Article Text

Abstract
Objective: To investigate the efficacy of switching to a second biological drug in rheumatoid arthritis (RA) patients.
Methods: Since 2000, Danish RA patients (n = 1021) receiving biological therapy have been registered in the nationwide DANBIO database. The first and second treatment series of patients, who switched therapy before 2005 (n = 235), were analysed for their reasons for switching, Disease Activity Score 28 (DAS28), DAS28 improvement, European League against Rheumatology (EULAR) response and drug survival. Most patients switched from infliximab to etanercept or adalimumab.
Results: Median survivals for switchers’ first/second treatment were 37/92 weeks (all patients’ first treatment 119 weeks). Reasons for switching were lack of efficacy (LOE; 109 patients), adverse events (AE; 72), other reasons (54). If patients experienced AE to the first drug, 15% had AE to the second. Median DAS28 improvements in first/second treatment at 3 months were: LOE switchers 1.1/1.6; AE switchers 1.5/0.8. In LOE switchers, a good/moderate EULAR response was more prevalent during the second treatment course than during the first (63% versus 54%, p = 0.02). AE switchers achieved similar EULAR responses to both treatments (59% versus 50%, p = 0.38).
Conclusion: LOE switchers had a better clinical response to the second treatment. AE switchers responded equally well to both treatments, with a low risk of discontinuing the second drug as a result of AE. Drug survival of the switchers’ second biological therapy was higher than of the first, but lower than that of non-switchers. No difference between various sequences of drugs were found. Danish post-marketing data thus support that RA patients may benefit from switching biological therapy.
- AE, Adverse event
- DAS28, Disease Activity Score 28
- DMARD, disease-modifying antirheumatic drug
- EULAR, European League against Rheumatology
- LOE, lack of efficacy
- RA, rheumatoid arthritis
- TNFα, tumor necrosis factor alpha
Statistics from Altmetric.com
- AE, Adverse event
- DAS28, Disease Activity Score 28
- DMARD, disease-modifying antirheumatic drug
- EULAR, European League against Rheumatology
- LOE, lack of efficacy
- RA, rheumatoid arthritis
- TNFα, tumor necrosis factor alpha
The tumor necrosis factor alpha (TNFα) antagonists, i.e. adalimumab, etanercept and infliximab, have been used for the treatment of rheumatoid arthritis (RA) in rheumatological clinical practice for up to 8 years. Controlled trials have documented their clinical efficacy.1–3 The three TNFα antagonists have not been tested head to head, but the treatment responses of the drugs appear to be similar.4
In approximately 30% of RA patients in clinical practice, the TNFα antagonist is withdrawn during the first treatment year because of a lack of efficacy (LOE) or adverse events (AE).5 It is thus relevant to consider whether these patients may benefit from switching to a second biological drug. From a theoretical point of view this is likely, because molecular structures and modes of action vary between the drugs.6 The different structures of the TNFα antagonists also make it relevant to stratify patients according to the drug.
So far, only a few small controlled clinical trials have investigated the clinical efficacy of a second biological treatment.7,8 Post-marketing data entered into clinical registries may provide useful information about patients who switch to a second biological drug.9 Since October 2000, the efficacy and AE of the biological agents in clinical practice have been registered prospectively in the nationwide Danish database for biological treatments (DANBIO).10,11
The purpose of this study was to investigate whether RA patients benefitted from switching to a second biological drug. The clinical responses were stratified according to drug and reason for switching. The treatment survivals of the first and second biological treatments were calculated, and trends in the withdrawal pattern were analysed.
MATERIALS AND METHODS
Materials
DANBIO is a Danish, nationwide, voluntary, rheumatological database of biological treatments. It covers over 90% of all prescriptions,10 and data on patient demographics, previous treatments, core measures of disease activity, reasons for withdrawal, and AE are registered prospectively.
By 31 December 2004, 1636 patients had been registered in DANBIO. Of those, 1221 patients had RA. Patients without baseline disease activity assessments (n = 172) or receiving anakinra (n = 28) were excluded from analyses, leaving a total of 1021 RA patients, hereafter designated “all patients”.
The present analyses focused on a subpopulation of 235 patients who had received at least two biological drugs, hereafter referred to as “switchers”. The initial biological drug among switchers was: infliximab 76% (178 patients; second treatment: adalimumab 56%, etanercept 44%); adalimumab 17% (39 patients; second treatment: etanercept 82%, infliximab 18%); etanercept 8% (18 patients; second treatment: adalimumab 67%, infliximab 33%). Forty-nine of the switchers had initiated a third treatment with TNFα antagonists: etanercept 26 (53%), adalimumab 15 (31%) and infliximab 8 (16%).
Methods
The patients were seen in the clinics at individual time points. After the baseline visit (0 months), the visits were approximated as follows: 0.5 month (range 1–4 weeks), 1.5 months (range 5–9 weeks), 3 months (range 10–17 weeks) and 6 months (range 18–32 weeks), etc. Therefore, a visit that had taken place between weeks 10 and 17 was registered as month 3, etc. If more than one visit had occurred during the period, the visit closest to the approximated month was selected.
The switchers were grouped according to the reason for switching: LOE, AE or other reasons (which cover other known or unknown reasons). The switchers were also stratified according to drug.
For each patient, the Disease Activity Score (28 joint count, four variables, serum C-reactive protein (CRP)-based; DAS28)12 at the initiation of the first biological treatment was chosen as the baseline. The clinical response was determined by the improvement in DAS28 over time (DAS28 improvement) and by the European League against Rheumatology (EULAR) criteria.12
The drug survivals of the first and second treatment of the switchers are presented in figure 1, with the drug survival of all patients shown for comparison.
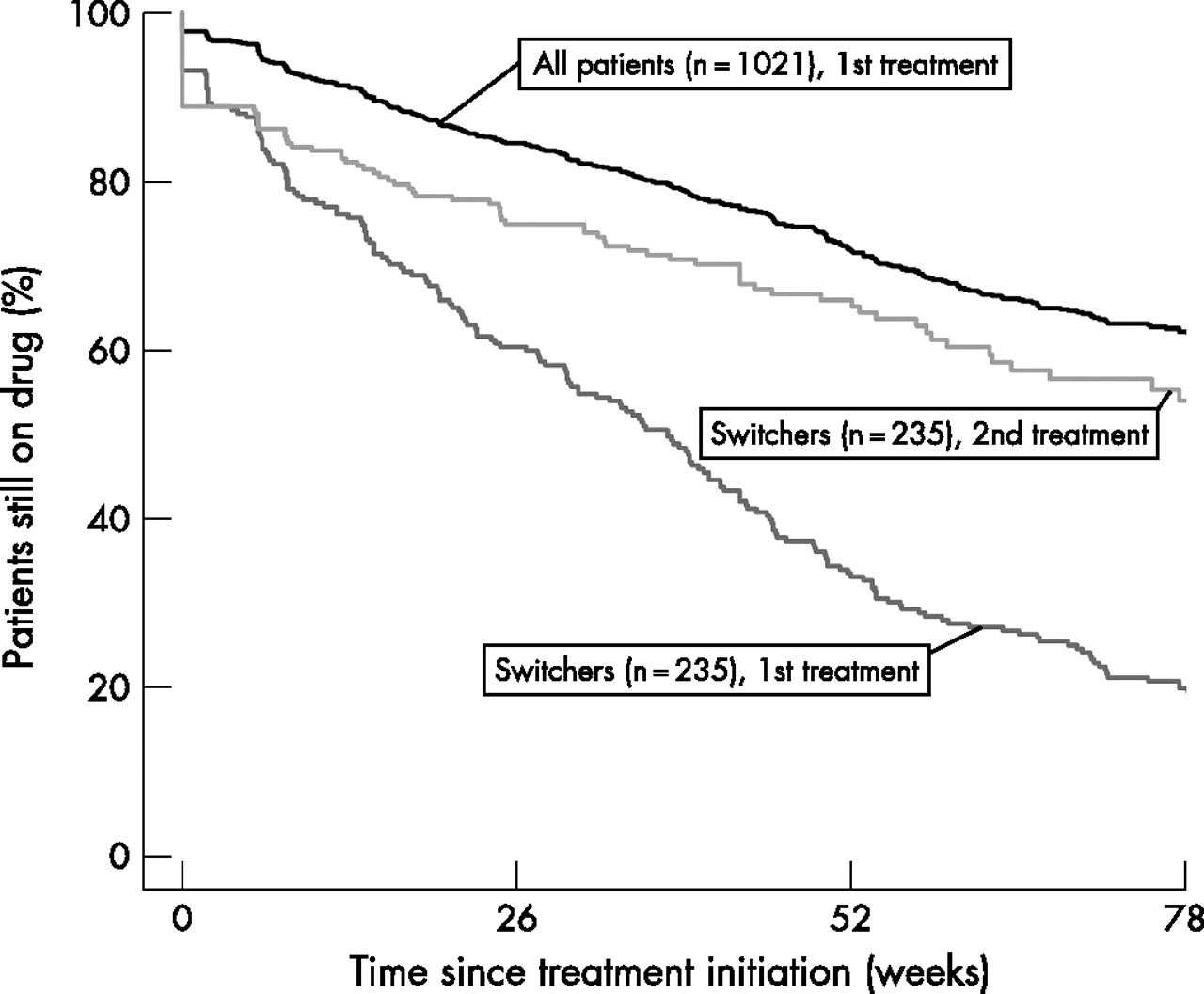
Drug survival during the first and second treatment of all switchers (n = 235) and in the whole population (all rheumatoid arthritis patients receiving their first biological therapy, n = 1021). Kaplan–Meier plots are shown.
Statistical analyses
Statistical analyses were undertaken using the Statistical Package for Social Sciences (SPSS) program, version 11.5 (SPSS Inc., Chicago, Illinois, USA). Medians and interquartile ranges (IQR) are presented. Non-parametric tests (descriptive statistics, Wilcoxon–Pratt, Mann–Whitney and Kruskal–Wallis tests) were used for the comparison of continuous variables. Dichotomous responses were analysed using χ2-tests. “Survival” analyses of the treatments were performed using Kaplan–Meier plots and log-rank tests. Probability (p) values less than 0.05 were considered significant.
Ethics
The Danish Data Registry approved the registry, and patients gave their written informed consent at inclusion. According to Danish law, the registry and its publications did not require approval by the ethics committee.
RESULTS
All patients
The clinical characteristics of the study population are shown in table 1.
Characteristics of the study population at the initiation of the first TNFα inhibitor
The median DAS28 improvement in all patients after 3 months was 1.6 (interquartile range (IQR) 0.6–2.5) and after 6 months 1.7 (0.8–2.6). The median survival time of the first treatment was 119 weeks, and 72% of the patients were still on the drug after 52 weeks (fig 1).
All switchers
Compared with non-switchers, the switchers were younger, had tried more DMARDs, used higher doses of methotrexate and had a higher baseline disease activity (table 1). The baseline disease activity for the second treatment was lower than for the first treatment course (5.2 (4.3–6.1) versus 5.9 (5.0–6.7), respectively, p = 0.002). In the 235 switchers, the median DAS28 improvements in the first/second treatments were after 3 months 1.2/1.0 (IQR 0.3–2.4/0.4–2.0), p = 0.20, and after 6 months 1.2/1.3 (IQR 0.2–2.3/0.2–2.1), p = 0.84. During the first and second treatments, the DAS28-scores had improved significantly after 3 months of therapy regardless of the reason for switching (p < 0.001). The median survival time of the first treatment was 37 weeks, and 34% of the patients still received the drug after 52 weeks. For the second treatment it was 92 weeks, with 65% on the drug after 52 weeks (fig 1), which was significantly longer than the survival of the first drug (p < 0.001).
The reasons for switching from the first treatment were LOE in 109 patients, AE in 72 patients, and other reasons in 54 patients (table 2).
Switchers, stratified by first TNFα inhibitor and by reason for switching therapy
LOE was also the most prevalent reason for withdrawal of the second biological drug (table 2).
In the 51 patients who had initiated a third biological treatment, the reason for switching from the second drug was LOE in 31 (61%), AE in eight (16%) and other reasons in 12 (24%) patients. The median DAS28 improvement in this group was 0.3 after 3 months (IQR 0.3–1.4) and 0.9 after 6 months (IQR: 0.2–2.6).
The median oral prednisolone dose in all switchers was at baseline 5 mg (IQR 0–10 mg) and at 6 months 5 mg (IQR 0–7.5 mg). At the beginning of the second treatment course, the median dose was 5 mg (0–7.5 mg) and at 6 months 0 mg (IQR 0–5 mg). Fifty-four per cent of patients received oral corticosteroids at baseline of the first treatment series and 47% at 6 months. During the second treatment, it was 51% at baseline and 44% at 6 months. The reduction in corticosteroid use was observed in all subgroups of switchers.
Switchers stratified by reason for switching
Switchers because of LOE
More women tended to switch treatment as a result of AE than LOE. Otherwise, the two subgroups of switchers were comparable (table 1). LOE was the most common reason for withdrawal of the first biological therapy (table 2).
Thirty-five patients (32%) who switched because of LOE also withdrew from the second treatment for this reason. For comparison, in the 72 patients who switched as a result of AE, 18 patients (25%) ceased the second drug because of LOE (table 2).
The DAS28 scores at 3 and 6 months were significantly lower during the second course than during the first (0.001 < p < 0.05), see figure 2A. At 3 months, the DAS28 improvement tended to be higher for the second course than for the first, and significantly more patients had a good or moderate response to the second treatment according to the EULAR criteria (63% versus 54%, respectively, p = 0.02), see table 3.
Baseline disease activity and treatment responses

{kind=link}
{kind=link}
DAS28 in the switchers (n = 235) receiving first and second biological treatments. (A) Switchers who had the first biological therapy withdrawn because of lack of efficacy (n = 109). (B) Switchers who had the first biological therapy withdrawn because of adverse events (n = 72). **p < 0.01. Only significant results are shown. CRP, C-reactive protein.
In switchers because of LOE, the DAS28 during the second treatment course was similar to the non-switchers’ DAS28 during treatment (non-significant at all time points).
Switchers because of AE
The DAS28 scores during the first and second treatment courses were similar at 3 and 6 months (fig 2B), and there was no difference in DAS28 improvement and EULAR responses between the two courses (table 3).
The AE to the first/second drug were one or several of the following: infections (in 14%/28% of patients), allergic or infusion reactions (15%/21%), rashes (22%/21%), others (62%/69%). There were 68 serious AE during the first and 14 during the second treatment course.
Eleven patients (15%), who switched because of AE, also withdrew from the second treatment course because of AE, whereas only three switchers because of LOE (3%) ceased the second treatment course as a result of AE (table 2).
Switchers stratified by sequence of drug
The baseline characteristics of the subgroups of patients stratified by the first biological drug were comparable except that more infliximab-treated patients received concomitant methotrexate (table 1).
The baseline DAS28, DAS28 improvements and EULAR responses during the first and second treatment courses for the different subgroups are listed in table 3. The effects of the first and second treatment courses as reflected in DAS28 improvement and EULAR response were similar for all combinations of drug sequences, although the number of patients in some groups were too low to perform statistical analysis. The reasons for withdrawal were similar for the three TNFα inhibitors (table 2).
DISCUSSION
This observational study, reflecting clinical practice throughout a country, showed that RA patients, who withdrew from the first biological treatment, mainly infliximab, because of LOE or AE, benefitted from switching to a second biological drug, primarily adalimumab or etanercept. The drug survival was higher after switching (92 versus 37 weeks), although it was not quite as high as for the non-switching RA patients.
Lack of efficacy was the most common reason for the discontinuation of both the first and second treatment course. Disease activity was reduced after switching, regardless of the reason for switching and the sequence of drugs administered. Withdrawal from the second drug because of AE was almost exclusively seen in patients who had also discontinued the first drug because of AE. However, even in this group fewer than one in six patients stopped because of AE.
The consensus guidelines for treatment with biological agents state that “…no well controlled switch trials have been published…”.13 Only small clinical studies have investigated whether it is beneficial to start a second biological treatment. One controlled clinical study7 showed that 24 patients who ceased infliximab treatment (because of LOE or AE) had a clinical response to subsequent adalimumab treatment that was equivalent to that observed in a comparison group who received adalimumab as the first treatment. In accordance with our results, a population-based study of 31 patients9 suggested that switching from infliximab to etanercept (mainly because of AE) or vice versa (mainly because of LOE) resulted in similar or improved response rates. Another study of 36 switchers from the same registry implied that patients who switched from infliximab or etanercept because of LOE had a similar clinical response to adalimumab compared with 26 patients initially treated with adalimumab.14 A retrospective study showed that the clinical outcomes of the treatment of 20 patients switching from etanercept to infliximab did not differ from those of 73 patients initially treated with infliximab.15 A 12-week open label study found that 25 patients switching from infliximab to etanercept mainly because of LOE experienced a clinical improvement during the second treatment.16 Another observational study with 38 switchers from infliximab to etanercept or vice versa17 showed good clinical response to the second drug regardless of the reason for switching and the sequence of drugs. This, and another study of 37 patients who switched from infliximab to etanercept with maintainance of efficacy,18 also implied that AE to the first drug do not predict AE to the second drug. However, a recent study showed, in accordance with the tendency in the present study, that both AE and LOE to the first drug can partly impact the outcome of the next treatment in the same direction.19
Data on the drug survival for second treatment courses in clinical practice have previously been published in two studies. One study of 488 patients switching between different TNFα antagonists in chronic arthritis20 concluded that the second treatment was generally shorter than the first, and was longest if the first drug was withdrawn as a result of AE. The reasons for switching were the same regardless of the drug. In the present study, the drug survival of the switcher’s second therapy was longer than that of their first biological therapy, but shorter than that of non-switchers in biological treatment. A recent study of 856 switchers showed that 73% of patients remained on the new therapy by the end of follow-up after 15 months.19 This is a larger fraction than in our study, and may reflect national differences in the pattern of initiating and switching treatment.
Data from the DANBIO registry reflect routine practice in a large number of patients followed through different treatments. It is therefore well suited for an investigation of the efficacy of switching between biological agents. Nevertheless, the present study has some limitations. The majority of subjects switched from infliximab to another TNFα inhibitor, which prevented a detailed analysis of the consequences of switching between the individual biological agents. There are several reasons for this: there was a shortage of etanercept during the first years and adalimumab was marketed later than infliximab and etanercept.
The different subgroups of switchers were generally comparable. The only difference was that more infliximab patients used concomitant methotrexate than patients receiving other biological therapies. This is, however, in accordance with international recommendations in the data collection period. The switchers had a lower baseline DAS28 in the second treatment course. This could be the result of a “carry-over” effect from the first treatment. In all subgroups, nevertheless, the second treatment course caused a DAS28 reduction.
Corticosteroid use was not restricted, but the dose was generally low. It was similar in the two treatment courses and did not increase during therapy. It could, therefore, not explain the lower disease activity observed in the second treatment course. Other confounders such as age, sex, disease activity, previous number of DMARDs and disease duration were similarly distributed in the subgroups and therefore did not seem to bias the results.
In conclusion, RA patients switching from infliximab or other TNFα inhibitors to a new TNFα inhibitor as a result of LOE showed a significantly better clinical response to the second biological drug. Patients who switched because of AE responded equally well to the second drug with only a low risk of discontinuing the second drug as a result of AE. The drug survival of the second biological therapy was higher than the first, but lower than that of non-switchers. Danish post-marketing data thus support the finding that RA patients failing one biological drug benefit from the introduction of another regardless of the reason for switching.
Acknowledgments
The authors wish to thank all contributing departments of rheumatology at hospitals in Denmark (Ålborg, Århus, Bispebjerg, Esbjerg, Fredericia, Frederiksberg, Gentofte, Glostrup, Gråsten, Herlev, Hjørring, Holbæk, Holstebro, Horsens, Hvidovre, Hørsholm, Køge, Kolding, Næstved, Nykøbing Falster, Odense, Rigshospitalet, Roskilde, Slagelse, Vejle and Viborg). DANBIO is indebted to the head of the Institute for Rational Pharmacotherapy, Jens Peter Kampmann, MD, DMSc, who hosted and financed the database from 2000 to 2003. Since 2004, Abbott, Wyeth and Schering-Plough have sponsored DANBIO. Elisabeth Hjardem received a scholarship from the Danish Rheumatism Association. The sponsors are acknowledged for their support. They have had no influence on data collection, analysis or publication.
REFERENCES
Footnotes
-
Published Online First 27 March 2007
-
Competing interests: None.