Article Text

Abstract
Background and objectives Instruments for measuring disease activity in psoriatic arthritis (PsA) are not yet firmly established, and most of the currently employed ones have been derived for rheumatoid arthritis. Some of these instruments are based on 28 joint counts, which do not capture joints frequently affected in PsA. Therefore, the reliability and validity of DAREA (for ‘Disease Activity index for REactive Arthritis’), which was originally developed for reactive arthritis and employs a 66/68 joint count, was tested in patients with PsA.
Methods Trial data from the Infliximab Multinational Psoriatic Arthritis Controlled Trial were analysed. Results were then independently validated using an observational data set. DAREA was compared to other composite indices regarding correlations with core set variables, sensitivity to change and criterion validity.
Results Good correlation of the DAREA with single items of disease activity, other composite scores (r=0.6−0.9) and physical function (Health Assessment Questionnaire; r=0.5) was found. Likewise, DAREA was at least as sensitive to change as the other indices and more so in patients with distal interphalangeal joint involvement. Additionally, DAREA correlated well with radiographic changes.
Conclusion The analyses of this study provide evidence of the utility and validity of the DAREA for PsA disease activity assessment. A second name should therefore be assigned to this score: DAPSA (for ‘Disease Activity index for PSoriatic Arthritis’).
Statistics from Altmetric.com
Introduction
Psoriatic arthritis (PsA) is an inflammatory joint disease that, aside from its association with psoriasis, may also involve the spine and entheses.1 2 Additionally, peripheral joint involvement is highly variable when compared to other arthritides.3 This heterogeneity and breadth of clinical features make it hard to account for the whole spectrum of disease manifestations using a single instrument. Separate assessment of these manifestations may be preferable; indeed, measures for several characteristics have been validated and successfully applied in clinical trials, such as for skin,4 spinal,5 6 entheseal and nail involvement,2 6,–,8 and dactylitis.6 9
It is well established that using composite scores is superior to the evaluation of individual variables by capturing several items and minimising between-patient and within-patient variability over time.10 11 Indeed, several such measures for peripheral arthritis activity have been developed and applied in recent years. However, an unequivocally reliable instrument for this aspect of PsA has not been ultimately provided. An instrument that came to be called the PsA Response Criteria (PsARC), which includes 66/68 tender and swollen joint counts (TJC, SJC) and evaluator and patient global assessments (EGA, PtGA),12 was developed for a single clinical trial. Like the American College of Rheumatology (ACR) response criteria for rheumatoid arthritis (RA),13 the PsARC does not allow quantification of disease activity; rather, it determines relative changes from baseline. Moreover, the PsARC has not been formally validated; in the initial trial for which it was created, it failed to show differences between treatments.12
Another instrument commonly employed in PsA is the Disease Activity Score using 28 joint counts (DAS28) that was originally developed for patients with RA.14 Similar to the ACR response criteria, it has been shown to effectively assess therapeutic efficacy in PsA6 15,–,17 and when compared with other criteria, including the PsARC, DAS28 was the most responsive and discriminating instrument.17 However, the 28 joint count used in the DAS28 does not include joints commonly involved in patients with PsA, such as distal interphalangeal (DIP) joints of the hand and joints of the ankle and foot. Therefore it may miss important elements of disease activity in many patients with PsA.1
In a recently performed principal component analysis (PCA), three components with a total of five items were revealed to best reflect disease activity of PsA.18 These components were (1) patient-reported outcomes, displayed most strongly by PtGA and pain assessments; (2) joint involvement, signified best by the 66 SJC and 68 TJC; and (3) acute phase response, represented best by C reactive protein (CRP). Interestingly, exactly these five components comprise a disease activity score which had been developed several years ago for the assessment of reactive arthritis (DAREA, for ‘Disease Activity index for REactive Arthritis’).19 For these reasons, we assessed whether the DAREA might be a valid instrument also in PsA, assuming that REA and PsA are seronegative spondylarthropathies, often affecting the lower extremities and also DIPs. The DAREA has been developed and validated for REA,19 constituting the background for a subsequent modification for RA assessment,20 the simplified and the clinical disease activity indices (SDAI, CDAI). It is based on a simple numerical summation of five variables of disease activity: TJC and SJC, using the 66/68 assessment, PtGA patient pain assessment, and CRP in mg/dl.20
Four of these variables (TJC, SJC, PtGA and pain) were also ranked as key outcomes in Outcome Measures in Rheumatoid Arthritis Clinical Trials surveys.6 21 Acute phase reactants, the fifth component, attained two-thirds of the votes, much more than EGA,6 21 which is not included in DAREA, and received only 51% of the votes in that survey.
In the present study, the DAREA was evaluated in PsA using data from a clinical trial that compared the efficacy of infliximab with placebo. Results were then validated using data from an observational cohort of outpatients with PsA.
Patients and methods
Data sources
We obtained an 80% random data sample from the Infliximab Multinational Psoriatic Arthritis Controlled Trial (IMPACT 2),16 in which patients received infliximab or placebo and were studied for 54 weeks. To be enrolled, patients had to have active PsA, as defined by: SJC≥5, TJC≥5 and a CRP≥15 mg/l or morning stiffness of ≥45 min. For the present analyses, baseline, week 14 and week 54 disease activity assessments of completers were used (n=180). The 14-week point was chosen because many patients, mostly on placebo, received rescue infliximab treatment after that time if they had been responding insufficiently. Changes in radiographic scores from baseline to 54 weeks were also evaluated. All analyses were on a randomised group basis.
The second population studied comprised a ‘real life’ observational cohort of 99 patients with PsA followed at the outpatient clinic at Hietzing Hospital after initiation of a new disease-modifying antirheumatic drug (DMARD) treatment for active joint involvement.
Appropriate ethical committee approvals were obtained.
Study variables
The variables derived from the IMPACT 2 cohort included joint counts on a 66/68 as well as on a 28 joint scale (SJC, TJC), PtGA and EGA by VAS, patient pain assessment (pain; VAS), erythrocyte sedimentation rate (ESR; mm/h), CRP (mg/dl), physical function domain of the Medical Outcomes Study Short-Form 36 (SF-36 pf) and radiographic data (assessed by the PsA-modified van der Heijde–Sharp scoring method, including hand DIPs22).
For the observational cohort we obtained the same variables as enumerated above, with the exception of x-ray changes and SF-36 scoring, while instead the Health Assessment Questionnaire (HAQ) disability index was evaluated.
Based on these individual measures, we calculated the following composite indices:
DAREA=SJC66+TJC68+PtGA+pain+CRP19;
SDAI=SJC28+TJC28+PtGA+EGA+CRP20;
CDAI=SJC28+TJC28+PtGA+EGA20 23;
DAS28 using CRP
(DAS28CRP)=0.56×√(TJC28)+0.28×√(SJC28)+0.36×lognat (CRP+1)+0.014×GH+0.9624 25;
DAS28 using ESR
(DAS28ESR)=0.56×√(TJC28)+0.28×√(SJC28)+0.70×lognat(ESR)+ 0.014×GH.14
In the SDAI, CDAI and DAREA as applied here, the VAS for PtGA, pain and EGA were used in cm and CRP in mg/dl; in the DAS28 the PtGA was employed as global health (GH) and the VAS in mm.
Statistical analyses
We used the baseline data of the IMPACT 2 study to explore, cross-sectionally, correlations between individual disease activity items and the described indices (item–score correlation). Thereafter, the focus was the comparative assessment of the indices' longitudinal validity, looking at their sensitivity to change and ability to discriminate active drug from placebo, as well as their criterion validity with regard to radiographic progression.
Sensitivity to change was assessed by effect sizes (ESs) after year 1 of treatment, determined as follows: ES=(meanat 1 year−meanat baseline)/SDat baseline.
Ability to discriminate was investigated using t tests on the change of scores and comparing the t score and associated p values. To ascertain criterion validity, we performed Spearman correlation of changes in DAREA scores during follow-up with radiographic progression during the first year (progression from baseline to week 54). Additionally, we applied receiver operating characteristic curves to test the predictive value of DAREA changes attained from baseline to week 54 for 1-year radiographic progression.
Validation and generalisability
To confirm and further validate findings of the primary trial data analysis, we studied patients with PsA who started a new DMARD treatment at our outpatient clinic (n=99). Thus, the validation set stemmed from a different source and also expanded the data to a real life cohort of patients not specifically selected to fulfil clinical trial inclusion and exclusion criteria.
We performed corresponding sensitivity to change analyses with the observational data set; the time point for the analyses of sensitivity to change was the subsequent clinical visit (2.8±3.5 months after baseline). Analyses on discrimination and criterion validity could not be performed in this group given the lack of a placebo arm and of radiographic data.
Analyses were performed on SPSS V.15.0 (SPSS, Chicago, Illinois, USA) or the SAS package, V. 9.1.3 (SAS, Cary, North Carolina, USA); p<0.05 was regarded significant.
Results
Patients
The demographic and baseline clinical characteristics of the two populations are shown in tables 1–3. While in IMPACT 2 patients were subjected to either infliximab (n=89) or placebo (n=91), patients in the observational cohort started the following DMARDs at the baseline visit: methotrexate (n=66), anti-TNF (n=21), sulfasalazine (n=12). In this section, we will initially present the analyses of the IMPACT 2 data, followed by the results of the observational cohort.
Demographic and baseline characteristics of patients enrolled in the IMPACT 2 study and of the observational patient cohort
Baseline, end point and change (improvement) values of individual variables and composite measures in the infliximab group of the IMPACT 2 study
Baseline and follow-up values (mean±SD) of individual variables and composite measures of 99 patients in the observational data set (average interval between visits: 2.8±3.5 months)
Item score correlation for DAREA and other indices
In the IMPACT 2 baseline data, significant correlations of the assessed composite indices with individual variables of disease activity were seen. This was true for those single variables that were part of the scores and for variables not included. For instance, relatively weak (r=0.30) but significant (p<0.001) correlation was found between EGA and DAREA (table 4), but this was similar to the correlations observed for some variables included in the index, such as pain and PtGA. Of notice, weak correlations of EGA were also found with other composite scores used in PsA, which (in contrast to DAREA) include EGA in their formulae (SDAI: r=0.41, CDAI: r=0.34; p<0.001 for all). For DAS28 which does not include EGA, the correlation coefficient was similar: r=0.33. Interestingly, in patients with DIP involvement, the correlation of EGA and DAREA was higher than in the entire cohort (r=0.54, p<0.001; table 4); even though DIPs are not included in the 28 joint counts, also the correlations between EGA and the other indices were higher in the subgroup of patients with DIP involvement, when compared with the total cohort (DAS28CRP-EGA: r=0.47, p<0.01, SDAI-EGA: r=0.62, p<0.001 and CDAI-EGA: r=0.56, p<0.001). Moreover, correlations of the DAREA with the SDAI, CDAI and DAS28 were strong (table 4).
Spearman's correlation coefficient of DAREA with disease activity variables and composite scores at baseline
In line with previous observations on SDAI,23 CRP levels did not significantly correlate with the values of composite indices. Correlation with the physical function score of the SF36 assessment and DAREA was weak but significant (r=0.26, p<0.01; table 4), comparable to that of DAS28CRP (r=0.28, p<0.001), SDAI (r=0.26, p<0.01) and CDAI (r=0.22, p<0.01).
Analysing the observational data, very similar results were obtained (table 4), especially regarding the correlation of DAREA with other composite indices. In addition to high correlations with joint counts, in this data set also EGA and pain strongly correlated with DAREA assessment (r=0.74 and r=0.86, respectively, both p<0.001; table 4). Also, baseline HAQ scores were available, and correlation with this functional score confirmed the overall correlational validity of the DAREA. As in the trial data set, correlation of DAREA with functional assessment in the overall cohort was similar to that of other scores (DAREA-HAQ: r=0.54, as compared to DAS28-HAQ: r=0.52, SDAI-HAQ: r=0.50, CDAI-HAQ: r=0.50, p<0.001 for all). In the DIP involving subgroup, correlation of HAQ and DAREA amounted to r=0.69, p<0.001 (table 4) (compared to DAS28-HAQ: r=0.68, p<0.001; SDAI-HAQ: r=0.62, p<0.01 and CDAI-HAQ: r=0.59, p<0.001).
Sensitivity to change
DAREA, CDAI, SDAI and DAS28 at baseline and follow-up during the IMPACT trial are displayed in figure 1 and table 2. Sensitivity to change was evaluated by calculating ESs (figure 2A). These were very high (>0.8) for the active treatment arm regardless of the score, while for placebo they were generally low. Indeed, the DAREA index did not show any placebo effect (for the difference between baseline and week 14). This difference in treatment effects of the trial arms was highly significant for DAREA (p=2.56×10−10), revealing its high discriminant capacity.

Infliximab Multinational Psoriatic Arthritis Controlled Trial (IMPACT) 2 data set: values of DAREA, CDAI, SDAI and DAS28CRP at baseline and follow-up at 14 and 54 weeks. x Axis: week of follow-up; y axis: mean values±SD of the respective scores. Left panels: treatment group (infliximab, IFX), right panels: placebo group (PLAC). ***p<0.001, **p<0.01, *p<0.05. Significant difference between baseline (BL) (week 0) and week 14, as well as between BL and week 54 in the treatment group; no significant difference in the placebo group from BL to week 14. Low levels of week 54 assessment in the placebo group are explained by the escape treatment with infliximab which started at week 14 in some patients.16 CDAI, clinical disease activity index; CRP, C reactive protein; DAREA, ‘Disease Activity index for REactive Arthritis’; DAS28, Disease Activity Score using 28 joint counts; SDAI, simplified disease activity index.
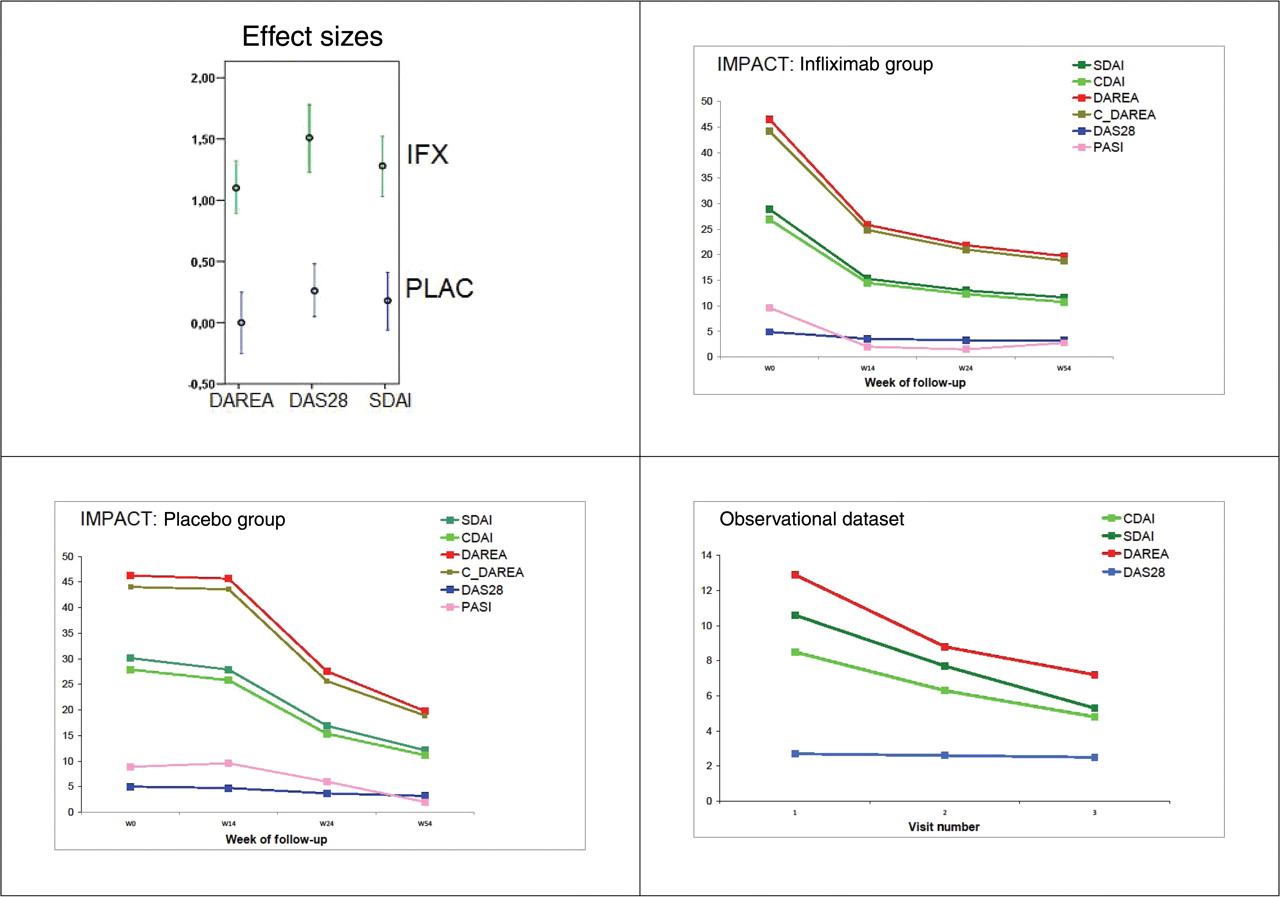
A. Effect sizes (y axis displays values) of three composite scores, DAREA, DAS28CRP and SDAI (x axis), assessed at baseline and week 14 during IMPACT 2. The placebo group shows generally low effect sizes, while in the infliximab group effect sizes are high (all above 0.8), indicating high sensitivity to change. Of note, the effect size of DAREA/DAPSA in the placebo arm is 0. B–D. Improvement of composite scores from baseline to week (w) 14, week 24 and week 54 (B, C) or consecutive visits (D); the x axis displays the time point of assessment (week of follow-up in the IMPACT 2 study/visit number in the observational data set). y axis: mean values of DAREA and C-DAREA (clinical DAREA), SDAI, CDAI, DAS28 and PASI. B. IMPACT 2 data set, infliximab treatment group. C. IMPACT 2 data set, placebo group (the decline from week 14 to week 54 reflects the employment of the escape protocol of the trial). D. Observational data: DAREA, SDAI, CDAI and DAS28ESR at baseline (visit 1=start of treatment) and follow-up. Changes of DAREA, SDAI and CDAI from baseline to visit 3 are significant (p<0.05). CDAI, clinical disease activity index; CRP, C reactive protein; DAREA, ‘Disease Activity index for REactive Arthritis’; DAPSA, Disease Activity index for Psoriatic Arthritis; DAS28, Disease Activity Score using 28 joint counts; IMPACT 2, Infliximab Multinational Psoriatic Arthritis Controlled Trial 2; PASI, psoriasis area and severity index; SDAI, simplified disease activity index.
DAREA provided good sensitivity to change also in the observational cohort assessing changes after starting a new treatment. The interval between follow-up visits was 2.8±3.5 months. At visits 2 and 3, most individual variables improved (table 3), with the exception of ESR (contrasting CRP levels). Even though the patients had mostly oligoarticular involvement, the changes of DAREA were driven by all its components, since similar improvement was seen for all of them, ranging from 0.8 (mean improvement of CRP) to 1.4 (reduction in mean 68 TJC; table 3). In line with changes of individual variables, DAREA and SDAI decreased significantly (p<0.05). The DAS28ESR did not change significantly, likely due to the low ESR levels at baseline and its subsequent slight increase, while DAS28CRP improved (p<0.05). Figure 2B–D illustrates the decrease of the various scores during follow-up in the IMPACT 2 (figure 2B,C) and the observational (figure 2D) data set. The change from week 14 to week 54 in the IMPACT 2 placebo data set (figure 2C) reflects the rescue medication given to many of these patients at week 14 and further corroborates the sensitivity to change of DAREA.
Criterion validity
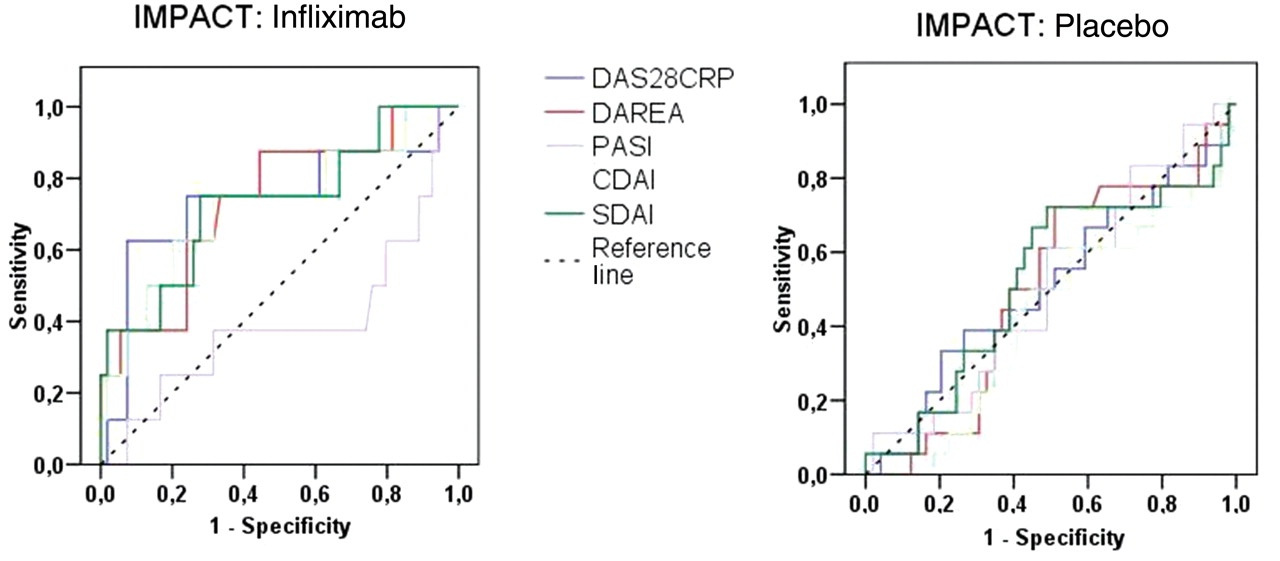
Changes of all scores were useful tests for radiographic prognosis (figure 3, table 5). Although the degree of associations was relatively low, the data revealed that disease activity assessed by DAREA, whether looking at its changes from baseline to week 24 or baseline to week 54, was associated with radiographic changes between baseline and week 54 at least to a similar extent as those of other scores. Of interest, the Psoriasis Area and Severity Index behaved dramatically different than other scores (figure 3) further supporting the notion that skin involvement does not necessarily reflect the extent of joint involvement.
{kind=link}
{kind=link}
{kind=link}
IMPACT 2 data set: receiver operating characteristic analyses of DAREA, DAS28, SDAI, CDAI and PASI change during 54 weeks of follow-up (areas under the curve (AUCs) weeks 0–54); Sensitivity and specificity with regard to radiographic progression after 1 year. A. Treatment group. B. Placebo group. CDAI, clinical disease activity index; CRP, C reactive protein; DAREA, ‘Disease Activity index for REactive Arthritis’; DAS28, Disease Activity Score using 28 joint counts; IMPACT 2, Infliximab Multinational Psoriatic Arthritis Controlled Trial 2; PASI, psoriasis area and severity index; SDAI, simplified disease activity index.
Areas under the curve (AUCs) of receiver operating characteristic analyses of DAREA, DAS28, SDAI and CDAI when used as tests for radiographic progression (defined as change of psoriatic arthritis (PsA) modified van der Heijde–Sharp score >0 at week 54; IMPACT 2 data set)
Sensitivity analyses
The DAREA is composed of two patient-centred items (PtGA and pain), one doctor centred item (SJC), one item dependent on patient and doctor (TJC) and a laboratory variable (CRP). When we exchanged PtGA by EGA, correlations with DAS28, SDAI or ESR in the observational database amounted to r=0.78, r=0.95 and r=0.30, respectively and similar results were seen for other combinations (data not shown). Thus, the correlational validity of the DAREA using its original components cannot be surpassed by combinations of other items, in line with the primary observations made in REA.19
However, since acute phase reactants are not always available at the patient's visit, we also tested a purely clinical derivation, the C-DAREA, omitting CRP; as shown in figure 3 (C-DAREA), results were comparable to the full DAREA. This is similar to previously published observations in RA utilising the SDAI and CDAI.20 23
In an additional sensitivity analysis, we focused on patients with DIP involvement (22% in the IMPACT 2 study and 41% in the observational cohort). In this subgroup, the usefulness of DAREA was particularly corroborated, since changes from baseline were well captured. Moreover, for DAREA, correlations with joint counts were generally numerically higher than those of the DAS28 and SDAI (table 6). Since DAREA was fully validated in the two cohorts of PsA studied and since the term DAREA might be misleading in the context of PsA, we assigned an additional term to the scores, namely DAPSA (for ‘Disease Activity index for PSoriatic Arthritis’) and C-DAPSA.
Spearman's correlation coefficient of composite scores with joint counts in patients with DIP involvement (according to classification of psoriatic arthritis (PsA) by Wright and Moll3) of IMPACT 2 and the observational data set
Discussion
In this study, we showed that DAREA/DAPSA, a score originally developed for another seronegative arthropathy, namely reactive arthritis, constitutes a useful measure of disease activity for PsA, exhibiting the attributes of correlational, discriminatory and criterion validity as well as sensitivity to change.
Which components should be contained in a disease activity index for PsA was still an open question until recently.18 21 A variety of items such as spinal involvement, enthesitis, dactylitis and skin and nail involvement scored highly as domains to be assessed in a survey, and so did physical function and quality of life21; however, most of these were not highly loading in a recent PCA.18 Given that various therapies may have different efficacy in skin, spinal, entheseal, nail and peripheral joint disease26 and that it is not at all clear if the pathogenetic events leading to these symptoms are the same, a score accounting for all manifestations of PsA would potentially increase the heterogeneity of responsiveness and reduce the discriminatory capacity. Therefore, the most appropriate way to assess PsA may be to employ a composite instrument for peripheral joint involvement such as DAREA/DAPSA and capture other clinical characteristics by additional instruments.4 5 7 Accounting for these aspects will allow evaluating therapies which are efficacious for certain but not necessarily other characteristics of this complex and heterogeneous disorder. Thus, the DAPSA is a peripheral arthritis disease activity index and capturing other variables, such as enthesitis, dactylitis etc may require an additional score, especially since these manifestations may sometime be predominant.
The DAPSA tended to have better correlation with individual items prototypic for PsA than other scores used in PsA clinical trials. Moreover, it has higher face validity, since it employs the 66/68 joint count rather than the 28 joint count used in the DAS28, SDAI and CDAI. In addition, it showed its value and validity in a clinical trial and an observational cohort. Future research activities in additional cohorts of patients with PsA will have to define minimal clinically important difference as minor response as well as criteria for major response for DAPSA. Another item for the research agenda will be testing the sensitivity and specificity of DAPSA in early versus late PsA.
There are some limitations to this study. First, DAPSA was originally not directly derived from patients with PsA; however, it has to be borne in mind that none of the currently available scores, including the PsARC, has been originally developed using such patient cohorts and that only DAPSA and PsARC evaluate a joint count that comprises the hand DIPs and foot joints which are frequently involved in PsA. Furthermore, the items selected as components of DAPSA might not have been the best ones to chose for PsA; however, all these items were most strongly loading in a recent PCA performed to find the most appropriate variables for the assessment of PsA18; moreover, when we exchanged several items for others, in particular PtGA for EGA, it provided no advantages in comparison with the original DAPSA. Interestingly though, an index that comprised all DAPSA components except CRP, which we name C-DAREA/C-DAPSA, gave very similar results to the original score. Also, the simplicity of calculating DAPSA/C-DAPSA might be regarded as a further limitation, because one may believe that more complex scores could be more reliable; but other scores that are based on more complex calculations do not provide advantages, while failing to assess feet and hand DIPs. Moreover, in RA, SDAI and CDAI, likewise undemanding to calculate, perform at least as well as DAS2820 23 and, like DAPSA/C-DAPSA, can be easily used both in clinical trials and clinical practice.
In conclusion, a simple summation of disease activity variables without weighting or transformation provides a useful instrument for the assessment of PsA both in the clinic and in trials. DAPSA/C-DAPSA are easy to calculate and have proven discriminative capacity and overall validity.27 Finally, DAPSA has face validity, accounting for joints often involved in PsA1 and disregarded in other scores.
References
Footnotes
-
Funding This study was supported in part by the Autocure project of the European Union.
-
Competing interests DA, AK and JSS have received grant support and/or honoraria from Centocor and/or Schering-Plough, unrelated to the present study.
-
Ethics approval This study was conducted with the approval of the individual sites.
-
Provenance and peer review Not commissioned; externally peer reviewed.