Article Text

Abstract
Objective The 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) criteria for rheumatoid arthritis (RA) have been thoroughly studied for the test characteristics but it is unclear whether ‘2010 RA’ has a different phenotype than ‘1987 RA’ when assessing the severity of the disease course. Therefore this study compared two long-term disease outcomes.
Methods 1502 early arthritis patients that had no other diagnoses than RA or undifferentiated arthritis (UA) were studied on fulfilling the 1987 ACR criteria, 2010 criteria or both. The severity of joint damage was studied with yearly radiographs over 7 years. Achieving disease-modifying anti-rheumatic drug (DMARD)-free sustained remission was assessed over 10-years follow-up. Multivariate normal regression and Cox-proportional hazard regression were used, adjusting for age, gender and treatment.
Results 550 patients fulfilled the 1987 criteria, 788 patients the 2010 criteria and 489 both criteria sets. Patients fulfilling the 2010 criteria developed less severe radiological joint damage (p=0.023) and achieved DMARD-free sustained remission more often (HR=1.18 (0.93–1.50)) than patients fulfilling the 1987 criteria, though the latter was not statistically significant. All 1987+2010- patients were anti-citrullinated peptide antibody (ACPA)-negative. When also applying the radiologic criterion of the 2010-criteria, half of the 1987+2010− patients became 2010 criteria positive, but results on the long-term outcome remained similar.
Conclusions ‘2010 RA’ has a milder disease course than ‘1987 RA’. This may have important implications for basic scientific studies and clinical trials in RA.
- Early Rheumatoid Arthritis
- Outcomes research
- Arthritis
Statistics from Altmetric.com
Introduction
Presently rheumatoid arthritis (RA) can be classified according to either the 1987 ACR criteria or the 2010 American College of Rheumatology/European League against Rheumatism (ACR/EULAR) criteria. Both sets of criteria are being used and multiple studies have evaluated the performance of the 2010 criteria.1–5 A formal meta-analysis on the test characteristic is in progress (personal communication H Radner), but the current impression is that the 2010 criteria, compared to the 1987 criteria, are more sensitive and less specific in classifying RA.1 It is yet insufficiently clear whether the phenotype of RA is different when the disease is classified according to the 2010 criteria or the 1987 criteria. Several studies observed that some disease characteristics at disease onset of 2010 RA patients were milder than of 1987 RA patients.2–5 Some authors reported that erosions at baseline and after 2 years are more often present in 1987 RA compared to 2010 RA2 ,4–6 Together, these data lead to the presumption that RA defined according to the 2010 criteria is milder in nature than that defined according to the 1987 criteria, but there is insufficient data to draw definite conclusions on this matter. Particularly, there are no studies comparing the long-term outcome of RA patients when RA is classified either to the 1987 criteria or the 2010 criteria. The most characteristic hallmarks of RA are progression of joint damage and disease persistence. We aimed to compare these two long-term disease outcomes in relation to the classification of RA and performed the present longitudinal study to this end.
Methods
Patients
Early arthritis patients included in the Leiden Early Arthritis Clinic Cohort7 between 1993 and May 2011 were studied. Inclusion took place when arthritis was confirmed at physical examination and symptom duration was <2 years. At the first visit, patients and rheumatologists completed questionnaires, physical examination was performed, and serum and radiographs were taken. Follow-up visits were performed yearly. For further description, see reference 7. The treatment differed for different inclusion periods. Patients included between 1993 and 1995 were initially treated with NSAIDs, patients included between 1996 and 1998 were initially treated with chloroquine or sulfasalazine and patients included after 1999 were promptly treated with methotrexate or sulfasalazine. The inclusion period was used as a proxy for the applied treatment strategy in the analyses.
Of all 2748 included early arthritis patients, patients that at first visit had a clear diagnosis other than RA or undifferentiated arthritis were excluded (n=839), which is in line with the 2010 criteria. Patients that were treated in randomised clinical trials were excluded (n=397) as the treatment of these patients was more tightly controlled and the medications used more potent, affecting the disease course. Patients with a follow-up <1 year were also excluded (n=10). Thus, 1502 patients were studied (figure 1A) and classified on fulfilling the 1987 ACR criteria and/or the 2010 ACR/EULAR criteria.
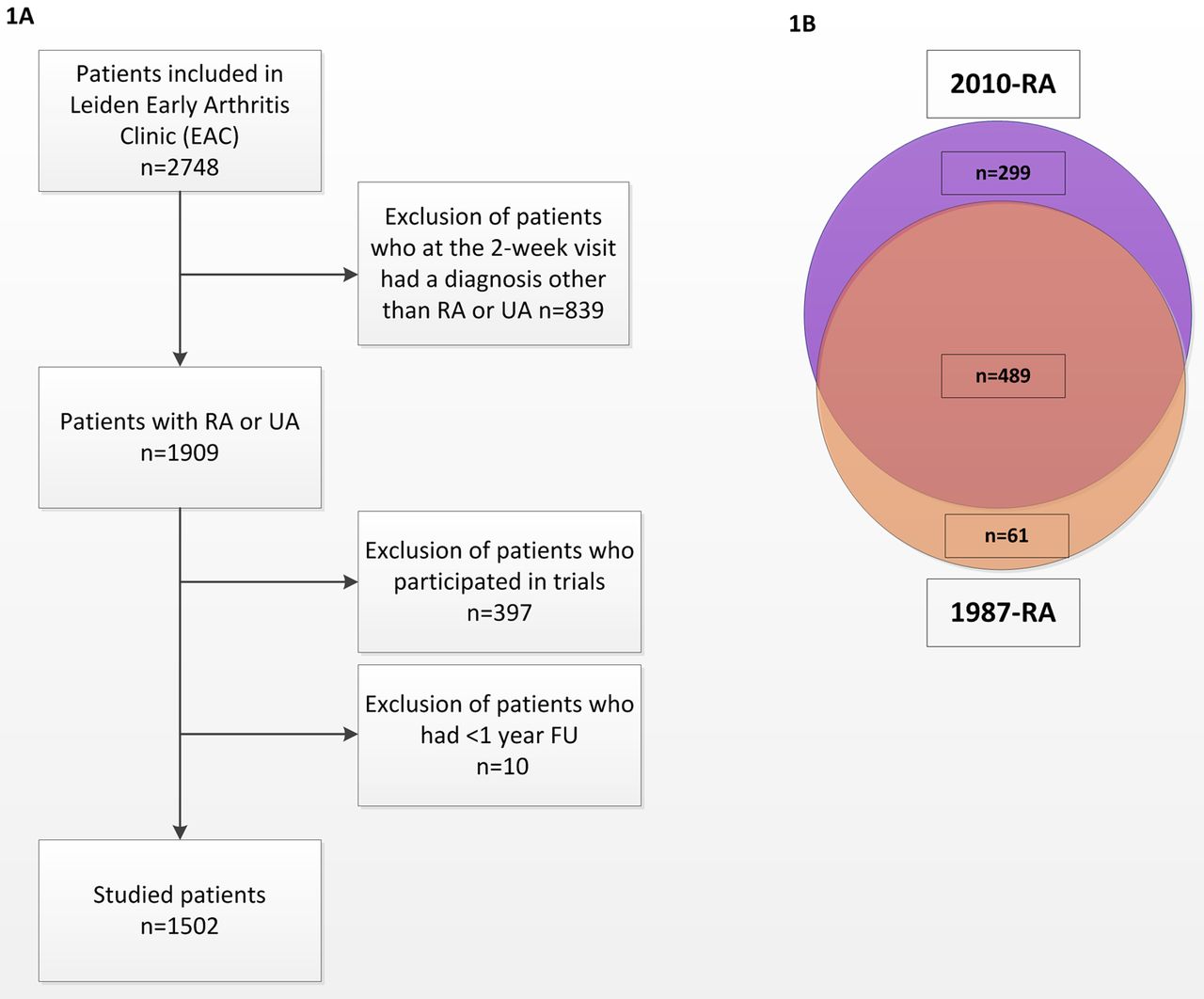
Flowchart of patient selection (A) and number of patients studied that fulfilled the 1987− and/or 2010 classification criteria at baseline (Bf (A) The 2010 American College of Rheumatology/European League against Rheumatism (ACR/EULAR) criteria state that these criteria should not be applied in patients that have other diagnoses. For this reason, patients that at the 2-week visit (when the results of laboratory and radiological evaluations were known) had clear rheumatologic diagnoses were excluded. Patients that were treated according to trial protocols were excluded as well, as treatment strategies of these patients differed from the other patients. However, the trial patients were included in a sensitivity analysis. (B) Of the 1502 patients studied, 489 fulfilled both criteria sets for rheumatoid arthritis (RA) at the 2-week visit. 299 patients fulfilled only the 2010-criteria and 61 patients fulfilled only the 1987-criteria. 714 patients fulfilled none of the criteria sets for RA.
Outcome
Two outcome measures were studied. The first was the severity of radiological damage during 7 years of follow-up. Hand and feet x-rays were taken at baseline and yearly thereafter and scored according to the Sharp-van der Heijde method by two readers with known time order, blinded to clinical data. Intraclass-observer correlation coefficients within the readers were 0.91 and 0.87 and between the two readers, it was 0.89.
The second outcome was achieving a disease-modifying anti-rheumatic drug (DMARD)-free sustained remission during 10 years of follow-up. Remission was defined as the sustained absence of synovitis (by physical examination) after discontinuation of DMARD-therapy. Synovitis had to be absent for the entire period of follow-up and at least during 1 year8; in general, these patients were also discharged from the outpatient clinic. Patients that achieved such a remission but relapsed (n=13) were included in the non-remission group. This stringent definition of remission is the best possible outcome of RA as it approximates ‘cure’; it is the opposite of disease persistency. Medical files of all patients were studied on remission, and this was determined until the 5 April 2012.
Statistical analyses
Analyses on remission were done using a Cox proportional hazard regression analysis.8 Analyses on joint destruction were done using a multivariate normal regression analysis as described previously, including all radiographs in one analysis and taking advantage of serial measurements.9 Another advantage is that it allowed to study all patients, also in case of missing radiographs, preventing selection bias that would be induced by a completers-only analysis.10 All analyses were adjusted for age, gender and treatment strategy. First the long-term outcomes of patients with RA according to the 1987 criteria and RA according to the 2010 criteria were compared. In this analysis, patients that fulfilled both criteria sets were included in both groups. Subsequently all patients were split in three groups (1987+2010−, 1987−2010+ and 1987+2010+) and analyses repeated. SPSS V.20.0 was used. p Values <0.05 were considered significant.
Results
Baseline characteristics
Of the 1502 patients studied, 550 patients fulfilled the 1987 criteria, 788 patients the 2010 criteria by having ≥6 points and 489 patients fulfilled both criteria (figure 1B). Table 1 presents the baseline characteristics. Overall, no large differences were seen between 1987 RA and 2010 RA, but 2010+ patients experienced less morning stiffness than 1987+ patients (median 60 vs 90 min) and had slightly lower C-reactive protein (CRP) levels. When comparing the three subgroups, it was observed that all 1987+2010− patients were anti-citrullinated peptide antibody (ACPA)-negative.
Baseline characteristics of patients classified with rheumatoid arthritis (RA) according to either the 1987 and/or the 2010− criteria
Comparison of 1987 and 2010 RA
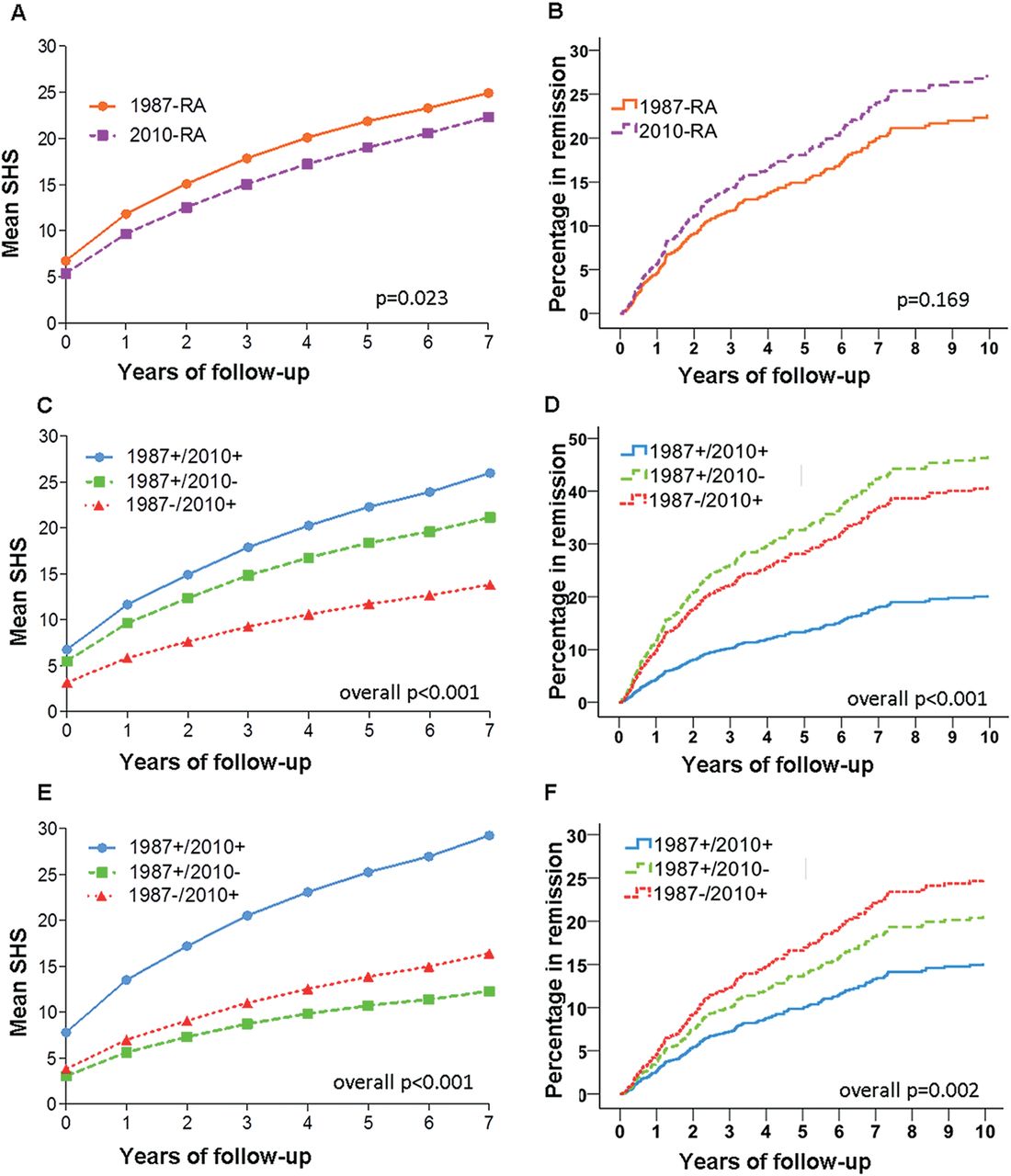
RA patients according to the 2010 criteria had less severe radiological joint destruction over 7 years of disease than RA patients classified using the 1987 criteria (p=0.023, figure 2A). When evaluating DMARD-free sustained remission, more remission was achieved in 2010+ RA-patients than in 1987+ RA-patients, though this difference was not statistically significant (HR=1.18(0.93–1.50) p=0.17, figure 2B).

{kind=link}
{kind=link}
Comparison of long-term outcomes of rheumatoid arthritis (RA) according to fulfilment of the 1987− and/or 2010 classification criteria for RA. f All analyses were adjusted for age, gender and treatment. Depicted in (A, C and E) are the predicted (by the multivariate normal regression model) Sharp-van der Heijde scores during 7-years of follow-up. Depicted in (B, D and F) are the percentage of patients achieving disease-modifying anti-rheumatic drug (DMARD)-free sustained remission (A and B) Comparison of patients fulfilling the 1987 criteria and patients fulfilling the 2010 criteria. (C and D) Comparison of patients fulfilling either one or both criteria sets for RA. (E and F) Comparison of patients fulfilling either one or both criteria sets for RA, after also adjusting for the presence of ACPA. (C–F) Presented are the overall p values when comparing three groups. For comparisons of subgroups with the 1987+2010+ patients as reference the results were for C: 1987+/2010+ vs 1987+/2010− p=0.35, 1987+/2010+ vs 1987−/2010+ p<0.001. D:1987+/2010+ vs 1987+/2010− p<0.001, 1987+/2010+ vs 1987−/2010+ p<0.001: E: 1987+/2010+ vs 1987+/2010− p=0.14, 1987+/2010+ vs 1987−/2010+ p<0.001. F:1987+/2010+ vs 1987+/2010− p=0.21, 1987+/2010+ vs 1987−/2010+ p<0.001.
Subanalyses
Subsequently, the RA patients were stratified in three groups (1987+2010−, 1987−2010+, 1987+2010+) and the analyses were repeated. As presented in figure 2 C,D, 1987+2010+ RA patients developed more severe joint destruction and achieved DMARD-free sustained remission less often than patients fulfilling one criteria set for RA (p<0.001 for both outcomes and comparison of three groups). Moreover, when analysing these subgroups in more detail, the severity of joint damage was not different between the 1987+2010+ and 1987+2010− patients (p=0.35) but differed between the 1987+2010+ and 1987−2010+ patients, p<0.001, figures 2C,D). Interestingly, 1987+2010− RA patients achieved DMARD-free sustained remission most frequently. However, this small subgroup contained only ACPA-negative patients. When the analysis was also adjusted for ACPA, this effect was no longer present (figure 2F).
Thus far, the 2010 criteria were applied using the point system. When applying the radiological criterion for RA-specific erosiveness (≥3 erosive joints)11 ,12 in addition to the point system, 30 of the 61 1987+2010− RA were now 2010-criteria positive. All analyses on joint damage and remission were repeated; this did not influence the results (see online supplementary figures 1 and 2).
Finally, all analyses were repeated including the 397 patients that were treated in clinical trials, yielding similar results as described above (data not shown).
Discussion
The present study evaluated the long-term outcome of patients classified to the 1987 criteria or the 2010 criteria and observed a statistically significant difference in the severity of joint damage and a non-significant difference with regard to disease persistency. For both outcomes, patients classified as RA using the 2010 criteria had a less severe disease course. Thereby the present data suggest that RA, when using the most recent classification criteria, has become a milder disease.
This observation might fit within the observations that the 2010 classification criteria have a lower specificity than the 1987 criteria and can be positive in patients that later on have other diagnoses (associated with a less destructive course).1 ,5 ,6 ,13–15 Alternatively, patients fulfilling the 2010 criteria, in particular, the 1987−2010+ patients, may simply represent a milder set of patients. The milder outcome observed was not due to an earlier diagnosis and earlier treatment initiation, as the 2010 criteria were applied after the follow-up data were obtained.
In our study, we did not observe large differences in baseline characteristics, though the 1987 RA patients experienced more morning stiffness than the 2010 RA patients. This may be a consequence of morning stiffness being part of the 1987 criteria. Adding morning stiffness as an additional adjustment factor to the analyses did not give different results (data not shown); hence the findings done were not driven by this baseline difference.
The 2010 criteria were derived with MTX-usage as outcome; by using this outcome, some level of circularity could not be prevented. Advantages of the two outcomes used here is that they are independent of any set of classification criteria, and therefore, do not suffer from circle reasoning.
A limitation is that patients were treated. Ideally, the present study question was evaluated in patients that were not treated over many years, as this completely represents the natural disease course. We excluded patients that were treated in clinical trials and studied only patients treated according to routine care. Nonetheless, the treatment strategies used in these patients had changed over time; therefore analyses were adjusted for these differences in treatment. Importantly, the proportion of 1987+ and 2010+ patients was similar for the different inclusion periods (data not shown). Moreover, including patients who were treated in clinical trials did not influence the findings.
All 1987+2010− patients were ACPA-negative, which is in line with another recent report.16 When the radiological criterion of the 2010 criteria was also applied, half of this group of patients became 2010-criteria positive. This supports the relevance of the radiological criterion as the frequency of this misclassification reduced.
In conclusion, the present longitudinal study showed that RA classified according to the 2010 criteria has less severe joint destruction and is less often persistent than RA classified according to the 1987 criteria. This may have important implications, both for basic scientific studies and randomised clinical trials in RA.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure 1
- Data supplement 2 - Online figure 2
Footnotes
Handling editor Tore K Kvien
LEB and JABvN contributed equally.
-
Contributors LEB, JABvN and AHMvdH contributed to the acquisition of the data, the analysis and interpretation of the data and drafting of the manuscript. LYH contributed to the acquisition of the data. AHMvdH, DPCdR and TWJH revised the article for important intellectual content. All authors gave final approval of the version to be published.
-
Funding This work is supported by a grant of the Dutch Arthritis Foundation (Reumafonds), by The European Community Seventh Framework Programme FP7 Health-F2-2008-223404 (Masterswitch) and by the IMI JU funded project BeTheCure, contract no 115142-2. The work of AHMvdH-vM is supported by a Vidi-grant of the Netherlands Organisation for Scientific Research.
-
Competing interests None.
-
Ethics approval Medical ethics committee LUMC.
-
Provenance and peer review Not commissioned; externally peer reviewed.