultation. Clinically swollen joints were actively injected if they had not been injected within the preceding 3 months, and/or bridging intramuscular steroid was administered if disease activity remained elevated within 3 months of DMARD escalation. MSUS was not used to guide intra-articular steroid injections. The use of other concomitant medications (including non-steroidal anti-inflammatory drugs and analgesics) was not restricted. Oral corticosteroids were limited to patients with either persistently active disease despite multiple triamcinolone injections or those with significant extra-articular disease.
Target
In the control group, the target was LDAS (DAS28-ESR<3.2).
In the intervention group, the target was total PD joint count ≤1. In patients with high disease activity (DAS28-ESR>5.1), or moderate disease activity (3.2<DAS28-ESR≤5.1) with ≥2 swollen joints, treatment was escalated without MSUS assessment. Treatment was not escalated in patients with moderate disease activity if the clinical swollen joint count and total MSUS PD joint count were both ≤1. Intervention group patients were informed whether treatment escalation decisions were based on DAS28 or MSUS findings.
MSUS assessments
Only patients allocated to the intervention group underwent MSUS assessment. MSUS assessment was undertaken when (i) DAS28 was >3.2 and <2 swollen joints or (ii) DAS28 was <3.2. All MSUS assessments were conducted by the same operator (JD) using a portable Voluson I, GE Healthcare machine, a 10–16 MHz linear probe (SP10-16RS) and standardised PD settings: frequency high (10 MHz, machine preset), pulse repetition frequency (PRF) 0.9 kHz, wall filter low (machine preset) and gain adjusted to just below the level at which Doppler artefact appeared beneath bone. The dorsal recesses of the index and middle proximal interphalangeal and metacarpophalangeal, radiocarpal, second and fifth metatarsophalangeal joints were examined bilaterally. Intra-articular PD activity was graded using a semiquantitative scale of 0–3.17 Active disease was defined as the presence of any PD in two joints.
Data collection
Clinical outcome measures were collected every 3 months by the same metrologist (AS) who was blinded to each patient's treatment strategy. The treating rheumatologist (JD) was unaware of these findings and they were not used to inform treatment decisions. The ACR core-set variables were collected:18 44 swollen joint count, Ritchie articular index, ESR, C reactive protein, patient global health 10 cm visual analogue score (VAS), pain 10 cm VAS, physician global disease activity Likert scale (0–5) and Health Assessment Questionnaire (HAQ). The EuroQoL5D-3L Index was also collected and converted to a single health utility index using standard UK value sets.19 The DAS28-ESR, commonly used in clinical practice, was used to inform treatment escalation decisions, whereas the original DAS44 (which includes clinical assessment of a larger joint set) was used as the outcome measure.
MRI scans of the dominant wrist and metacarpophalangeal joints and plain radiographs of hands and feet were undertaken at baseline and 18 months. All MRI scans were performed on a single machine (1.5T Siemens Avanto) using the following sequences: coronal T2-weighted fat-saturated and axial and coronal T1-weighted preintravenous and postintravenous gadolinium. MRI images were graded using the Outcome Measures in Rheumatology (OMERACT) Rheumatoid Arthritis MRI Scoring System (RAMRIS) atlas20 ,21 and plain radiographs were graded using the modified van der Heijde/Sharp Score (vdHSS).22 Both sets of images were graded independently, in chronological order, by two experienced readers who were blinded to the patient's treatment strategy. The means of the reader's scores for each component of the scoring system were used in the statistical analysis. Plain radiographs were scored by a commercial company (Imaging Rheumatology International).
Statistical analysis
The coprimary clinical and imaging outcomes were the mean change in DAS44 and RAMRIS erosions score between baseline and 18 months. All statistical analyses were conducted using SAS software, V.9.3 (SAS Institute). Between-group comparisons of normally distributed continuous variables were conducted using Student's t test and the Mann–Whitney U test was used for non-normally distributed variables. Paired continuous variables were compared using the Wilcoxon rank sum test and proportions within categorical groupings were compared using Fisher's exact test. Interobserver agreement for each component of the RAMRIS score and vdHSS was assessed using the intraclass correlation coefficient and the mean of the difference between each reader's findings. Each reader regraded 30 randomly selected sets of images and intrareader variability was estimated using the intraclass correlation coefficient. The smallest detectable change of RAMRIS and vdHSS erosion scores was calculated to differentiate true progression from measurement error.23
With coprimary outcomes, the type I and II error rates were effectively doubled. So, to obtain 90% power at 5% significance level, sample size calculations were based on 95% power and 2.5% significance level. Assuming a SD of the change in DAS44 of 0.7,24 50 patients needed to be recruited to each group to have sufficient power to detect a between-group difference in the mean change in DAS44 of 0.55, approximately half of a clinically significant change.25 Further, assuming a SD of the change in RAMRIS wrist erosions of 1.64,26 this sample size was powered to detect a between-group difference in the mean change of 1.29.
Results
Study cohort
One hundred and seventy patients with clinical diagnoses of UA or RA were screened for recruitment and 111 consented to participate (figure 1). The randomisation process assigned 57 patients to the control group and 54 patients to the intervention group. The control group contained a higher proportion of females (75% vs 61%), but no other differences in baseline characteristics were observed between the groups (table 1). Fifty-one control group and 50 intervention group patients completed the follow-up period and were included in the analysis of the primary outcomes. In total, five patients were lost to follow-up, four withdrew consent to participate and one was withdrawn after he developed an overlap syndrome with dermatomyositis that required aggressive immunosuppression. In the MSUS group, the median number of MSUS assessments performed per patient was 9 (IQR 6–10) and all patients in this group underwent at least one MSUS assessment.
Baseline characteristics of the study participants

Consort diagram—patient progress through study. RA, rheumatoid arthritis.
Treatment exposure
Patients in the intervention group received more intensive DMARD treatment than the control group (table 2). After 6 months, a higher proportion of the intervention group were prescribed combination therapy (67% vs 38%, p=0.003), and after 18 months a higher number had received etanercept (22% vs 10%, p=0.11). There were no significant differences in the mean doses of individual DMARDs at any time point, except at 18 months when oral MTX dose was higher in the control group (control 18 mg/week, intervention 15 mg/week, p=0.016). Both groups received similar total doses of triamcinolone acetonide (mean: control 288 mg (SD207), intervention 247 mg (SD171), p=0.25). Three control group and two intervention group patients received oral prednisolone. By study completion, three control group (mean dose 10 mg/day) and one intervention group patient (6.5 mg/day) remained on oral prednisolone.
Change between baseline and 18 months of ACR core-set variables and imaging outcomes, mean (SD)
Clinical outcomes
Both groups exhibited the greatest improvement in disease activity during the first 3 months of treatment. After 18 months, there was no significant between-group difference in the mean change in DAS44 (figure 2: control −2.58 (95% CI −3.02 to −2.14), intervention −2.69 (−3.09 to −2.29), p=0.72), nor the mean area under the curve DAS44 (control 40.9 (SD19.3), intervention 37.9 (SD17.7), p=0.42). Both groups exhibited significant improvements in all ACR core-set variables with no significant between-group differences for any variable (table 2).

Mean (95% CI) change in DAS44 from baseline.
There were no significant differences in the proportion of patients achieving ACR-Boolean remission,27 European League Against Rheumatism (EULAR) good, ACR 20, ACR 50 or ACR 70 responses (figure 3). After 18 months, a higher proportion of intervention group patients had achieved DAS44 remission (DAS44<1.6: control 43%, intervention 66%, p=0.03), but there were no differences in DAS44 remission rates at any other time point.

Percentage attainment of response criteria after 18 months follow-up: (A) ACR 20/50/70 and EULAR good responders; (B) DAS44 remission (DAS44≤1.6) and ACR-EULAR-Boolean remission. ACR, American College of Rheumatology; DAS44, 44 joint disease activity score; EULAR, European League Against Rheumatism.
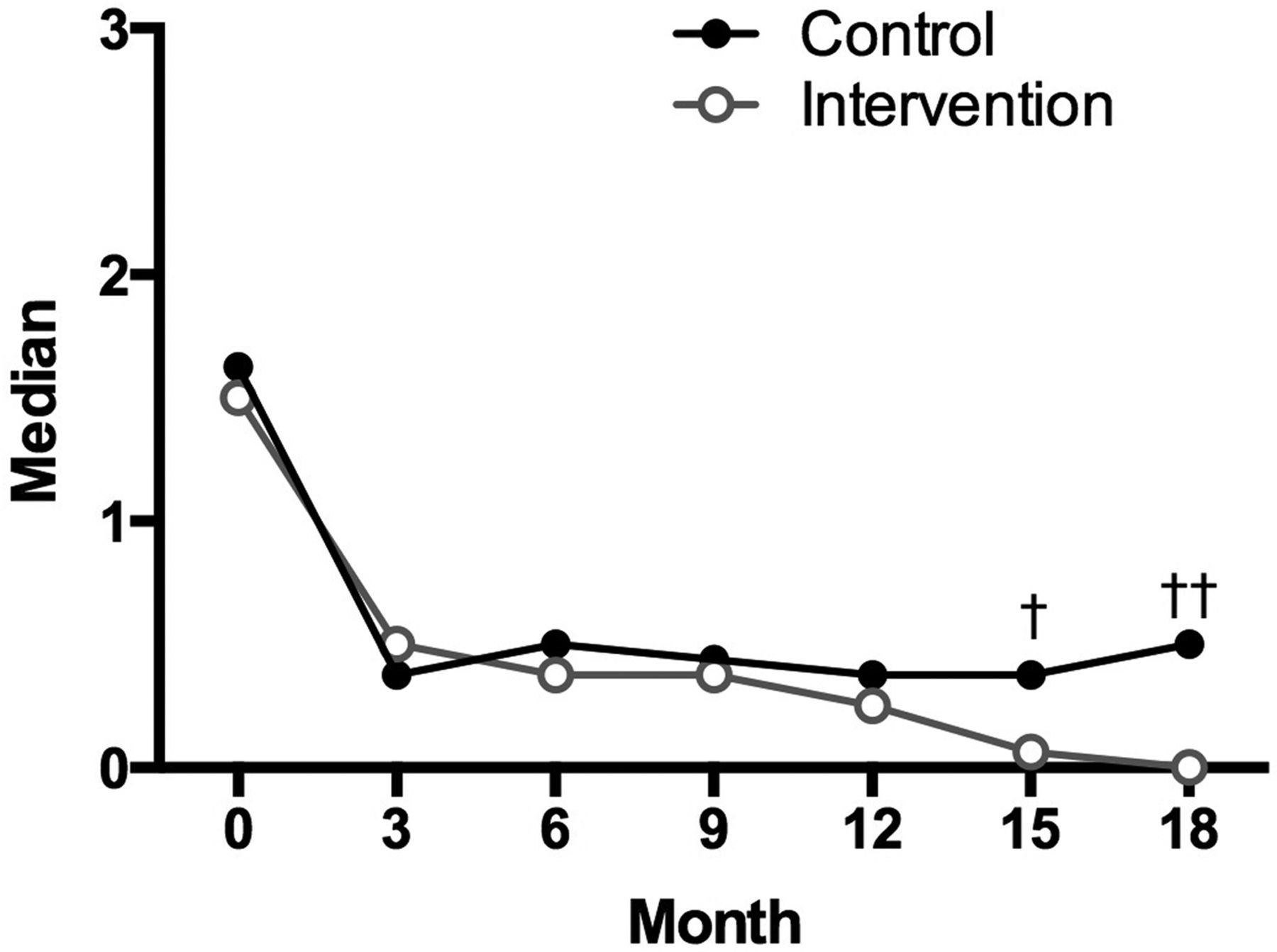
After 15 and 18 months, the intervention group exhibited numerically lower HAQ scores (figure 4: median HAQ: 0.38 vs 0.06, p=0.31 at 15 months; 0.5 vs 0.0, p=0.06 at 18 months). Health utility index values improved significantly in both groups, with no significant between-group differences at any time point, nor the number of quality-adjusted life years gained over the follow-up period (mean (95% CI): control 0.97 (0.84 to 1.10), intervention 1.02 (0.90 to 1.14), p=0.57).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Median Health Assessment Questionnaire (HAQ). (†p=0.31, ††p=0.06).
Imaging outcomes
There was good-to-excellent intrareader and interreader agreement for each component of the RAMRIS score and vdHSS (see online supplementary tables S1 and S2). Baseline values for individual components of the RAMRIS and vdHSS were similar (table 1). Both groups showed small increases in the RAMRIS erosion score and significant decreases in the synovitis and osteitis scores. Similarly, on plain radiographs, both groups showed very small increases in erosion, joint space narrowing and total vdHSS (table 2). However, for each RAMRIS and vdHSS component, there was no significant between-group difference in either the change from baseline (table 2) or the value at each time point (see online supplementary tables S3 and S4). Numerically, fewer patients in the intervention group had changes in RAMRIS erosion (16 vs 24%, p=0.39) and vdHSS erosion (11 vs 23%, p=0.17) scores that exceeded the smallest detectable change (RAMRIS erosions smallest detectable change (SDC)=2.5, vdHSS erosion SDC=1.3).
Supplementary appendix
Adverse events
Forty-eight control group patients (89%) and 46 intervention group patients (81%) reported at least one adverse event. Both groups reported similar numbers of adverse events (control 109, intervention 100) and mean number of events per patient (2.3 vs 2.2, p=0.72). The most commonly reported adverse events were abnormal liver function tests (control 19, intervention 15), nausea (18 vs 14), lower respiratory tract infection (15 vs 18), urinary tract infection (6 vs 3), rash (3 vs 3) and leucopoenia (2 vs 6). One control group patient was diagnosed with small lymphocytic lymphoma and one intervention group patient developed Waldenström's macroglobulinemia. Neither diagnosis was thought to be related to participation in the study.
A higher number of serious adverse events (including elective admissions) was observed in the intervention group (8 vs 19). There were no deaths in either group and one serious infective episode (pneumonia) in the intervention group required emergency admission for intravenous antibiotics. Two control group patients and four intervention group patients underwent elective orthopaedic admissions. One intervention group patient underwent three hospital admissions with abdominal pain and nausea (chronic symptoms that preceded participation in the study) and another intervention group patient underwent four admissions for treatment of a pre-existing cardiac condition. All of these episodes were classified as serious adverse events, but were not thought to be related to participation in the study. One control group patient underwent emergency admission for assessment of an exudative pleural effusion that was considered to be an extra-articular manifestation of RA.
Discussion
This is the first randomised controlled trial to evaluate the impact of integrating MSUS assessments into a T2T strategy of newly diagnosed RA/UA. The presence of MSUS synovitis, and intra-articular PD signal in particular, is associated with active RA and radiographic progression; consequently, sonographic remission has been proposed as a potential disease activity target.28 Similarly, composite disease activity scores are known to have limited sensitivity and specificity and may not wholly represent the true disease activity state. This study demonstrates that regular assessment of RA disease activity by MSUS, aiming for MSUS remission, leads to a greater intensity of DMARD therapy. However, while this was not associated with a higher rate of adverse events, it was also not associated with superior clinical, functional, health-related quality of life or imaging outcomes.
Both groups experienced an excellent overall response to treatment that may have limited the power of the study to detect significant between-group differences. However, the 95% CIs for the difference in the primary clinical outcome (95% CI mean improvement in DAS44: −0.70 to 0.48) indicate that clinically significant differences in outcome are unlikely. Over the first 12 months of the study, there were no differences in any of the clinical outcomes. After 15 months, HAQ scores were numerically lower in the intervention group, and after 18 months, a significantly higher proportion of patients had attained DAS44 (but not ACR/EULAR-Boolean) remission. These differences should not be overinterpreted. Given the large number of comparisons, a small number of statistically significant results might be expected by chance. However, it is also possible that improved outcomes might only become apparent in the intervention group over a longer follow-up period, perhaps as the rate of etanercept use rises.
It is notable that the rate of damage progression in this study was considerably lower than observed in the TICORA study: median change total vdHSS: 4.5 (IQR 1–9.9) compared with either group in this study (control 0.5 (IQR 0–1.5), intervention 0 (IQR 0–1.0)). Patients in the TICORA study presented with higher DAS44 scores (mean 4.76 (SD 0.94)), higher rates of smoking (46%) and longer symptom durations (mean 20 months (SD16)), all of which could contribute to a higher overall risk of radiographic progression. While there was no significant difference observed in the primary imaging outcome, there were numerically fewer intervention group patients who exhibited progression in RAMRIS and vdHSS erosion scores that exceeded the SDC. It is possible that with a larger cohort and with longer follow-up that these observations might become statistically significant. However, it has previously been shown that there is very little radiographic progression in patients who attain stringent remission criteria27 ,29–32 suggesting that any differences that might be observed between those in clinical and sonographic remission are unlikely to be clinically relevant. The excess of reported serious adverse events (SAEs) in the intervention group was not statistically significant, and is unlikely to be of clinical significance either—the majority of SAEs were not thought to be adverse reactions to treatment.
The routine, systematic use of MSUS assessment in all patients with DAS28-LDAS resulted in a large number of negative assessments that did not influence management.16 This is time consuming and may not be practical in busy clinics. Several recent studies have proposed limited MSUS joint sets33 ,34 that require shorter examination times, perform as well as extended joint sets34–37 and are responsive to changes in disease activity.34 ,38 Even now, there is no consensus about which is the most appropriate set of joints to examine, nor is there an accepted definition of what level of MSUS findings constitutes ‘active’ RA. The MSUS joint set used by this study was designed pragmatically by combining the common peripheral joints of two previously proposed sets.33 ,34 Any benefit from using a more extensive joint set, or more detailed examination (eg, to include tendons) would need to be offset against the additional time and expertise required. The observation that the joints of healthy volunteers may also display PD signal39 ,40 argued against a very stringent MSUS treatment target. Requiring at least two joints to exhibit PD signal was thus a pragmatic decision aimed at avoiding potentially unnecessary treatment escalation, cognizant that it might have excluded some patients from reaching true MSUS remission. Furthermore, for this study, PRF was set at 0.9 kHz for all assessments; using a lower PRF settings would have increased the sensitivity for the detection of PD signal at the risk of increased artefact, but this would be unlikely to affect the conclusions of the study.
Since the study was undertaken, there have been significant advances in ultrasound technology leading to increased sensitivity for the detection of grey scale and PD abnormalities. The significance of these abnormalities is not certain—recent studies have suggested that modern machines may identify grey scale synovitis in healthy individuals,41 although this is not usually associated with PD signal,42 and PD abnormalities of grade ≥2 are rare.43 Given the favourable outcomes achieved in the control group, it is arguable whether the use of improved technology would alter any of the study's conclusions.
In both groups, DAS44 improved most quickly between the baseline and month 3 visits. Therefore, the intervention that had the greatest impact on disease activity was commencement of treatment and not the method used to monitor disease activity. This study used a standardised DMARD escalation protocol that was similar to other early RA strategy studies.1 ,5 ,44–47 There are some conflicting data about the relative merits of initial combination and step-up strategies: some studies suggest they are equally effective,45 ,46 whereas others suggest modest advantages associated with combination therapy.5 ,48 The Swedish Farmacotherapy (SWEFOT) study suggested that a substantial minority (approximately 30%) will achieve LDAS with MTX monotherapy47 and the Rheumatoid Arthritis: Comparison of Active Therapies (RECAT) study demonstrated that, after MTX monotherapy failure, the sequence of progression from triple to biological therapy does not significantly affect clinical or radiographic outcomes.45 The results of the TaSER study are in line with these findings; very intensive MSUS-driven DMARD escalation did not produce significantly better clinical or imaging outcomes than an intensive DAS28-ESR-driven strategy.
Previous studies have suggested that MSUS evidence of subclinical disease (especially PD signal) is not benign, being predictive of acute flare,12–14 radiographic damage progression15 and failure to successfully taper biological therapy.49 It is possible that treating to eradicate imaging evidence of subclinical disease will achieve a more stable disease state, which eventually becomes associated with more favourable long-term outcomes, than treating to attain LDAS. However, given that both groups exhibited an excellent treatment response, it may not be possible (or feasible) to use current disease activity measures to demonstrate subtle between-group differences in response without powering studies to examine markedly smaller effect sizes over much longer follow-up periods.
This study confirms that patients with newly diagnosed early RA/UA treated according to an intensive T2T strategy have excellent short-term clinical, functional, health-related quality of life and imaging outcomes. There will undoubtedly continue to be a major role for the use of MSUS in the management of patients with RA, including assessment of disease activity, and informing treatment decisions when disease activity status is not clinically apparent. However, the results of this study do not currently support the routine use of MSUS assessment as part of an enhanced T2T strategy in newly diagnosed inflammatory arthritis.
Acknowledgments
The authors sincerely thank the staff and patients from the Departments of Rheumatology at Gartnavel General Hospital, Glasgow Royal Infirmary, Inverclyde Royal Hospital and Stobhill Hospital, Glasgow for their contribution to this study.
References
Supplementary materials
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Tore K Kvien
Twitter Follow James Dale at @jimedale
Contributors JD, IBM and DP conceived the study. JD, PC, AMC and DP designed the study. AS, JF, MS and DvdH were responsible for the collection of outcome variables. JD, RZ, DP and AM conducted the statistical analysis. JD drafted the manuscript and all authors helped to finalise the manuscript.
Funding This study was jointly funded by a Clinical Academic Fellowship from the Chief Scientist's Office, Scottish Executive and an Investigator Initiated project grant from Pfizer UK. Neither funder had any role in the design, performance, analysis, interpretation or reporting of the study.
Competing interests JD reports grants from Chief Scientist's Office, Scottish Government, grants from Pfizer, during the conduct of the study; personal fees and non-financial support from Abbvie, personal fees from Janssen, personal fees from Pfizer, outside the submitted work; AS reports grants from Chief Scientist's Office, Scottish Government, grants from Pfizer, during the conduct of the study; RZ has nothing to disclose; DP reports grants from Pfizer and Chief Scientists Office, Scottish Government, during the conduct of the study; JF has nothing to disclose; MS reports that he is an Executive Member of the British Society of Radiologists; PGC reports grants and personal fees from BMS, personal fees from Abbvie, personal fees from Janssen, personal fees from Pfizer, personal fees from Roche, personal fees from Novartis, personal fees from Merck, outside the submitted work; DvdH reports other from University of Glasgow, during the conduct of the study; personal fees from AbbVie, personal fees from Amgen, personal fees from Astellas, personal fees from AstraZeneca, personal fees from BMS, personal fees from Celgene, personal fees from Daiichi, personal fees from Eli-Lilly, personal fees from Galapagos, personal fees from Merck, personal fees from Novartis, personal fees from Pfizer, personal fees from Roche, personal fees from Sanofi-Aventis, personal fees from UCB, other from Imaging Rheumatology BV, outside the submitted work; AMC reports grants from Chief Scientists Office, Scottish Government, grants from Pfizer, during the conduct of the study; IBM reports grants and personal fees from Pfizer, during the conduct of the study; grants and personal fees from UCB, grants and personal fees from AbbVie, grants and personal fees from BMS, grants and personal fees from MSD, grants and personal fees from Roche, outside the submitted work; DP reports grants from Pfizer, grants from Chief Scientists Office, Scottish Government, during the conduct of the study; grants and personal fees from Pfizer, outside the submitted work.
Ethics approval West of Scotland Research Ethics Service. All patients provided written, informed consent to participate.
Provenance and peer review Not commissioned; externally peer reviewed.