Article Text

Abstract
Objective: To report adverse events (AEs) seen in a large cohort of patients with juvenile idiopathic arthritis (JIA) treated with tumour necrosis factor (TNF)α blockers (infliximab and etanercept).
Methods: All patients with JIA treated with infliximab or etanercept at the Paediatric Rheumatologic Centre of the G Pini Institute (Milan, Italy) from November 1999 to February 2006, were enrolled in an open, single-centre, long-term prospective study
Results: In all, 163 patients (68 infliximab, 95 etanercept) were enrolled. Mean (SD) age of onset was 6.4 (4.8) years, mean age 17.1 (9.2) years, mean therapy duration 22.9 (17.6) months. A total of 45 patients (32 infliximab, 13 etanercept) failed to respond to or did not tolerate the first therapy and switched to a second one. In all, 208 treatments (81 infliximab, 127 etanercept) were performed. A total of 71 AEs occurred in 51 (62.9%) patients on infliximab and led to discontinuation in 26 (32.1%); 133 AEs occurred in 69 (54.3%) patients on etanercept and led to discontinuation in 18 (14.2%). Some AEs, such as thrombocytopoenia, neuropsychiatric disorders, new onset of Crohn disease and new onset or flare-up of chronic iridocyclitis (CIC), are unusual and have rarely been described before, yet proved to be significant in frequency and/or clinically noteworthy in the large population we followed.
Conclusions: In our 6-year study, anti-TNFα agents infliximab and etanercept were well tolerated and safe, and were associated with only few serious, but all reversible, AEs. However, such inhibitors are associated with various and numerous AEs. Children and young adults affected by JIA should be carefully monitored so as to limit the risk of AEs during anti-TNFα therapy as much as possible.
Statistics from Altmetric.com
According to International League of Associations for Rheumatology (ILAR) classification,1 2 juvenile idiopathic arthritis (JIA) includes seven categories, different from each other and from adult rheumatoid arthritis (RA). Many disease-modifying antirheumatic drugs (DMARDs) commonly used in RA have shown a lack of efficacy in controlled trials in JIA.3–6 Only methotrexate (MTX) has proven to be effective and safe in a large controlled trial.7 Nevertheless, in many cases, inefficacy or intolerance to MTX has led investigators to try other therapeutic options with debatable results.6 8–10 Prior to the era of biologicals, more than 25% of polyarticular and nearly 50% of systemic patients with JIA at 5 years after onset had functional limitations, and two-thirds had radiographically evident damage.11 Consequently, there has been a requirement for the new biological therapies to fill.
Etanercept (soluble p75TNF-receptor), is the only anti-tumour necrosis factor (TNF)α agent approved for JIA on the basis of a controlled trial.12 13 For the last 6 years, our facility has been using infliximab (chimaeric, human–murine, anti-TNFα monoclonal antibody) off-label for the treatment of refractory JIA.14 The results of the international controlled trials on infliximab and adalimumab (fully human anti-TNFα monoclonal antibody) are either only very recently published or have been published only in abstract form.15 16 Apart from these studies, the literature is limited to retrospective17 18 or open prospective studies of small series19–25 and to some national registries.26–30 The main published studies are listed in table 1.
Etanercept12 13 and infliximab14 have shown a dramatic therapeutic benefit in refractory polyarticular JIA. Nevertheless, as their use has increased worldwide, serious AEs (SAEs) but uncommon (infections, malignancies, heart failure, demyelinating disorders, lupus-like disease) have emerged.22 31 Several of these risks (eg, lymphoma and infections) can also be associated with either disease per se or previous and concomitant immunosuppressive treatments.32 In our long-term prospective experience of a large series of patients with JIA treated with etanercept or infliximab, unexpected AEs not apparent in controlled trials required for registration have emerged. It has become clear that TNFα inhibitors have a different safety profile. In order to use TNFα blockers appropriately, it is important to be fully aware of their safety profile and of the differences between them.
PATIENTS AND METHODS
All patients fulfilling JIA-ILAR diagnostic criteria1 2 treated with infliximab or etanercept from November 1999 to February 2006, were enrolled and prospectively followed. Patients, and/or both parents of patients younger than 18 years, gave their informed consent to treatment.
The infliximab starting dose was 3 mg/kg intravenously, at weeks 0, 2, 6, and every 8 weeks thereafter. Dosage could be increased up to 10 mg/kg and intervals between infusions could be reduced to 4 weeks according to clinical judgment. The etanercept dose was 0.4 mg/kg (maximum 25 mg), subcutaneously twice a week. In rare severe refractory cases, dosage was increased up to 1 mg/kg. Non-steroidal anti-inflammatory drugs (NSAIDs) and corticosteroids, if needed, MTX or other previous DMARDs, if tolerated, were continued. A complete physical examination (by an expert paediatric rheumatologist (IP)), standard laboratory tests, antinuclear antibodies (ANA) and anti-dsDNA auto-antibodies (anti-ds-DNA-Ab) were assessed at baseline and either every 2 months thereafter (etanercept), or at each subsequent infusion (infliximab). At the screening visit, chest x ray, EKG, and tuberculin skin test were performed.
All AEs were recorded on a unique registration form. According to the physician’s evaluation, the relationship between each AE and treatment was classified as:
Type A. Definite (AE firstly observed during treatment and completely resolved with its temporary or definitive suspension, or dose-dependent).
Type B. Probable (AE probably favoured by treatment, but also possible in patients with JIA not treated with anti-TNFα).
Type C. Possible/concomitant/unrelated (AE judged as possibly related or unrelated occasionally concomitant event).
Statistical analysis
Pairwise comparisons were based on the Wilcoxon matched pairs signed-ranks test. All values of p<0.05 were considered to indicate statistical significance (two-tailed test).
RESULTS
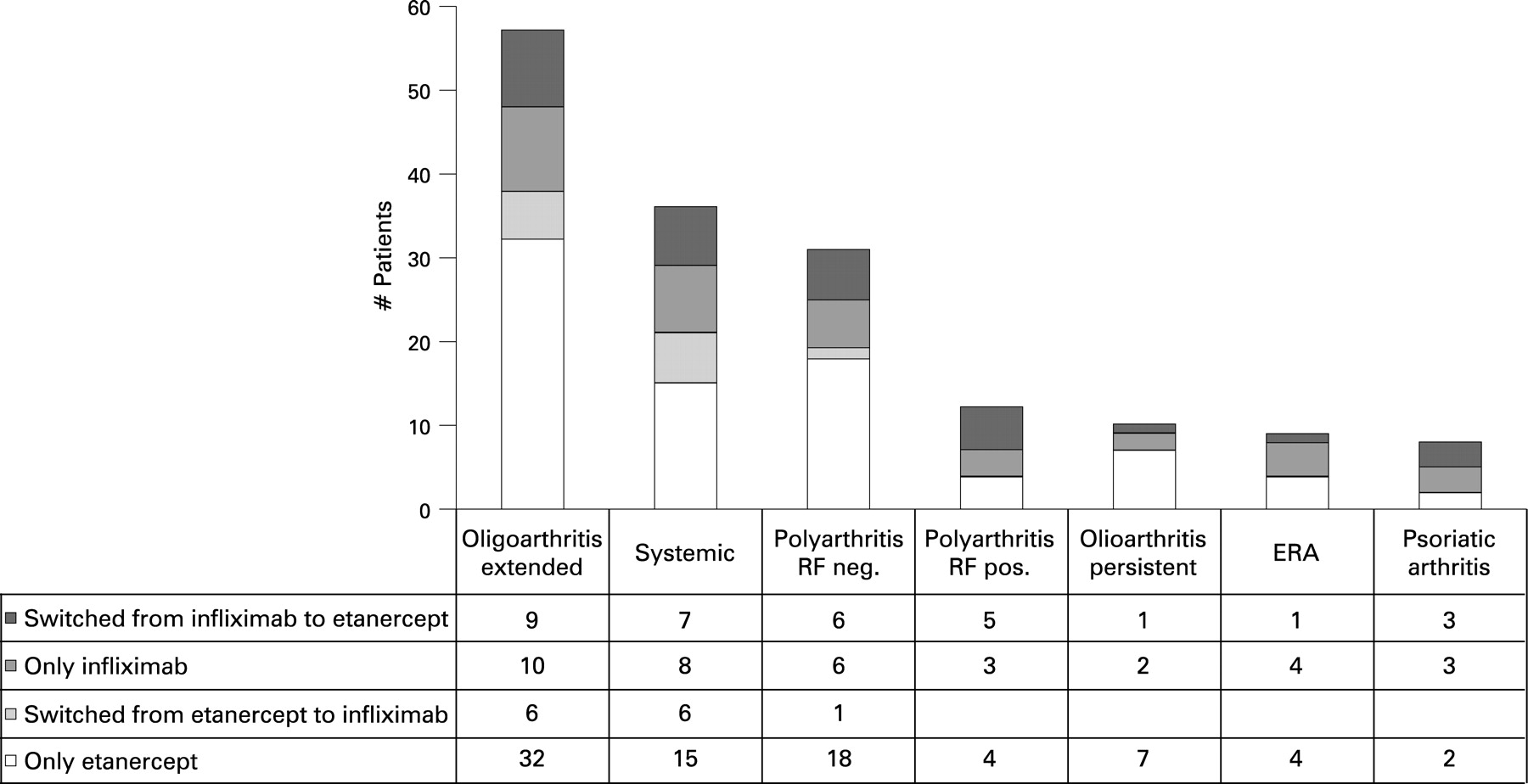
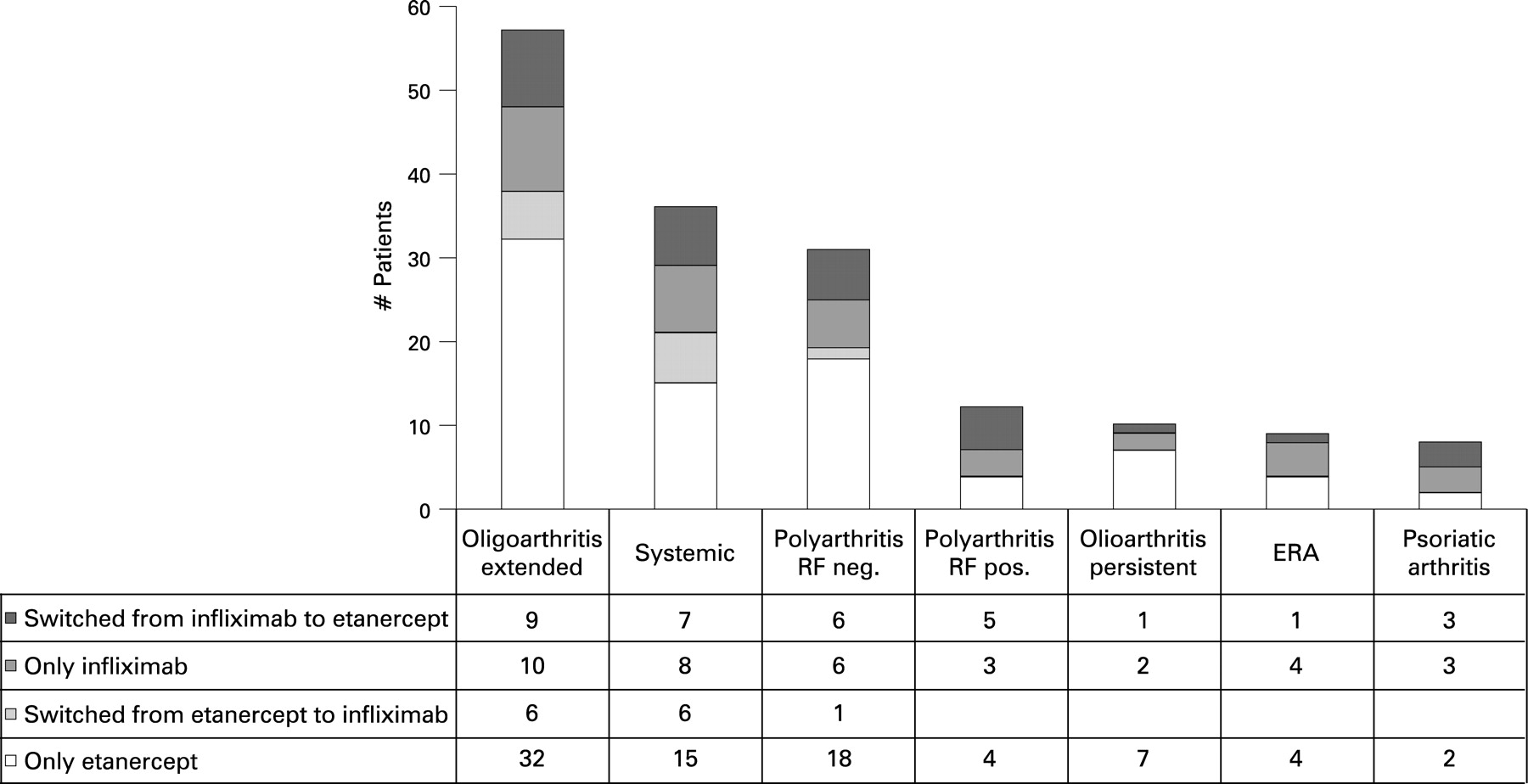
In all, 163 patients were enrolled: 68 (57 females, 11 males) on infliximab, 95 (67 females, 28 males) on etanercept. A total of 45 patients (32 infliximab, 13 etanercept) failed to respond to (or did not tolerate) the first therapy and switched to a second one; thus, a total of 208 treatments were performed: 81 infliximab and 127 etanercept. Diagnosis, treatments, and demographic data are given in figs 1 and 2 and table 2.

{kind=link}
{kind=link}
All patients were not responsive to or did not tolerate one or more DMARDs; in particular they had failed MTX. Patients enrolled from November 1999 to February 2000 were treated with infliximab for compassionate use (at that time, TNFα inhibitors were not yet approved in Italy for JIA; etanercept was approved in February 2000). Thus, they were those with a more severe long-lasting refractory disease (mean previous failed DMARDs = 4). Furthermore they had a significantly older onset age (table 2). In fact, in this group, the number of patients who were polyarticular rheumatoid factor (RF)-positive JIA, had enthesitis related arthritis (ERA) and psoriatic arthritis was significantly higher (11.8, 7.3, 8.8% vs 4.2, 4.2, 2.1%, respectively) (fig 1). This unbalanced distribution of ILAR categories explains the older onset age of this group. The 45 patients who switched to a second biological therapy, compared to the 118 who successfully continued the first one, had a significantly longer disease duration (13.6 (8.0) vs 9.5 (8.5) years). Moreover, in this group, the more severe ILAR categories (systemic and RF-positive polyarthritis) were significantly more represented (respectively, 28.9% and 11.1% vs 19.5% and 5.9%).
In all, 204 AEs complicated 120 treatments (57.7%) in a total anti-TNF treatment exposure of 398 patient years, and led to withdrawal in 44 (21.1%) (table 3).
Infliximab
In all, 71 AEs complicated 51 treatments (62.9%) and led to withdrawal in 26 (32.1%). A total of 38 patients experienced a single AE, and 13 patients had >1 AE.
Infusion reactions (IR) (AE type A) were observed in 31 patients (38.3%). Neuropsychiatric manifestations (AE type B) were observed in 10 patients (12.3%), who presented one (6 patients) or more (4 patients) neuropsychiatric events (total events = 17). Seven patients (8.6%) presented infections: six minor infections and one serious cytomegalovirus (CMV) pneumonia, complicated by macrophage activation syndrome (MAS) (AE type B). Five patients (6.2%) presented hypertension (AE type B). Three patients (3.7%) presented cutaneous lesions: one urticarial rash relapsing after each infusion (AE type A), one severe worsening of allergic skin lesions, one new onset of psoriatic rash (AEs type B). Three patients (3.7%) presented a severe flare-up or new onset of chronic iridocyclitis (CIC) (AE type C). Two patients (2.5%) presented an unexplained persistent macrohaematuria (AE type B). Individual patients (1.2%) presented other AEs judged as occasionally concomitant diseases (AE type C). These were: uterine polyp, stress fracture, deep vein thrombosis.
Etanercept
In all, 133 AEs complicated 69 treatments (54.3%) and led to withdrawal in 18 (14.2%); 30 patients experienced a single AE, 39 patients had >1 AE. Apart from frequent, mild, injection-site reactions (unrecorded), the most frequent AEs were neuropsychiatric manifestations observed in 30 patients (23.6%), who presented 1 (24 patients) or >1 (6 patients) events (total events 36). A total of 29 patients (22.8%) presented >1 infections (total events 34): 32 minor infections and 2 serious infections (1 hip prosthetic infection and 1 life-threatening bacterial pneumonia in the same patient who, when previously treated with infliximab, suffered from CMV pneumonia and MAS). A total of 12 patients (9.4%) presented a diffuse cutaneous reaction to the etanercept injection (pruritic, urticarial rash) (AE type A). Nine other various skin and/or annexal lesions were observed in eight patients (6.3%): one pityriasis versicolor, three onychodistrophy, two alopecia, two oral aphtosis (AEs type C) and one cutaneous leg ulcer (AE type B). Seven patients (5.5%) presented abdominal or epigastric pain (AE type C). Five patients (3.9%) presented the unexpected new onset of an aseptic bowel inflammation with abdominal pain and chronic diarrhoea. In three patients, a biopsy was performed. The histological diagnosis was aspecific inflammatory bowel disease (IBD) in one, and Crohn disease in two (AE type A). Five patients (3.9%) presented irregular/painful menses or gonadal pathologies (ovarian cyst, endometriosis) (AE type C). Four patients (3.1%) presented a severe persistent flare up of CIC (AE type C). Four patients (3.1%) presented tachycardia or extrasystolia (AE type B). Three patients (2.4%) presented hypertension (AE type B). Two patients (1.2%) presented leukopoenia and thrombocytopoenia (AE type A). Other various AEs were: two cases of epistaxis, single cases of proctorrhagia, bronchial asthma, biliary calculosis, coccigeal cyst, aseptic necrosis of femoral head, monoclonal electrophoretic band, thyroid microcarcinoma (AE type C) and an unexplained persistent macrohaematuria (AE type B).
All AEs and withdrawals for AEs are listed in table 3, neuropsychiatric manifestations in table 4, and infections in table 5.
Furthermore, seven patients with infliximab (8.6%) and two with etanercept (1.6%) presented newly induced anti-dsDNA-Ab (AE type A). With infliximab, we also observed newly induced anti-RNP-Ab in one patient affected by juvenile psoriatic arthritis.
DISCUSSION
As far as we know, our 6-year prospective study on safety of TNFα blockade with etanercept and infliximab in JIA is the largest conducted to date. In ours as in other studies, the tolerability of anti-TNFα therapy in JIA was good overall. In the 398 patient-treatment years of our study 204 AEs were recorded (table 3). In the 592 patient-treatment years of the German etanercept registry, there were only 69 AEs.26 In the USA etanercept registry the rate of AEs was low (21%), exactly the same as was observed with MTX.28 Etanercept also offers an acceptable safety profile in long-term treatments: after 4 years, the rate of SAEs was 0.13 and of serious infections was 0.04 per patient year, in a total etanercept exposure of 225 patient years.33 Young people generally tolerate all antirheumatic therapies better than adults. In our study, one or more AEs complicated 57.7% of treatments. Such results contrast with some adult studies where up to 95% of patients experienced at least one AE.34 The AEs observed in our population usually were not serious; all AEs were completely treated, but led to discontinuation of therapy in 21.1% of patients.
The greater number of patients who presented AEs with infliximab (62.9%) vs those with etanercept (54.3%) was due to IRs, not to other AEs that could be related to the pre-existing condition of more severe refractory disease.
As well as with other DMARDs, systemic JIA seems to be at greater risk for AEs than non-systemic JIA categories (73% vs 57%).
One of the major concerns with the chimaeric monoclonal antibody infliximab is the potential formation of human anti-chimaeric antibodies (HACA) that neutralise the drug, limiting its long-term efficacy or causing hyperergic IRs.35–37 IRs were the most common AEs in our patients treated with infliximab (38.3%). IRs (sensation of thoracic constriction, dyspnoea, flushing, urticaria) generally occurred soon after the start of infusion and, in many cases, seemed to be caused by some error in the drug reconstitution or administration (such as agitating the solution or administering the infusion too quickly). In these cases, after a brief interruption, the infusion can be restarted and completed without any further reaction. IRs could be prevented or attenuated by pre-medication with antihistamines and steroids. Nevertheless, 20.1% of our patients suspended treatment because of severe IR relapse at each infusion despite pre-medication. Similarly, in the Finland experience and in the international trial, IRs were the most frequent AE that caused withdrawals.15 19 In the international trial, HACA developed more frequently (37.7% vs 12.2%) with lower (3 mg/kg) rather than with higher (6 mg/kg) doses. Moreover, patients with HACA had a threefold incidence of IRs.15 The same results were obtained in the first studies of infliximab in RA: higher doses (10 mg/kg) significantly reduced the incidence of IRs.38 A second hypothesis is that some IRs could be related to the release of prostaglandin D2 (niacin-like effect), as described in “red man syndrome”.39 40
Transient injection-site reactions are described in about 39% of patients with JIA on etanercept.12 In our study, 12 patients manifested a diffuse cutaneous reaction that required an antihistamine treatment that led to withdrawal in two of them.
Neuropsychiatric AEs (depression, headache, manifestations of central nervous system (CNS) demyelisation, optic neuropathy) have been reported in previous experiences with etanercept in JIA.12 13 22 26 41 Nevertheless, we did not expect to observe such a high frequency of neuropsychiatric disorders, (28.1% with etanercept,12.5% with infliximab).
Neuropsychiatric manifestations with etanercept ranged from aspecific signs (headache, vertigo, fatigue, hyperactivity, nervousness, anxiety) to important behavioural alterations (severe unusual aggressiveness), definite neuropsychiatric syndromes (pain amplification, panic attacks, depression, anorexia nervosa) and rare organic signs (hypoglossal paralysis). The cases of unusual aggressiveness, severe headache and pain amplification syndrome were clearly dose dependent (occurring in patients not responders to the conventional dose and treated with higher doses) and disappeared with suspension of treatment or with dosage reduction to 0.4 mg/kg. The case of hypoglossal paralysis was difficult to explain: MRI did not show signs of CNS demyelisation or vasculitis. Similarly, but less frequently, with infliximab we observed aspecific neuropsychiatric symptoms (sleepiness, insomnia, anxiety, paresthaesia, fatigue), as well as major psychiatric syndromes (panic attacks, depression, psychoses).
All neuropsychiatric AEs completely recovered after treatment interruption or dose reduction. Major psychiatric syndromes also needed a psychopharmacological therapy.
The major concern with TNFα blockers is their potential pro-infective action. The reactivation of silent tuberculosis (TB), definitely related to TNFα inhibition, has completely disappeared as TB screening and prophylaxis are now the rule before any anti-TNFα therapy. Infliximab is associated with the greatest risk.42 Two cases of TB arthritis in systemic patients with JIA respectively treated with infliximab and etanercept have been described; the first patient died.43 44
Cases of death from sepsis are also reported.15 45 In our population, two life-threatening infections occurred in the same patient: a patient with systemic JIA with a long-lasting polyarticular course developed a CMV pneumonia complicated by MAS while on infliximab. She recovered, and she was then successfully treated with etanercept, but again, after 4 months, suffered a serious staphylococcal pneumonia. Two cases of MAS in systemic patients with JIA, respectively treated with infliximab and etanercept, were previously described.19 46 In our Rheumatological Department (consisting of two units: adult and paediatric), severe infections with biologicals are more frequent in adults. Patients with JIA have less therapeutic options, are usually treated with anti-TNFα earlier on, and thus they are less exposed to long-lasting immunosuppressant treatments and to persistent uncontrolled disease activity.
We recorded many recurrent upper respiratory (URI) or urinary tract infections (UTI), and other common, easily managed, paediatric infections (more frequently with etanercept, perhaps because of the younger age of this population and the higher baseline rate of these infections in school age children vs adolescents and young adults).
A particular paediatric concern is the immunosuppressive action of biologicals in children who are exposed to or develop varicella. In our experience, four children developed varicella while on etanercept. Treatment was temporarily interrupted in only three (alarmingly, one of them, due to poor compliance of the parents, continued etanercept even during the varicella infection). Nevertheless, there were no complications.
Another concern of TNFα blockade is its potential action to shift the pattern of immune response from T helper 1 (Th1) to Th2, thus enhancing antibody production and inducing or worsening autoantibody mediated or allergic diseases. Infliximab seems to be more frequently responsible for newly induced ANA and anti-dsDNA-Ab.47 However, only rare cases of drug-induced systemic lupus erythaematosus (SLE), discoid LE and cutaneous vasculitis are described.
Experiences with etanercept in JIA reported single cases of new onset of diabetes mellitus type 1, juvenile SLE, proliferative lupus nephritis and leukocytoclastic vasculitis, and new onset of Crohn disease.22 48–51 With infliximab, one case of relapse of autoimmune alopecia was described.19
We observed many cases of newly induced autoantibodies, but all without any autoimmune clinical manifestations.
Unexpected and surprising was the new onset of five cases of inflammatory idiopathic (aseptic) bowel diseases (IBD) in our patients treated with etanercept. In the first three cases, the diagnosis was histologically confirmed. In the two subsequent cases, the diagnosis of an initial IBD was clinically suspected (chronic abdominal pain and aseptic diarrhoea, quickly and completely recovered only after etanercept suspension). All patients were certainly affected by long-lasting definite forms of JIA. However, they had never previously suffered from abdominal complaints, nor did they present other signs suggesting that their arthritis could be a complication of a pre-existing subclinical IBD. In all patients treatment was switched to a monoclonal anti-TNFα antibody, with complete remission of the bowel symptoms.
Another concern with TNFα blockade, mainly with etanercept, is the possible reactivation of CIC. In a recent large survey and in a small controlled trial, etanercept seems inefficacious in preventing relapses of CIC.52 53 In our study, relapses of CIC during etanercept therapy occurred in 4 of 12 patients (33.3%). By contrast, there are case reports where infliximab seems to be efficacious for refractory JIA uveitis.54–60 Nevertheless, in our infliximab-treated population relapses of CIC occurred in 2 of 12 patients, and 1 case of new onset of CIC was observed. The presence of ANA seems to be important in the pathogenesis of CIC. The relapse of CIC, as the new onset of a second autoantibody mediated disease, could therefore be related to TNFα blockade and its action that favours ANA production.
Bone marrow suppression is rarely described with TNFα blockers. We observed one case of mild persistent leukopoenia and one case of severe thrombocytopoenia and leukopoenia definitely related to etanercept treatment.
More studies are needed to evaluate the baseline occurrence of malignancies in RA and JIA and to determine the adjunct risk posed by an anti-TNFα therapy. We observed one case of thyroid cancer in a 25-year-old female affected by a long-lasting persistently active RF-positive JIA while on etanercept, who had previously also been treated with infliximab, MTX and many other DMARDs.
CONCLUSIONS
From clinical experience, it appears TNFα inhibitors are well tolerated overall, SAEs are rare, and their risk–benefit profile strongly favours benefit. However, long-term safety data still need to be established. Severe infections, including TB and sepsis, have been reported. These can be largely prevented by appropriate screening and careful monitoring. Clearly, comorbidities, long-lasting persistently active disease and concomitant immunosuppressant medications all contribute to the risk of infections, malignancies, and other SAEs. In our 6-year study, infliximab and etanercept have been well-tolerated and appear safe overall, causing only a few, all reversible, SAEs. Biologicals allow better and faster disease control than was previously possible, and their early application within the “window of opportunity” in combination with conventional DMARDs seems to produce the best outcomes. Thus, for patients with JIA whose disease is not sufficiently controlled with NSAIDs and MTX, TNFα blockers may be considered the first-choice treatment.
REFERENCES
Footnotes
Competing interests: None declared.