Article Text

Abstract
Background: Smoking is a well-established environmental risk factor for the development of rheumatoid arthritis (RA). However, it remains unclear whether smoking influences RA disease progression and whether smokers have more radiographic damage progression than non-smokers over time.
Objective: To compare the rates of radiographic damage progression in current smokers and non-smokers in a large prospective RA cohort.
Methods: The SCQM-RA is a population-based registry monitoring disease activity, radiographic damage and symptoms at regular intervals. All patients in the SCQM-RA database with sequential plain radiographs were included. Joint erosions were assessed in 38 hand and foot joints with a validated scoring method. The rate of erosion progression was analysed using multivariate longitudinal regression models and adjusted for potential confounders.
Results: 2004 RA patients with a mean of 3.6 sequential radiographs and 3.1 years of follow-up were included. The 545 (27%) current smokers smoked on average 16 cigarettes per day and had a mean past smoking exposure of 20.6 pack-years. Radiographic joint damage progressed at a similar rate in current smokers and non-smokers (p = 0.26). However, smoking intensity was associated with a significant inverse dose–response; heavy smokers (>1 pack-day) progressed significantly less than non-smokers or moderate smokers (p<0.001).
Conclusion: Radiographic joint damage progressed at an equivalent rate in smokers and non-smokers. Furthermore, a significant trend was observed for reduced radiographic progression and generally more favourable functional scores among heavy smokers, suggesting that cigarette smoke does not accelerate RA disease progression.
- rheumatoid arthritis
- joint damage
- environmental exposures
- smoking
- HAQ, Health Assessment Questionnaire
- ICC, intraclass correlation coefficient
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- SCQM-RA, Swiss Clinical Quality Management programme for RA
Statistics from Altmetric.com
- rheumatoid arthritis
- joint damage
- environmental exposures
- smoking
- HAQ, Health Assessment Questionnaire
- ICC, intraclass correlation coefficient
- RA, rheumatoid arthritis
- RF, rheumatoid factor
- SCQM-RA, Swiss Clinical Quality Management programme for RA
Rheumatoid arthritis (RA) is a chronic inflammatory disease that causes progressive joint destruction, disability and premature death. As a complex inflammatory disease, genetic and environmental risk factors are thought to be important in its pathogenesis.1,2 Long-term outcomes such as severe disability and surgical joint replacement occur relatively late in the disease. The rate of progression of joint damage on radiographs is a measurable proxy for RA severity, representing cumulative disease activity for an individual patient. Many studies have shown that radiographic joint damage is associated with long-term loss of function, long-term disability,3,4 employment status5 and social security disability status.6 Radiographic measures of joint damage are generally considered the “gold standard” for treatment efficacy studies7 and controlling progressive joint damage has become a goal for the management of RA.8
Smoking is the best-established environmental risk factor for the development of RA9–19 and potential mechanisms are starting to be understood.2 Some studies have suggested that smoking also influences RA disease severity,20–24 however, this remains controversial.23 In cross-sectional studies, smokers have higher concentrations of rheumatoid factor (RF),21–23 more rheumatoid nodules,21–23,25 lower grip strength,22 more functional disability,22 higher levels of disease activity23 and more erosions on radiographs.20–23 However, because of the cross-sectional design of these studies, no causal relationships have been established. In contrast, in longitudinal studies, current and past smokers had similar rates of radiographic damage progression,23,24,26,27 had less persistent synovitis26 and were less likely to require total joint arthroplasty.28
To date, it remains unclear whether smoking influences disease severity or disease progression in established RA. In particular, we do not know whether current smokers have more radiographic damage progression than non-smokers over time, which might be another critical incentive for patients with RA to quit smoking. The aim of this study was therefore to assess the influence of current smoking on the rate of radiographic damage progression in RA patients. Our a priori hypothesis was that cigarette smoking would accelerate the erosive disease process.
METHODS
Study population
The Swiss Clinical Quality Management programme for RA (SCQM-RA) is a longitudinal population-based cohort of patients with RA. The programme is under the auspices of the Swiss Society of Rheumatology, and aims to improve the quality of care for patients with RA by providing feedback on outcomes for individual patients to the physician (provider feedback).29 Rheumatologists are further motivated to enrol patients in the SCQM-RA as they are allowed to deduct drug costs for enrolled patients from their global treatment expenditures, scrutinised by the health authorities. Currently more than two-thirds of all practising rheumatologists in Switzerland are contributing patients to the SCQM. Patients come from a wide range of settings: about 60% come from private practices, 20% from academic centres and 20% from non-academic centres. Patients enrolled in the database tend to have more severe disease and receive biologic therapies more often than RA patients in the general population, because the recruitment is exclusively carried out by rheumatologists.30–32 The SCQM system requests at least yearly assessments of disease activity, radiographic damage, antirheumatic therapy, sociodemographic factors and lifestyle characteristics, including cigarette smoking history.
Study design
This is a longitudinal observational study of a population-based cohort of patients with RA. The analysis included data collected between March 1996 and November 2005. The inclusion criteria were a diagnosis of RA by a rheumatologist and at least two consecutive sets of radiographs. Exclusion criteria were a missing smoking status or missing follow-up radiographs.
Outcome variables
The study’s primary outcome was the progression of radiographic joint damage as measured by changes from baseline in radiographic damage scores. Radiographic damage was assessed prospectively by a single assessor on serial radiographs with a validated scoring system (Ratingen Score) according to a published method.33 The scoring method is sensitive to change and less susceptible to ceiling effects in advanced disease because of a true ordinal rating scheme.34 The reliability of this scoring method is excellent with an intraclass correlation coefficient (ICC) for intra-rater reliability of 0.8 to 0.9 and an ICC for inter-rater reliability of 0.7 to 0.9.33,35 The minimal detectable radiographic change for this method has been determined to be 3.3% of the maximum score.33 The intra-rater reliability for the study assessor of these radiographs is good with an ICC of 0.94 for a cross-sectional assessment and an ICC of 0.71 for change scores.
A secondary outcome of this study was the progression of functional disability as measured by change from baseline in the Stanford Health Assessment Questionnaire disability index36 (HAQ). The HAQ is a 20-item self-report questionnaire ranging from 0 to 3, which tends to increase slowly over time in RA (average of 0.03 units per year6). The HAQ is the most widely used functional status questionnaire in rheumatology and has been shown to predict work disability,37 joint replacement,37 medical costs38 and mortality39 in RA.
Exposure variable and predictors
The exposure of interest for this study was current smoking. All patients were categorised as smokers or non-smokers based on current smoking status in the patient’s self-reported questionnaire. Patients discontinuing smoking or starting smoking during the observation period were also categorised as smokers. In order to explore a potential dose–response effect of smoking, we further stratified smokers into “heavy smokers” (more than one pack/day) and “moderate smokers” (one pack/day or less). Other important predictors of RA disease progression such as measures of disease activity, self-assessed symptom questionnaires, various disease characteristics and demographic characteristics, were extracted from the database to be used in the analysis. We further determined the dominant antirheumatic treatment regimen utilised during the time span in between consecutive radiographic assessments and used this variable to control the analysis for DMARD use. The dominant antirheumatic treatment was operationally defined as the regimen used during more than 50% of the follow-up period.
Statistical analysis
Based on previous studies with this dataset,31 we calculated that a sample size of 102 patients per group with an alpha error of less than 0.05 would provide 90% power to detect a two-sided difference of at least 1 Ratingen score unit (0.5% of the maximum score) in radiographic damage progression per year, which represents a small difference.
Baseline disease characteristics were compared between the three groups using one-way ANOVA for normally distributed continuous variables and the Kruskal-Wallis test for non-normally distributed continuous variables. For dichotomous variables, Pearson’s Χ2 test was used to evaluate the significance of differences in proportions. Fewer than 5% of covariates were sporadically missing; in order to minimise potential bias, we used the population average of the respective covariates as a substitute.
Confounding was a concern in this study, as it is known from the literature that patients who smoke tend to present to physicians with more severe RA. Because such differences may substantially influence disease progression, we used multivariate adjustment to overcome such confounding effects. Radiographic and functional disability progression were analysed using generalised mixed models for longitudinal data.40 We first selected the best fitting model without controlling for potential confounders (crude model). We verified that the multivariate normal assumption for longitudinal models was satisfied and examined whether time as a linear trend or as a polynomial function fit the data best. We then adjusted the analysis for differences in baseline disease characteristics. Rheumatoid factor, age, sex, DAS28, HAQ, disease duration and DMARD use were all considered confounders a priori and added into the model. We tested other covariates using a backwards stepwise selection approach. The final model was adjusted for differences in baseline damage scores, disease activity (DAS28), functional disability (HAQ), use of DMARDs and glucocorticoids, presence of rheumatoid factor, gender, age, disease duration and education level. Point estimates of the regression model were used to produce the result graphs (fig 1). We also explored potential effect modification by sex, by presence of rheumatoid factor and by therapy with TNF inhibitors. All statistical tests were two-sided and evaluated at the 0.05 significance level. The statistical analysis was performed with Stata version 9.2 for Windows (Stata Statistical Software, Texas, USA).
{kind=link}
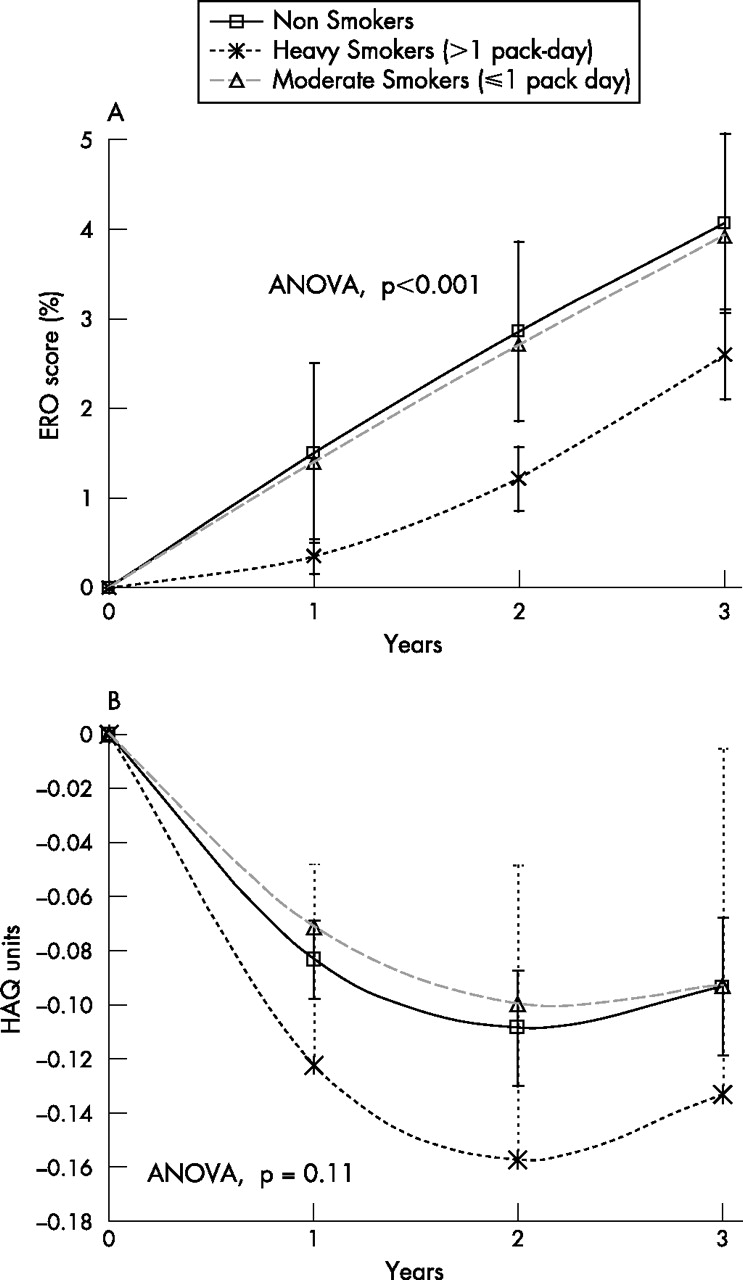
A represents radiographic joint damage progression ( = ERO) over time. The vertical lines represent the 95% confidence interval of the mean. The progression trajectories depicted are adjusted for differences in baseline differences in baseline damage scores, disease activity (DAS28), functional disability (HAQ), use of DMARDs and glucocorticoids, presence of rheumatoid factor, gender, age, disease duration and education level ( = adjusted model). ERO score (%) represents the percentage of maximum possible damage of the Ratingen erosion score and corresponds to the average proportion of joint surface damaged by erosions. B represents progression of functional disability ( = HAQ) over time. The vertical lines represent the 95% confidence interval of the mean. The progression trajectories depicted are adjusted for differences in baseline differences in baseline functional disability (HAQ), disease activity (DAS28), use of DMARDs and glucocorticoids, presence of rheumatoid factor, gender, age, disease duration and education level ( = adjusted model). The HAQ score from the Stanford Health Assessment Questionnaire ranges from 0 to 3, where 3 represents the maximum possible disability.
RESULTS
Of the 3601 patients with RA in the SCQM-RA registry, a total of 2004 RA patients with an average of 3.6 sequential x rays and 3.1 years of follow-up met the study inclusion criteria (56%). All excluded patients (1597 patients) were missing follow-up radiographs. Because missing radiographic follow-up is generally related to a recent enrolment in the database (median enrolment in 2004 versus 2001 for study patients, p<0.0001), we assumed absent follow-up to be missing at random. The 545 (27%) current smokers consumed on average 16 cigarettes per day and had a mean past smoking exposure of 20.6 pack-years. Five patients reported ceasing smoking and none reported starting smoking during the observation period. Smokers categorised as heavy smokers (n = 55) reported an average intake of 33 cigarettes/day and 27.7 years of smoking, compared with an average of 13 cigarettes/day and 24.2 years of smoking for moderate smokers (n = 489). As expected, smokers were more often male, of younger age, and had shorter disease duration with consequently less joint erosions at baseline (table 1). Other important risk factors for disease progression such as rheumatoid factor seropositivity, antirheumatic therapy, glucocorticoid use, functional status and educational level did not differ significantly between smokers and non-smokers.
Baseline patient characteristics
Radiographic damage progression
No evidence for more rapid progression of radiographic joint damage was seen among smokers compared to non-smokers. In the crude analysis, unadjusted radiographic damage progressed by 2.75% (95% CI: 2.54–2.96) at 2 years in non-smokers compared to 2.47% (95% CI: 2.10–2.79) in smokers (p = 0.14). In the fully adjusted model, radiographic damage progressed by 2.79% (95% CI: 2.59–3.02) at 2 years in non-smokers compared to 2.51% (95% CI: 2.14–2.89) in smokers (p = 0.26). However, we found an inverse dose–response effect for heavy smokers compared to moderate smokers and non-smokers (trend test, p<0.001). Specifically, radiographic erosions evolved significantly more slowly in heavy smokers than in non-smokers (p<0.001), whereas erosive disease in moderate smokers progressed at a rate similar to that in non-smokers (p = 0.65). In two years, heavy smokers progressed an average of 1.21% (95% CI: 0.23–2.25) of the maximum damage score, moderate smokers by 2.71% (95% CI: 2.35–3.06) and non-smokers by 2.86% (95% CI: 2.65–3.07) (fig 1a). In a sensitivity analysis, we examined current smoking exposure as a continuous variable and with an alternative categorisation and found qualitatively the same inverse dose–response effect (data not shown). Analyses restricted to subgroups of patients with RF positive disease, male patients and patients treated with TNF inhibitors yielded qualitatively very similar results. The strongest predictors of radiographic damage progression were disease duration, baseline radiographic damage and RF.
Progression of functional disability
To examine the consistency of the radiographic data, we repeated the analysis with the HAQ score as the outcome. Patients had a mean of 5.4 sequential HAQ score assessments during the observation period. Overall, mean HAQ scores tended to improve somewhat during the first years of the observation (–0.034 at 1 year (95% CI: –0.025; –0.043) and –0.054 at 2 years (95% CI: –0.038; –0.070), related to the initiation of new antirheumatic therapies at the time of enrolment into the database (fig 1b). As with the radiographic data, the evolution of HAQ scores did not differ significantly between smokers and non-smokers (crude analysis p = 0.36; adjusted p = 0.35). We found no significant inverse dose–response effect with functional disability in heavy smokers compared to moderate smokers and non-smokers (trend test, p = 0.68; ANOVA, p = 0.11). However, heavy smokers also tended to have more favourable HAQ scores than non-smokers, although the difference did not reach significance. At 2 years, heavy smokers improved their functional scores on average by –0.16 (95% CI: –0.05;–0.27), moderate smokers by –0.10 (95% CI: –0.06;–0.14) and non-smokers by –0.11 (95% CI: –0.09;–0.13) (fig 1b). We did not find any effect modification of smoking by gender, by RF positivity or by TNF inhibitor therapy. Strong predictors for functional disability were high baseline HAQ score, female gender, RF and lower educational levels.
DISCUSSION
While smoking is a well-established environmental risk factor for the development of RA, in particular seropositive RA, its effects on RA severity are still controversial. In this large observational study, we found no difference in the progression of radiographic joint damage or functional disability between current smokers and non-smokers. We observed an unexpected inverse dose–response with current smoking intensity; heavy smokers had less radiographic disease progression than moderate smokers and non-smokers. The evolution of functional capacity displayed a similar trend, although it did not reach significance. This suggests that smoking may be more important in the initiation of RA than in the perpetuation of the erosive disease process.
Other studies have examined radiographic damage related to smoking status with conflicting results.21–24,26,27,41 All studies that have demonstrated significant associations between radiographic joint damage and smoking were cross-sectional analyses.21–23,41 Cross-sectional studies are unable to establish the temporality of events, limiting their ability to make causal inferences. For example, disease severity could influence smoking habits, which in turn would bias an association between smoking and disease severity in cross-sectional analyses. Furthermore, smoking is associated with socioeconomic factors and disease characteristics that could confound the association with RA disease severity. In longitudinal studies examining the association between cigarette smoking and radiographic progression, no effect of overall current or past smoking has been seen.23,24,26,27 Some of these studies reported a dose–response with cumulative smoking exposure on radiographic damage,24 but others have not.23,26 Interestingly, the only other longitudinal study that examined the impact of current smoking also described a possible inverse dose–response upon radiographic progression.26 Furthermore, the authors of that study also found that current smokers had significantly fewer swollen joints over time.26 Wolfe et al unexpectedly found that past or present smoking was protective against requiring total joint replacement in RA.28 Taken together, these results suggest that the discrepancy between published studies on the effect of smoking on RA severity may be related in part to study design (cross-sectional versus longitudinal). Our findings are in agreement with other longitudinal analyses examining the effect of smoking on radiographic progression.23,24,26,27 The larger sample size of our observation may have allowed us to demonstrate a significant inverse dose–response with current smoking intensity.
Functional disability correlates relatively well with long-term radiographic joint damage in established RA.41 As with radiographic change, we did not find significant differences in the evolution of functional disability (HAQ scores) between current smokers and non-smokers, nor did we see a significant dose–response effect. Others have made similar observations concerning functional capacity and smoking,24,26 which might be due to the lower sensitivity to change of functional measures compared to radiographic outcomes. Overall changes in functional capacity over time were very small and not clinically significant.38
Smoking is related in a dose-dependent fashion to RF and anti-CCP antibody titres, both in healthy individuals and in RA patients.2,20,21,24,42,43 Furthermore, a gene–environment interaction has been reported between the HLA-shared epitope and cigarette smoking in determining the risk of seropositive RA.44 It is hypothesised that smoking induces citrullination of certain peptides, which, in the presence of the shared-epitope, may lead to the expression of anti-CCP antibodies and the development of RA.1,2 In the present study, we explored a potential interaction between smoking and RF, because HLA shared epitope and the anti-CCP status was not available. We found no effect modification of the association between smoking and radiographic progression by the presence of RF, suggesting that this interaction may play a role in the pathogenesis of RA, but not necessarily in disease severity. Other biological effects of smoking have been hypothesised such as direct effects on the immune function.45 It would seem logical to assume that the same mechanisms that intervene in disease susceptibility could also induce more severe forms of RA.21
The finding that heavy smokers have less radiographic progression was not expected. However, smoking has been reported to protect against the development and the severity of osteoarthritis 46–48 and demonstrated protective effects in several other inflammatory diseases such as ulcerative colitis or Kaposi’s sarcoma.26,49–51 The results of different clinical studies suggest that nicotine, one of the multiple components of tobacco, possesses anti-inflammatory properties. These regulatory effects are mediated by the α7 nicotinic acetylcholine receptor (α7 nAcR), which is expressed on macrophages and endothelial cells.52 Indeed, acetylcholine released following stimulation of the vagus nerve and administration of agonists such as nicotine decreases the release of pro-inflammatory cytokines such as TNF-α by macrophages in experimental models.53 Nicotine inhibits the expression of adhesion molecules induced by TNF-α, and blocks leucocyte migration in the carrageenan air pouch model. This inhibitory effect of nicotine in endothelial cells is mediated by blocking the activation of NF-κB induced by TNF-α.52 Recently, it has been shown that nicotine can dampen macrophage activation by stimulating the production of the suppressor of cytokine signalling (SOCS)3,54 a member of a family of negative signalling regulators that exerts potent anti-inflammatory effects in experimental arthritis.55 Another potential pathway through which nicotine can exert anti-inflammatory properties is spinal activation of the primary afferent nociceptor, which inhibits plasma extravasations in animal models of arthritis.56 Currently, several trials testing therapeutic approaches targeting the α7 nicotinic receptor are ongoing.51,57,58 Taken together, both clinical observations and results of experimental models suggest that nicotine may exert protective effects in inflammatory diseases and thus, may support our finding in RA.
Our study does have several limitations. Forty-four per cent of patients in the registry had no radiographic follow-up and were excluded. Study subjects without radiographic follow-up were overall similar in their socioeconomic and disease characteristics (data not shown), except for a higher proportion of smokers in subjects without radiographic follow-up (39% versus 27%, p<0.001), but a similar proportion of heavy smokers (11%, p = 0.71). Our results could be biased if missing radiographic follow-up were associated with both smoking and with more severe radiographic progression. We have several reasons to think that our results are not due to selection bias. First, the main cause for missing radiographic follow-up was recent enrolment in the database with insufficient time for subsequent radiographs (median enrolment in 2004 versus 2001 for those missing versus those not missing radiographic data, p<0.0001). Second, while an association with smoking appears to exist, we have no indication that missing radiographic follow-up is related to a more severe disease progression. On the contrary, patients with more severe disease are likely to be evaluated more closely and regularly assessed by radiographs than patients with a more benign evolution, which would tend to bias these results towards the null. Third, important prognostic factors of disease progression, such as disease activity (DAS28), functional capacity (HAQ) or estimated prior radiographic progression, did not differ significantly among smokers that were included and or excluded from this study.
We employed self-reported smoking exposure status, which may be prone to misclassification. While patients may under-report their daily tobacco consumption to please their physicians, it is highly unlikely that the current smoking status was differentially misclassified by levels of disease severity. We have not examined the impact of past smoking, which also has been associated with more severe disease in past studies.20,24 Because of the wording of our questionnaire, most current non-smokers did not report past smoking. Therefore, we felt that this information was probably unreliable and chose not to analyse it. Furthermore, cumulative cigarette exposure was highly correlated with current smoking intensity, making it difficult to dissociate the effect of past and current smoking. We also could not examine the influence of passive smoking, which was not assessed in the questionnaires. Nevertheless, the primary objective of this study was to examine pragmatically whether current smokers had more rapid disease progression in established RA, independent of their past smoking history. While we were able to control the analysis for potential confounding by important prognostic factors such as RF, socioeconomic status, disease activity and duration, and drug therapies received, we cannot exclude the possibility of residual confounding or unmeasured confounding, nor dynamics such as a potential “survivor effect” in chronic smokers, such that the patients most affected by smoking have quit in the past.
The main strength of our analysis is the use of a large, prospectively followed, population-based RA cohort. As enrolment in the SCQM-RA database is determined by physician and treatment choices (patients on biological therapy are preferentially enrolled), there is little chance that smokers or non-smokers were differentially enrolled. Quantification of radiographic destruction was performed using validated and reproducible methods with high intra-rater and inter-rater correlations. The power of our study was sufficient to detect small differences in rates of radiographic progression and notably larger than other studies that have examined the effects of smoking on radiographic progression. We employed a longitudinal analysis accounting for therapies, socioeconomic factors and other important confounders.
In conclusion, no difference was demonstrated in the progression of radiographic joint damage or functional disability between current smokers and non-smokers in this cohort of patients with established RA. However, an inverse dose–response emerged with smoking intensity. Heavy smokers demonstrated significantly less radiographic disease progression than mild smokers and non-smokers. Overall, this suggests that smoking may be more important in the initiation of RA than in the perpetuation of the erosive disease process. Possibly high levels of nicotine exposure could have anti-inflammatory effects, with beneficial consequences on RA disease progression. However, global health risks associated with smoking are much greater than those potential benefits. In particular, the cardiovascular hazards of smoking certainly outweigh the potential anti-inflammatory benefits of nicotine. Further research is needed to understand the impact of cigarette smoking on human immunity and identify the effects of tobacco exposure on RA disease outcomes.
Acknowledgments
We are grateful to the SCQM staff for data management and support and to participating physicians and patients who made this study possible.
SCQM has received grants from the Swiss Health authorities (BAG), the Swiss Academy for Medical Sciences (SAMW), the JL Warnery Foundation, the Swiss Society of Polyarthritic Patients (SPV) and private companies (Abbott, Essex, Wyeth, Roche, Bristol-Myers Squibb, Mepha, Novartis, Sanofi-Aventis).
We wish to thank specifically those rheumatologists who enrolled large numbers of these patients (10 or more, in order of numbers included): Colla F, Winterthur; Suter JB, Bern; Chamot A-M, Morges; Lehmann T, Bern; Martin A, Liestal; Wicht F, Solothurn; Marbet Grierson G, Olten; Tinner H, Weinfelden; Aellen P, Nyon; Elmiger B, Bern; Hafelin F, Schlieren; Muller-Werth B, Sarnen; Wiedersheim P, St Gallen; Buchler I, St Gallen; Gerster, J-C, Lausanne; Rappoport G, Yverdon-les-Bains; Cunningham T, Geneva; Brucker R, Luzern; Kloti R, Brugg; Glenz D, Visp; Pancaldi P, Muralto; Diethelm U, Mannedorf; Sturzenegger J, Kreuzlingen; Zenklusen C, Neuchatel; Buchard P-A, Sion; Altermatt R, St Gallen; Messikommer M, Visp; Fluck A, Zurich; Wuest P, Basel; Sauvain M-J, Fribourg; Frey D, Basel; Pfister S, Bulach; Thiebaud G, Geneva; Eigenmann B, Zurich; Muff L, Affoltern a Albis; Keller F, Uster; Brunner H, Thun; Schwartz GM, Geneva; Buchs N, Geneva; Ziehmann M, Zurich; Gut C, Reinach; Maager R, Aarau; Raccaud O, Lausanne; Saxer M, Basel; Maclachlan D, Heiden; Laubscher A, Bad Ragaz; Reich-Rutz C, Zurich; Schaub K, Mannedorf; Schlor-Dorr U, Reinach; Widmer M, Wetzikon; Baumgartner E, Porrentruy; Davoine G-A, Geneva; Christen B, Lugano; Kowalski M, Solothurn; Gratzl S, Basel; Bodmer F, Geneve; Hunkeler M, Neuchatel; Gaeumann U, Murten; Caravatti M, Wetzikon; Lamoth M, Schaffhausen; Schonbachler J, Zurich; Seglias J, Burgdorf.
We also want to thank specially participating rheumatology clinics that registered large numbers of these cases (20 or more): Universitatsspital, Zurich; Inselspital, Bern; Kantonsspital, Aarau; Centre Hospitalier Universitaire Vaudois, Lausanne; Kantonsspital, Winterthur; Bethesda Spital, Basel; Felix-Platter-Spital, Basel; Kantonsspital, St Gallen; Kantonsspital, Luzern; Hopital Cantonal Universitaire de Genève, Geneva; Triemli Stadtspital, Zürich; Hopital de La Chaux-de-Fonds, Neuchatel; Thurgauer Klinik St Katharinental, Diessenhofen; aarRehab Schinznach-Bad, Aarau; Schulthess Klinik, Zürich; Burgerspital, Solothurn; Hopital Regional, Delemont.
REFERENCES
Footnotes
-
Published Online First 19 January 2007
-
Funding: Axel Finckh is supported by a research grant from Geneva University. S. Dehler is supported by the SCQM Foundation; Karen H Costenbader is supported by an Arthritis Investigator Award from the American College of Rheumatology and the Arthritis Foundation, NIH K12 HD051959, and a Katherine Swan Ginsburg Memorial Award. C. Gabay is supported by the Swiss National Science Foundation (Grant N° 320000–107592)
-
Competing interests: None