Article Text

Abstract
Objectives We performed a systematic review and meta-analysis of randomised controlled trials (RCTs) of psoriatic arthritis (PsA) to examine the effect of tumour necrosis factor (TNF) blockers on radiographic progression, and to determine whether treatment combining TNF blocker with methotrexate (MTX) was superior to TNF-blocker monotherapy.
Methods We systematically reviewed articles published up to December 2012 in Embase and Medline, and from the two last EUropean League Against Rheumatism (EULAR) and American College or Rheumatology (ACR) meetings. The primary endpoint was the proportion of patients with no radiographic progression (non-progressors) at treatment week 24 (defined by change in modified total Sharp score (mTSS) ≤0.5). The Mantel–Haenszel method was used to estimate ORs and 95% CIs of the effect of TNF blockers (with or without MTX) versus placebo (with or without MTX). Statistical heterogeneity was assessed by χ² test.
Results The search retrieved 207 articles; 5 (1110 patients) met the meta-analysis criteria. For patients receiving TNF blockers, 494/584 (84.5%) were considered non-progressors at treatment week 24 vs 362/526 (68.8%) receiving placebo (OR 2.68 (95% CI 1.99 to 3.60) p<0.001), without significant heterogeneity (I2=3%; p=0.39). Only three RCTs provided data on potential additional efficacy of MTX: two did not find significant difference, one suggested a benefit of combined therapy.
Conclusions For patients with PsA, control of structural damage is better at week 24 with TNF blockers than placebo. Due to the limited data, we were unable to conclude on the potential additional effect of MTX on structural damages.
- Psoriatic Arthritis
- DMARDs (biologic)
- TNF-alpha
- Methotrexate
Statistics from Altmetric.com
Introduction
Psoriatic arthritis (PsA) is a frequent inflammatory arthritis occurring in 0.3–1% of the general population.1 It has variable clinical presentation (articular and dermatological features, peripheral arthritis, enthesitis, inflammatory back pain) and disease course. One-third of patients with psoriasis will have joint involvement, usually several years after dermatological signs.2 Even if PsA is considered less aggressive than rheumatoid arthritis (RA), recent studies suggested that it can lead to severe morbidity and disability.3 This situation may lead to physical and psychosocial disability and higher mortality than for the general population.4 ,5
Treatment of PsA remains largely empirical, and the rationale for various strategies was frequently extrapolated from efficacy data for RA. The proinflammatory cytokine, tumour necrosis factor α (TNF-α) has a key role in the pathogenesis of the disease,6 ,7 and the efficacy of biological agents that neutralise TNF has been demonstrated in several studies of PsA, mainly versus placebo.8 However, radiographic assessments have never been primary endpoints of clinical trials. Moreover, we lack evidence of whether methotrexate (MTX), sulfasalazine or leflunomide can slow structural PsA progression. Kingsley et al9 even suggested that MTX had no clinical effect in PsA in a controlled study comparing placebo in 221 patients. By contrast, in RA, with its incomplete response to synthetic disease-modifying antirheumatic drugs (DMARDs) alone, combining biologics with synthetic DMARDs is the ‘gold standard’ because of clinical and radiological efficacy.10 ,11 In patients with PsA, the effect of concomitant therapy with MTX, and the roles of the biologic and conventional DMARDs on clinical and radiographic efficacy, is still unclear. Recently, in an observational study, among 440 PsA patients treated by TNF-blockers combined or not with MTX, Fagerli et al12 did not notice an additional effect of the combined therapy on patient and physician global assessments and functional indexes, after 3 months of treatment. However, they found a better drug survival after 1 and 2 years in the combined therapy group.
We performed a systematic review with meta-analysis of reports of randomised controlled trials (RCTs) of TNF blockers and placebo to determine whether TNF blockers affect radiographic evidence of PsA progression, and to determine whether their combination with MTX is superior to TNF-blocker monotherapy.
Methods
Search method
We performed a systematic review of articles published up to 1 December 2012 in Medline (via PubMed), Embase and databases for the 2010, 2011 and 2012 European League Against Rheumatism and American College of Rheumatology annual meetings. Keywords included ‘psoriatic arthritis’, ‘methotrexate’, ‘biological therapy’, ‘tumor necrosis factor-alpha’, ‘adalimumab’, ‘certolizumab’, ‘etanercept’, ‘golimumab’ and ‘infliximab’, as well as exclusion terms, such as ‘ankylosing spondylitis’ or ‘rheumatoid arthritis’. (Details on the exact keywords used in the literature research are available in online supplementary figure S1). The search was limited to articles published in English, RCTs, clinical trials and meta-analyses of patients older than 18 years. We chose articles of studies reporting the efficacy of TNF blockers versus placebo on PsA and including data on radiographic evidence of disease progression.
We first screened abstracts, then chose relevant full-text articles. The reference lists of selected articles were manually searched to identify additional relevant reports.
Data extraction
Two investigators (RG and GM) independently extracted the following information by using a predefined data collection form. The following methodological features were collected: blinding, intention-to-treat analysis or not, and number of participants who completed follow-up. The Jadad scale13 was applied, which contains two questions for randomisation and masking, and one question evaluating the reporting of withdrawals and dropouts. Each question entails a yes or no response option. In total, five points can be awarded, with higher scores indicating higher quality. For each trial, patient characteristics, treatment modalities (type of TNF blocker, dosage, MTX use), control group characteristics, follow-up duration, evaluation criteria (clinical and radiographic scores) and main findings were collected. Disagreements were determined by consensus by the two investigators. We attempted to contact authors for missing radiographic data.
Endpoints
We extracted radiographic data and found that all the selected articles used the Sharp method modified for PsA.14 The modified total Sharp score (mTSS) has been used to evaluate radiographic evidence of damage in RA.15 The method has been adapted to PsA, including distal interphalangeal hand, wrist and feet joints, and was demonstrated to be sensitive enough to assess treatment effect over a short time.14
The primary endpoint was the proportion of patients without radiographic evidence of disease progression at treatment week 24 (non-progressors). Secondary endpoints were the proportion of non-progressors at week 48, and mean change in mTSS at week 24. Non-progressors were defined by change in mTSS≤0.5 from baseline to 24 or 48 weeks, because it seemed more clinically relevant to study ‘non-progressors patients’ than the mean change in mTSS, and because this value and this cut-off were used in all the selected articles. Moreover, we evaluated the respective role of MTX and biologics in radiographic disease progression if data were available.
Statistical analysis
The Mantel–Haenszel method was used to estimate ORs and 95% CIs (shown in forest plots) for TNF blockers (with or without MTX) versus placebo (with or without MTX) for RCTs of infliximab (IFX), etanercept (ETN), adalimumab (ADA) and golimumab (GLM). Statistical heterogeneity was assessed by the χ² Q test. A p<0.05 was considered statistically significant. All the analyses were performed with RevMan 5.1 Software (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011).
Results
The literature search retrieved 207 articles; we examined 67 articles on the basis of the title and abstract, and finally retrieved the full text for five articles that met the meta-analysis criteria.16–20 The selection of articles is in figure 1. For articles concerning GLM, we separately analysed data for the 50 and 100 mg doses because the final dosage had not yet been selected.
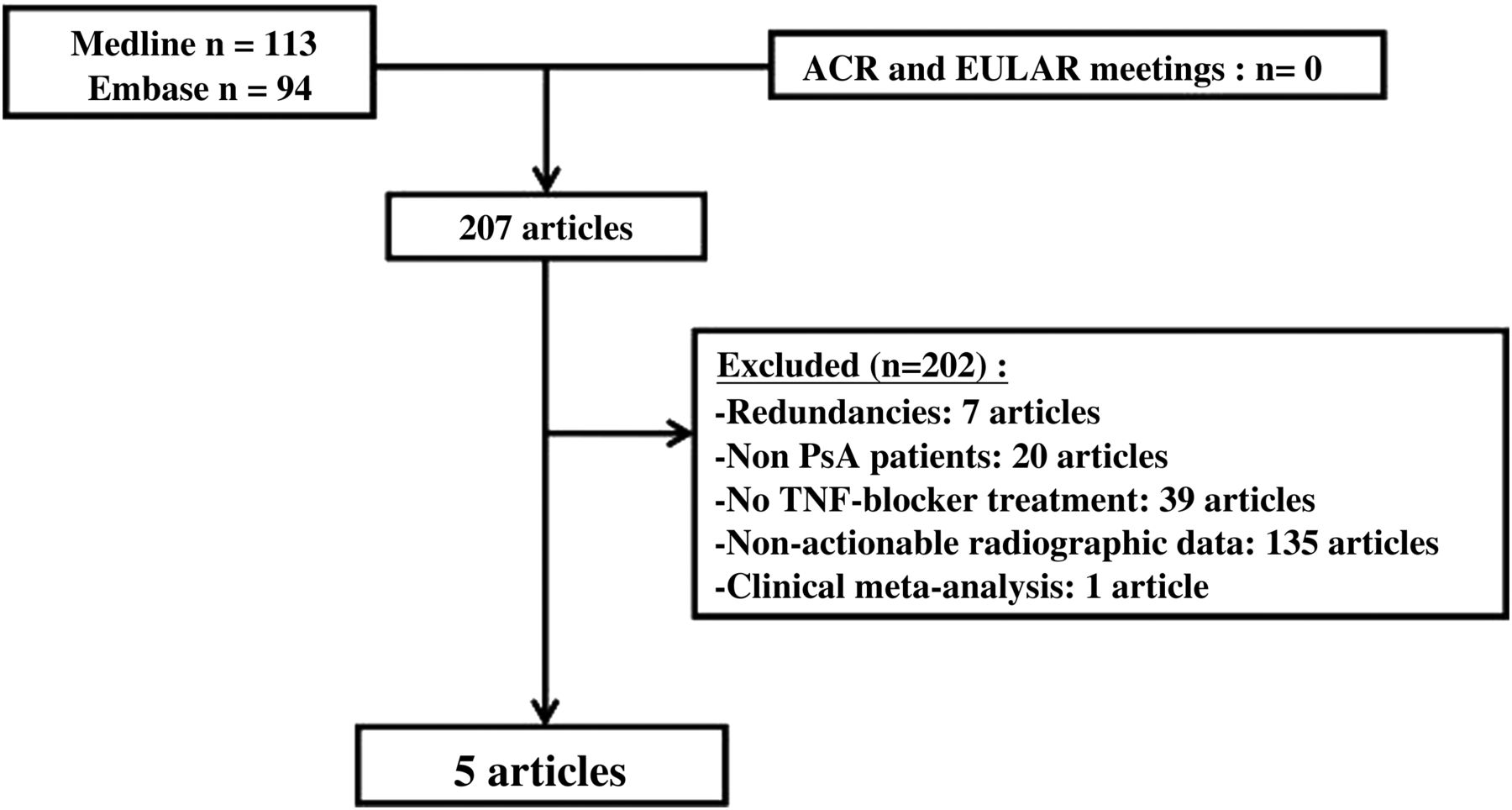
Flow chart of the selection of the articles.
The studies involved 1110 patients, 584 receiving TNF blockers with or without MTX, and 526 placebo with or without MTX. No study compared a TNF blocker with a synthetic DMARD. Patient characteristics and radiography results are in table 1. The two groups for each study were comparable in terms of age, disease duration and MTX use at baseline.
Meta-analysis of randomised controlled trials of psoriatic arthritis (PsA), characteristics of included patients and major endpoints
In total, 494/584 (84.5%) of patients receiving TNF blockers for PsA were considered non-progressors at week 24 as compared with 362/526 (68.8%) receiving placebo (OR 2.68 (95% CI 1.99 to 3.60), p<0.001), without significant heterogeneity (I2=3%, p=0.39) (figure 2). At week 24, patients in both groups started receiving TNF blockers: at week 48, one group had received TNF blockers for 24 weeks, and the other for 48 weeks. Thus, at week 48, results again favoured TNF blockers (OR 2.42 (1.57 to 3.71); I2=0%; p=0.91) (figure 3).
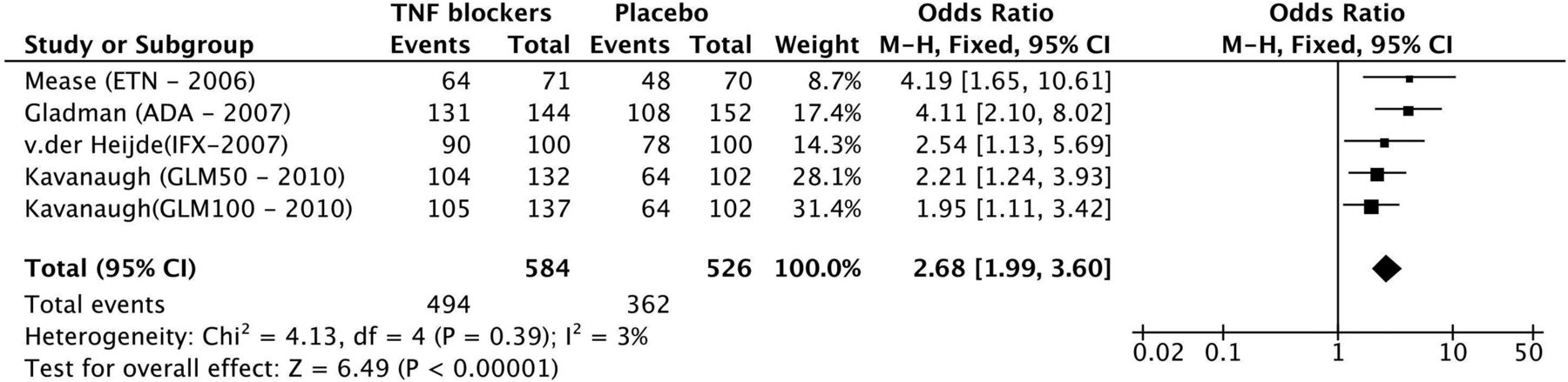
Risk estimates of non-progressors reported in randomised controlled trials of PsA patients receiving tumour necrosis factor blockers after 24 weeks of treatment.

Risk estimates of non-progressors reported in randomised controlled trials of PsA patients receiving tumour necrosis factor blockers after 48 weeks of treatment.
Among 533 patients receiving TNF blockers versus 454 receiving placebo at 24 weeks in three studies (four comparisons because of two dosages in the GLM study), the mean change in mTSS was lower with the TNF blocker than placebo (OR −0.69 (−1.12 to −0.27)), with significant heterogeneity (I2=76%; p=0.006) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean progression of modified total Sharp score reported in randomised controlled trials of PsA patients receiving tumour necrosis factor blockers after 24 weeks of treatment.
Only a few data were available for TNF blocker therapy combined with MTX. No RCT directly compared the three groups of treatment: TNF blockers combined with synthetic DMARDs and each therapy alone. No study evaluated the effect of biologics added to MTX on radiographic and clinical outcomes in PsA. Mease et al,16 in a subanalysis, found no difference in structural progression between two groups (ETN treatment alone vs ETN with MTX) after 24 weeks, but no statistical analysis was available. Gladman et al,17 in a subanalysis, found no difference in radiographic disease progression between ADA alone and ADA with MTX (mean difference in mTSS at 24 weeks −0.2±1.17 vs −0.2±1.59). More interestingly, in the same study, radiographic disease progression was similar in the placebo group controlling for MTX use (1.2±3.01 with MTX vs 0.9±2.99 without MTX; 78 vs74 patients). Van der Heijde et al19 noted that the median differences between IFX plus MTX versus MTX plus placebo in changes in radiographic scores were greater for subgroups of patients with features of more severe disease, including baseline MTX use. Concerning GLM,20 after 24 weeks of treatment, in a subgroup analysis of patients receiving MTX at baseline, non-progressors were less frequent in patients receiving placebo versus those receiving 50 or 100 mg GLM (32/53 (60.4%) vs 55/65 (84.6%) p=0.003, and 52/67 (77.6%) p=0.041, respectively). For patients not receiving MTX at baseline, non-progressors were not statistically different among three groups (32/49 (65.3%) in placebo group vs 49/67 (73.1%) in 50 mg GLM group, p=0.364 versus placebo, and 53/70 (75.7%) in 100 mg GLM group p=0.216 vs placebo). The authors suggested that MTX could enhance the GLM effect on inhibiting radiographic disease progression.
Discussion
Because of the persistence of inflammation, PsA can lead to joint destruction as great as in RA.3 Although some radiographic features of PsA are characteristic and differ from those in RA, especially in terms of the location of affected joints and concurrent destructive changes and bone proliferation, PsA may have the same overall progressive course as RA. Therefore, treatment should be started before structural damage occurs, to avoid disability. Treatment, such as TNF blockers, must be evaluated among these patients to determine how to slow down or even stop the disease course.
We performed a systematic review and meta-analysis of RCTs of PsA to examine the effect of TNF blockers on radiographic evidence of disease progression. A second objective was to determine whether treatment combining TNF blockers with MTX was superior to TNF-blocker monotherapy. Results from five articles (1110 patients) showed that the four TNF blockers led to better control of radiographic disease progression than placebo. This structural effect looks in the same range between drugs, with the limitations inherited by these kinds of indirect comparisons.
Most scoring methods for the assessment of joint damage were developed and validated for RA. We chose articles using the mTSS because it is a well-proven method for scoring radiographic damage, and is used in most clinical trials of RA and PsA. Nevertheless, further work is needed to validate the van der Heijde hand and foot modification of the Sharp method in a large PsA population; address its face validity, reproducibility and implications for predicting further structural damage, and compare its performance with that of other methods proposed to assess radiographic features unique to PsA.21 We defined non-progressors patients on mTSS (increase in mTSS ≤0.5 between baseline and 24 and 48 weeks); a 0.5 mTSS change included most of the change attributable to reader error. An alternative would have been to use the smallest detectable change (SDC)23—the smallest change needed in the mTSS to exceed the amount of change attributable to reader error. Nevertheless, the SDC is calculated within each study, and its value depends on the radiographic reader experiment. Moreover, the SDC was not reported in all articles, and thus, could not be pooled. When reported, the SDC was small (eg, 1.88 of the mTSS in the study concerning ADA23) and did not influence the results, which favoured TNF blockers after 24 weeks of treatment.
We considered both doses of GLM (50 and 100 mg) in our comparisons. At present, the 50 mg dosage seems to be the only one marketed.
Our secondary endpoints were comparisons at 48 weeks of treatment. Indeed, at 48 weeks, the non-biologic group had received 24 weeks of placebo, then 24 weeks of treatment up to week 48, whereas the TNF-blocker group had received 48 weeks of treatment. Thus, the placebo-controlled period lasted only 24 weeks, which may undervalue the difference between the two groups, perhaps in favour of the non-biologic group, at week 48. Other long-term comparisons, for more than 48 weeks without any biologic treatment, could have been of interest, because disease progression determined radiographically is a long process in the disease outcome, but no data were available.
Considering the characteristic16 and van der Heijde19 had more males than females in their TNF-blocker group than the non-biologic group (57% vs 45% and 71% vs 51%, respectively) as compared with the other RCTs. However, male sex does not seem to be associated with a worse prognosis in PsA patients.4 The baseline mTSS was higher in the three TNF-blocker arms (ETN, ADA, and GLM) than the non-biologic arm (table 1). The TNF-blocker group could be thus considered as having more severe disease than the non-biologic group in these RCTs. This difference could lead to undervaluing the difference observed between the two groups, possibly in favour of the non-biologic group, but final results at 48 weeks still favoured TNF blockers. By contrast, in the van der Heijde et al trial,19 the baseline mTSS was higher in the non-biologic than IFX group (30.3 vs 39.1). Concerning the patients, the diagnosis of PsA was not defined precisely by the ClASsification criteria for Psoriatic Arthritis (CASPAR),24 which are now commonly used for diagnosis of PsA. Thus, we cannot exclude that some RA patients with psoriasis could have been inappropriately included in these PsA RCTs.
Evaluation of MTX combined with TNF blockers on the structural effect in PsA was difficult because of limited data. Clinical trials of RA compared MTX plus TNF blockers versus MTX or TNF blockers alone, and concluded a substantial effect of the combination on clinical and radiographic outcomes.10 ,11 Similar trials are not available in PsA, and only post hoc analysis attempted to evaluate the efficacy of the combination without evidence of the add-on value of this combination.
Recently, Gladman et al25 reported as an abstract a randomised controlled trial where the structural effect of certolizumab (CZP) was evaluated among 409 PsA patients. Significantly more patients were non-progressors (defined by mTSS<0) in both CZP groups (200 mg and 400 mg) compared with placebo (respectively, 83.3% and 76.3% vs 34.6%, p<0.001 for both CZP groups vs placebo). We did not include these results in our meta-analysis because of limited information in this preliminary report.
Our meta-analysis of RCTs of PsA revealed that the TNF blockers ETN, IFX, ADA and GLM all led to better control of structural damages than non-biologic therapy after 24 and 48 weeks of treatment. The role of the therapy combined with MTX could not be clearly determined because of limited available data. More studies are required to propose a strategy for treating early PsA as in RA.26 ,27 Such studies should investigate risk factors of radiographic disease progression such as C-reactive protein level and baseline radiographic scores to prevent disability in this frequent disease that can be as severe as RA.
Acknowledgments
We wish to thank Abbott who provided logistic support in the organisation of sessions about the implementation of a meta-analysis, and remained independent of the collection, analysis and interpretation of data.
References
Supplementary materials
Lay summary
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
Footnotes
Handling editor Tore K Kvien
-
Contributors All authors have taken part in drafting the article or revising it critically for important intellectual content and final approval of the version to be published. RG, GM, CL, JM and BC conceived this review and meta-analysis. RG and GM reviewed the literature. RG, GM, TB, CL and BC conducted interpretation and analysis. RG, GM and BC contributed to drafting the manuscript. CL and JM reviewed the manuscript.
-
Competing interests BC has received honorarium from Merck and Pfizer. JM and BC have received grant funding from Pfizer.
-
Provenance and peer review Not commissioned; externally peer reviewed.