Article Text

Abstract
Objective: To investigate the contribution of red blood cell (RBC) methotrexate polyglutamates (MTX PGs), RBC folate polyglutamates (folate PGs), and a pharmacogenetic index to the clinical status of patients with rheumatoid arthritis treated with MTX.
Methods: 226 adult patients treated with weekly MTX for more than 3 months were enrolled at three sites in a multicentred cross sectional observational study. Clinical status was assessed by the number of joint counts, physician’s global assessment of disease activity, and a modified Health Assessment Questionnaire (mHAQ). RBC MTX PG and folate PG metabolite levels were measured by high performance liquid chromatography fluorometry and radioassay, respectively. A composite pharmacogenetic index comprising low penetrance genetic polymorphisms in reduced folate carrier (RFC-1 G80A), AICAR transformylase (ATIC C347G), and thymidylate synthase (TSER*2/*3) was calculated. Statistical analyses were by multivariate linear regression with clinical measures as dependent variables and metabolite levels and the pharmacogenetic index as independent variables after adjustment for other covariates.
Results: Multivariate analysis showed that lower RBC MTX PG levels (median 40 nmol/l) and a lower pharmacogenetic index (median 2) were associated with a higher number of joint counts, higher disease activity, and higher mHAQ (p<0.09). Multivariate analysis also established that higher RBC folate PG levels (median 1062 nmol/l) were associated with a higher number of tender and swollen joints after adjustment for RBC MTX PG levels and the pharmacogenetic index (p<0.05).
Conclusion: Pharmacogenetic and metabolite measurements may be useful in optimising MTX treatment. Prospective studies are warranted to investigate the predictive value of these markers for MTX efficacy.
- AICAR, amino-imidazole carboxamide ribonucleotide
- CI, confidence interval
- DMARD, disease modifying antirheumatic drug
- mHAQ, modified Health Assessment Questionnaire
- MTX, methotrexate
- MTX PG3, MTX triglutamate
- PGs, polyglutamates
- RBC, red blood cell
- RFC, reduced folate carrier
- TS, thymidylate synthase
- VAS, visual analogue scale
- pharmacogenetics
- methotrexate
- methotrexate polyglutamates
- drug monitoring
Statistics from Altmetric.com
- AICAR, amino-imidazole carboxamide ribonucleotide
- CI, confidence interval
- DMARD, disease modifying antirheumatic drug
- mHAQ, modified Health Assessment Questionnaire
- MTX, methotrexate
- MTX PG3, MTX triglutamate
- PGs, polyglutamates
- RBC, red blood cell
- RFC, reduced folate carrier
- TS, thymidylate synthase
- VAS, visual analogue scale
Several studies in controlled and uncontrolled clinical trials have established that methotrexate (MTX) is an effective disease modifying antirheumatic drug (DMARD).1–,3 Yet, there is a large interpatient variability in the response to MTX, and the drug is inefficient at controlling disease activity and achieving remission in 30–40% of patients.4–,7 MTX is an antifolate entering cells through the reduced folate carrier (RFC-1)8 and activated to form methotrexate polyglutamates (MTX PGs) by folylpolyglutamate synthase.9,10 This γ-linked sequential addition of glutamic acid residues enhances the intracellular retention of MTX and promotes the sustained inhibition of amino-imidazole carboxamide ribonucleotide (AICAR) transformylase11 and thymidylate synthase (TS),12 the final steps in the de novo purine and pyrimidine biosynthesis, respectively. The result is an antiproliferative effect and a release of the anti-inflammatory agent, adenosine.13,14
The mechanisms underlying the large interpatient variability in the therapeutic response to MTX in patients with rheumatoid arthritis are not precisely established, but several lines of evidence suggest that the genetic makeup of the patient may have a significant role.15,16 Other reasons may more simply include lack of compliance and inadequate dosage. A recent study suggested that the MTX dosage was suboptimal in patients with rheumatoid arthritis,17 and a need for more rapid MTX dosage titration to individualise the MTX dose-maximising response was discussed.
It is now well established that patients with poor folate status have an increased risk of MTX gastrointestinal and haematological related side effects,18,19 and that folic acid supplementation can decrease the risk for the related toxicity of MTX.20–,22 However, as MTX may exert part of its pharmacological effects through folate depletion, it might be expected that folic acid supplementation would also decrease MTX efficacy. Although some studies have investigated the contribution of folate supplements to the effects of MTX,18,23 reports are controversial, and the effects of folate PG levels on MTX efficacy are not clearly established.
In this study we investigated the contribution of pharmacogenetic markers and of metabolite measurements (red blood cell (RBC) folate PGs and MTX PGs) to the clinical status of a large group of patients receiving MTX treatment.
PATIENTS AND METHODS
Study design
The study was cross sectional at three investigational American sites (Rheumatology Consultants, Knoxville, TN; Radiant Research, Daytona Beach, FL; Center for Rheumatology, Albany, NY). To be eligible, patients (⩾18 years) had to meet the revised criteria of the American Rheumatism Association for rheumatoid arthritis and to have received low dose MTX treatment for at least 3 months. We designed the study with MTX as the sole DMARD to minimise potential confounding factors introduced by other drugs. However, low dose corticosteroids (<10 mg/day) were allowed in the study. Folic acid supplements for the prevention of MTX induced side effects were also given. Institutional review boards approved the study for each site, and consent was obtained from each patient. Patient demographics were collected at the time of enrolment in the study. The blood was drawn in tubes containing EDTA and shipped overnight to our remote location in San Diego, CA.
Clinical status assessment
Patient clinical and demographic characteristics were collected on case report forms at the time of the single study visit. Each attending physician and each patient were unaware of the RBC MTX PGs, folate PGs, and pharmacogenetic indices throughout the entire study. A reduced 22 joint count (including metacarpophalangeal joints, proximal interphalangeal joints, wrists, and elbows) was employed. A physician’s global assessment of disease activity (10 cm visual analogue scale (VAS)) and a patient’s assessment of physical function using the modified Health Assessment Questionnaire (mHAQ) were also collected. In addition, a physician’s assessment of a patient’s response to MTX using a 10 cm VAS was used. The physician’s assessment of a patient’s response to MTX was scored from 0 (high response) to 10 (poor response).
Laboratory measurements
Red blood cell MTX PG concentrations (expressed as nmol/l RBCs) were measured using a high performance liquid chromatography fluorometry procedure with a post-column photo-oxidation technique.24 Our preliminary analyses showed that MTX triglutamate (MTX PG3) is the predominant polyglutamate species in RBCs from patients with rheumatoid arthritis and is strongly predictive of the total long chain MTX PG concentrations expressed as the sum of MTX PG3 + MTX PG4 + MTX PG5 (R2 = 0.92; n = 226, data not shown). Therefore, RBC MTX PG3 concentration was used as the marker of long chain MTX PG concentration (MTX PG3-5). RBC folate PGs (expressed as nmol/l RBCs) were measured using a radioassay (Biorad, USA). Common polymorphisms in reduced folate carrier (RFC-1/SLC191A1 G80A), AICAR transformylase (ATIC C347G), and thymidylate synthase (TSER*2/*3: 28 bp variable number of tandem repeats in the promoter region) were measured as described previously.25
Statistical analyses
The pharmacogenetic index is a cumulative composite index of individual genotypic components which maximises phenotype expression of low penetrance genetic polymorphisms. For ATIC C347G and TSER*2/*3 polymorphisms, a value of 0 was assigned to the ATIC 347CC or TSER*3/*3 genotype, a value of 1 was assigned to the ATIC 347CG or TSER*2/*3 genotype, and a value of 2 was assigned to the ATIC 347GG or TSER*2/*2 genotype. For RFC-1 G80A, a value of 0 was assigned to the RFC-1 80GG or 80GA genotype and a value of 1 was assigned to the RFC-1 80AA genotype. Thus the sum originating from each component (ATIC + TSER + RFC-1) was calculated and constitutes the pharmacogenetic index for the patient.
The analysis consisted of a multivariate linear regression (or univariate analysis, as appropriate), with clinical measures as dependent variables and RBC MTX PG levels, RBC folate PG levels, and the pharmacogenetic index as independent variables. All regression estimates were adjusted for the presence of rheumatoid factors, the MTX dose administered, the duration of the disease, and the concomitant administration of corticosteroids.
The physician’s assessment of a patient’s response to MTX was used to divide the population into good responders (VAS <2 cm) and poor responders (VAS >2 cm) to MTX. Poor responders were compared with good responders using a multivariate logistic regression analysis with RBC MTX PGs and pharmacogenetic index as independent variables. The probability of being a poor responder was derived from the logistic regression model. Odds ratio, and probability (p) are given with a 95% confidence interval (CI). Analyses involving group comparison were performed using the Kruskal-Wallis test as appropriate.
RESULTS
Patients’ characteristics
A total of 226 patients (165 (73%) women, 61 (27%) men) who were undergoing MTX treatment for more than 3 months were enrolled from December 2002 to November 2003 at three different American study sites (Tennessee site, 108 patients; Florida site, 53 patients; Albany site, 65 patients). The median weekly MTX dose administered was 15 mg, a total of 184 patients received folic acid supplementation (median 1 mg/daily), and 107 patients were receiving concomitant low dose corticosteroids. The physician’s assessment of a patient’s response to MTX was used to split the population of patients into responders (n = 112) and poor responders (n = 113) (one patient did not complete the VAS). Table 1⇓ summarises the patient demographic data.
Clinical characteristics of the 226 patients enrolled in the study
Median RBC MTX PG3 was 40 nmol/l (range <2–132 nmol/l; n = 226). The allelic frequency for RFC-1 80A was 42% (95% CI 38 to 47%), for ATIC 347G 35% (95% CI 30 to 39%) and for TSER*2 49% (95% CI 44 to 53%). The pharmacogenetic index ranged from 0 to 5 (median = 2; fig 1⇓). The population of patients consisted of 221 white subject and five black Americans. All polymorphisms were detected in these five patients (not shown). Higher MTX doses resulted in higher RBC MTX PG levels (univariate analysis, R2 = 0.14, p<0.001), and there was no association between the pharmacogenetic index and RBC MTX PG levels (univariate analysis, R2 = 0.001; p = 0.9).
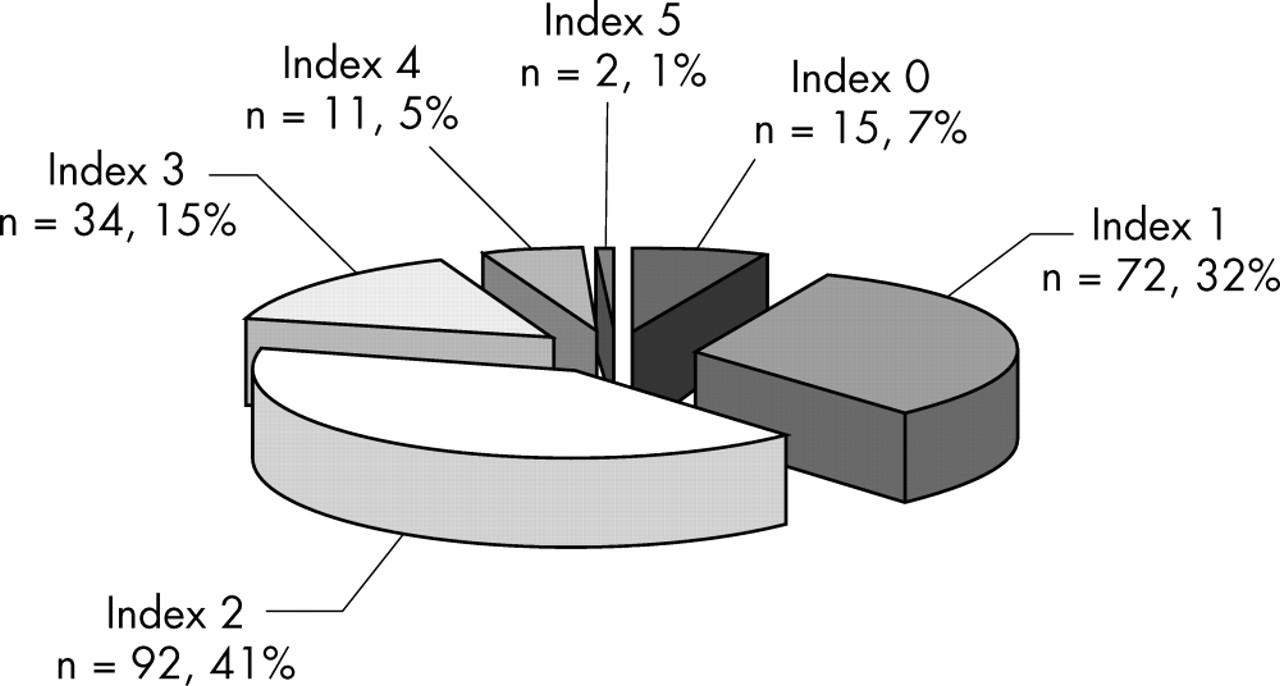
Pharmacogenetic index. The index ranged from 0 to 5 (median 2). Two patients had an index of 5, which corresponded to the presence of the three homozygous variant genotypes (value of 2 for ATIC 347GG + value of 2 for TSER*2/*2 + value of 1 for RFC-1 80AA). Fifteen patients had an index of 0, which corresponded to the presence of ATIC 347CC (value of 0), TSER*3/*3 (value of 0), and the presence of either the RFC-1 80GG or GA genotype (value of 0 for wild-type and heterozygous). The number of patients (percentage of the total group) is given for each index.
Association between RBC MTX PG levels, pharmacogenetic index, and clinical status
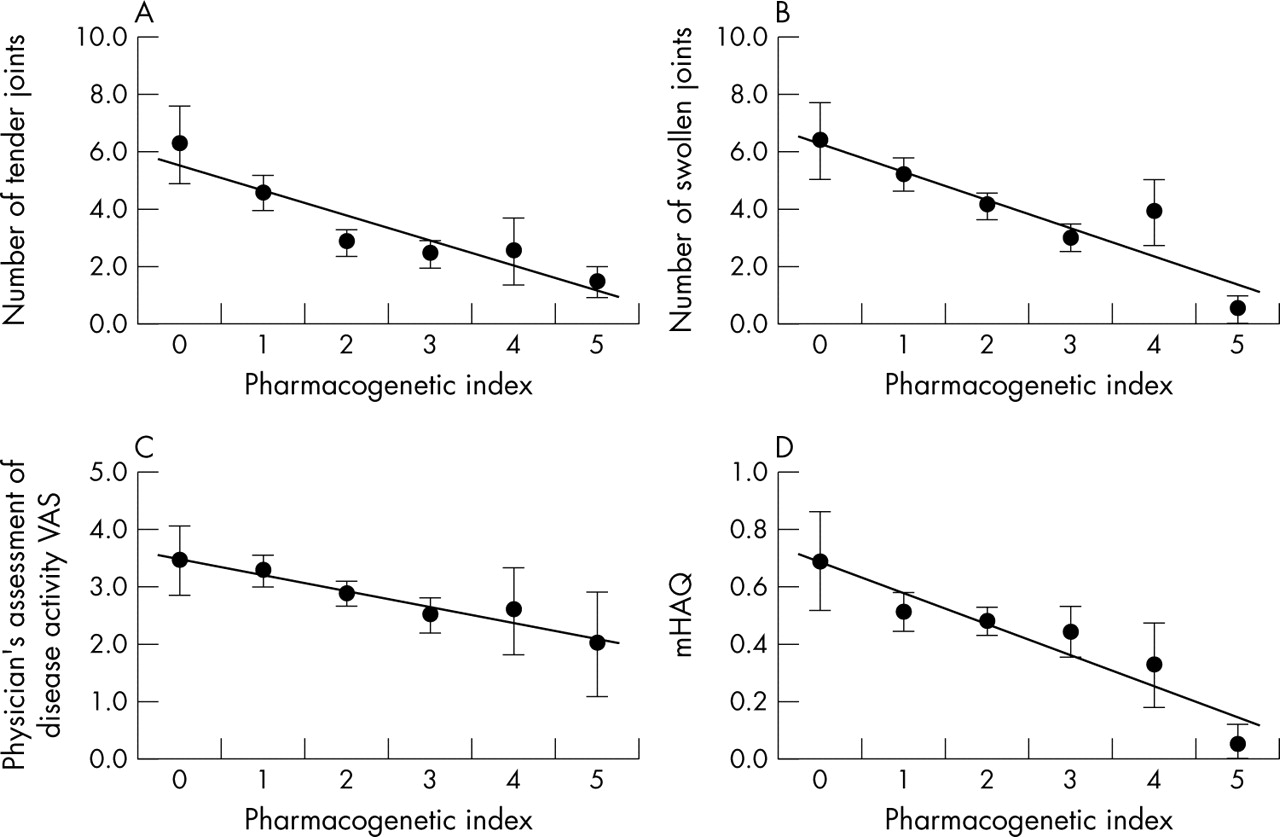
A multivariate regression analysis showed that RBC MTX PG levels and the pharmacogenetic index were associated independently with the number of swollen joints, tender joints, physician’s global assessment of disease activity, and mHAQ. Table 2⇓ presents the results. A poor clinical status (high number of tender and swollen joints, high disease activity, high mHAQ) was associated with low RBC MTX PG levels and low pharmacogenetic index (regression estimates <0; table 2⇓). Figure 2⇓ presents the association between the pharmacogenetic index (univariate analysis) and clinical status.
Multivariate linear regression of clinical measures with RBC MTX PG levels and pharmacogenetic measurements in the 226 patients

Association between the pharmacogenetic index and clinical status. In a univariate analysis, a lower pharmacogenetic index was associated with (A) a higher number of tender joints (p = 0.002); (B) a higher number of swollen joints (p = 0.003); (C) a higher physician’s global assessment of disease activity VAS (p = 0.032); and (D) a higher mHAQ (p = 0.047). Results are expressed as mean (SEM). The linear regression line is shown.
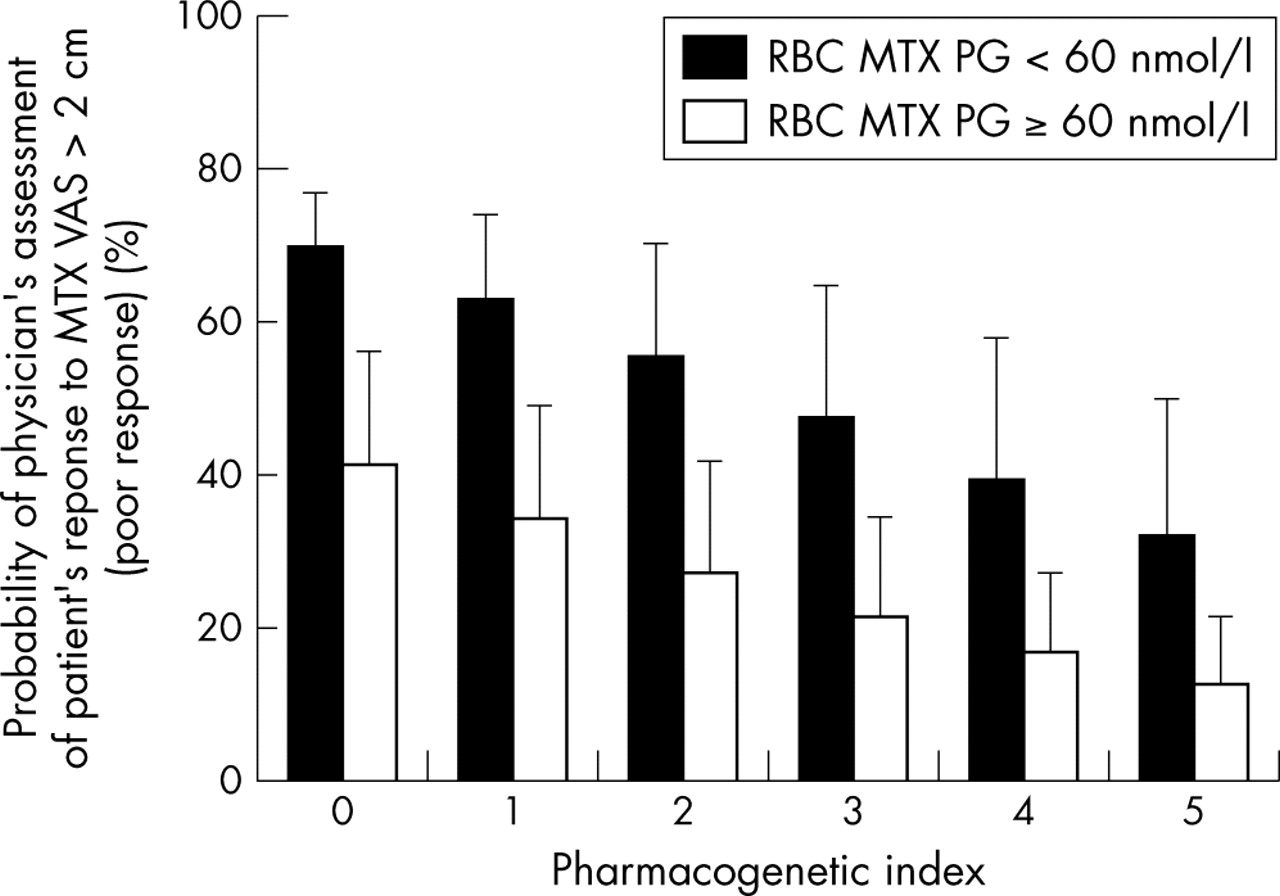
A multivariate logistic regression including RBC MTX PG levels and the pharmacogenetic index showed that MTX PGs <60 nmol/l and low pharmacogenetic index were associated with increased likelihood for a physician’s assessment of patient’s response to MTX VAS >2 cm (poor response; p<0.001 and p = 0.034, respectively). Figure 3⇓ presents the association between low RBC MTX PG levels, low pharmacogenetic index, and the likelihood of a poor response to MTX.

Association between MTX PGs, pharmacogenetic index, and the physician’s assessment of patient’s response to MTX. Patients having RBC MTX PG levels <60 nmol/l were 4.4-fold (95% CI 2.0 to 8.5; p = 0.0001) more likely to present a physician’s assessment of patient’s response to MTX VAS >2 cm (poor response). A lower pharmacogenetic index was also associated with a higher likelihood of physician’s assessment of patient’s response to MTX VAS >2 cm (p = 0.034). Probability (95% CI) is given.
Association between RBC folate PG levels and clinical status
Because blood for folate PG determination was not available in the first 50 patients enrolled at the Tennessee site, and was missing (insufficient blood volume) in five patients enrolled elsewhere, we evaluated the contribution of folate PGs to clinical status in a subset of 171 patients. The median level of RBC folate PGs was 1062 nmol/l (range 282–3162 nmol/l; n = 171). When higher folic acid doses were given, higher RBC folate PG levels were found (p = 0.009) (fig 4A⇓). After adjusting for MTX dose, duration of disease, presence of rheumatoid factors, administration of steroids, RBC MTX PG levels, and the pharmacogenetic index, a multivariate analysis showed that RBC folate PGs were not significantly associated with the physician’s global assessment of disease activity (p = 0.18) or the mHAQ (p = 0.79). However the multivariate analysis established that higher folate PG levels were associated with a higher number of tender joints (global R = 0.41; R2 = 0.166; estimate for RBC folate PGs = 0.0020 (0.0007); p = 0.003) and higher number of swollen joints (global R = 0.36; R2 = 0.129; estimate for RBC folate PGs = 0.0014 (0.0006); p = 0.028). Figure 4B⇓ illustrates the association between RBC folate PGs and the number of swollen and tender joints in a univariate analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between RBC folate PG concentrations and the number of tender and swollen joints. (A) Higher daily folic acid doses resulted in higher RBC folate PGs (p = 0.009). (B) In a univariate linear regression, higher folate PGs were associated with a higher number of tender (p = 0.002) and swollen joints (p = 0.006). The number of tender and swollen joints calculated from the univariate regression is given for folate PGs in the 10th (622 nmol/l), 25th (738 nmol/l), 50th (1062 nmol/l), 75th (1447 nmol/l), and 90th centile (1736 nmol/l) of the patient population. Bars represent values with 95% CI.
DISCUSSION
As far as we know, this is the first study to evaluate the contribution of pharmacogenomic and pharmacometabolic markers (RBC MTX PGs and folate PGs) to the effect of MTX in a large group of patients with rheumatoid arthritis. We previously suggested that polyglutamation of MTX with common polymorphisms in the folate/purine/pyrimidine pathways was associated with MTX effects in patients enrolled in a single study site.25 In the present report we have extended the enrolment to a larger cohort of patients at three study sites, and have also evaluated the contribution of RBC folate PGs to the effect of MTX.
We designed the study with MTX as the sole DMARD to minimise potential confounding factors introduced by other drugs. Because our study was cross sectional, we employed a new means of assessing a patient’s response to MTX treatment. We chose a VAS as it was felt that it would accurately reflect a clinician’s judgment of response in an appropriate dimension not captured by either of the standard outcome measures. This measure can be considered as a “real world” measure of the clinician’s judgment of overall response in a normal practice setting where American College of Rheumatology measures are not usually performed to evaluate treatment efficacy. The analysis showed that low RBC MTX PG levels were associated with poor clinical status, and that patients with MTX PG levels <60 nmol/l were fourfold more likely to have a poor response to MTX Although we cannot exclude the possibility that the maximum tolerated dose was achieved in poor responders having RBC MTX PG levels <60 nmol/l, it is worth noting that only 23% of the patients in the cohort reached this threshold.
Higher MTX doses resulted in higher MTX PG levels, but a higher MTX dosage tended to be associated with smaller effects (poor clinical status). Given our cross sectional study design, there are two hypotheses to explain these results. Firstly, MTX might have been increased during previous visits because the patient was not responding to MTX. These subjects would have had a level of RBC MTX PG which we suggest would have been low. Alternatively, some patients might have been responders at a low MTX dosage with the formation of a satisfactory level of MTX PG commensurate with a good response.
We have to acknowledge that there are some limitations in our cross sectional observational study design, and some caution should be exercised while interpreting the data. For example, the cohort of patients had been receiving MTX for an average of 5 years and we cannot extrapolate and generalise our data to patients starting MTX treatment. In addition, none of the patients enrolled had experienced toxicity requiring MTX withdrawal at the time of the visit, and therefore, MTX PG levels associated with toxicity are not known. However, this study lays the groundwork for a prospective longitudinal study aimed at confirming the value of RBC MTX PGs to establish whether the weekly dose of the drug is adequate to achieve the desired response. In fact, our preliminary analysis from such a prospective study appears to confirm our hypothesis and higher MTX PG levels seem to predict the ACR20 criteria during dose escalation.26 Moreover, a recent study suggests that increasing the MTX dose does not necessarily produce greater effects,7 and it will be important to determine whether MTX PG formation can reach saturation.
It is now well established that pharmacogenetics are useful for optimising treatment.15,16,27 In this study we evaluated the contribution of common polymorphisms in the folate (RFC-1 G80A), purine (ATIC C347G), and thymidylate synthase pathways (TSER*2/*3) to MTX effects. All these polymorphisms were previously associated with alteration in the response to MTX25,28 or with alteration in folate pools.29,30
Because the integrity of these pathways is critical for cellular homoeostasis, inborn errors that severely impair expression of these key enzymatic steps result in a high penetrance phenotype during childhood. For example, mutations that severely impair AICAR transformylase activity are associated with devastating neurological disorders,31 those affecting cellular folate uptake result in severe aplastic anaemia,32 and to our knowledge, no deficiency in thymidylate synthase has ever been reported. Consequently, only mutations associated with subtle alterations in these key enzymatic steps may be transmitted across generations (common polymorphisms), and are likely to exhibit low marginal phenotypic expression. Therefore, we calculated a composite index comprising individual genotypic components to maximise the pharmacogenetic contribution of these low penetrance polymorphisms.
The pharmacogenetic index contributed to MTX effects and lower index values resulted in diminished therapeutic efficacy. We speculate that lower indices are associated with subtle alterations in the folate, purine, and pyrimidine homoeostasis that result in poor sensitivity to MTX. Furthermore, both low RBC MTX PG levels and a low pharmacogenetic index were independently associated with poor clinical status and, therefore, both markers may be useful to stratify MTX dose to maximise effects. Of course, additional polymorphisms in other genes are likely to contribute to the effects of MTX, and hence could increase the modest variance explained by the genetic index in the study.
The vast majority of patients enrolled in the study received folic acid supplementation to prevent side effects induced by MTX. Because part of the effect of MTX may be mediated through depletion of folate cofactors, we suggested that folic acid supplementation could interact with MTX effects. Our analysis showed that RBC folate PG levels did influence the effects of MTX, with higher RBC folate PGs contributing to a higher number of tender and swollen joints. This first line of evidence suggests that folate PG levels may partially antagonise MTX effects. It would therefore appear that additional investigations into the rationale for folic acid supplementation with MTX treatment are appropriate.
In conclusion, these new data suggest that therapeutic drug monitoring of MTX treatment combining pharmacogenetic and intracellular metabolite measurements may be useful to optimise MTX treatment. Prospective studies will be necessary to confirm these findings and determine with certainty the predictive value of these markers.
Acknowledgments
We acknowledge Robert Barham and Gary Meyer for technical assistance and Brian Meshkin for discussion and interpretation of the results.
REFERENCES
Footnotes
Published Online First 27 January 2005
Competing interests: Thierry Dervieux, Diana Orentas Lein, and Katie Smith are employed by Prometheus Laboratories and have shares in the company. Joel Kremer, Daniel Furst, and Jacques Caldwell have received funds for clinical research from Prometheus Laboratories.
Ethics approval: Institutional review boards approved the study for each site, and consent was obtained from each patient.