Article Text

Abstract
Objective To assess the rates and explore predictors of microscopic gut inflammation in a cohort of patients with axial and peripheral spondyloarthritis (SpA).
Methods Ileocolonoscopy was performed in 65 patients with axial and peripheral SpA from the Gent Inflammatory Arthritis and spoNdylitis cohorT. Histopathological analysis and scoring were performed by an experienced pathologist.
Results Overall, 46.2% of the patients with SpA showed microscopic gut inflammation. In axial SpA, the following parameters were independently associated with gut involvement: male sex (OR=8.9, p=0.035); high disease activity measured by the Bath Ankylosing Spondylitis Disease Activity Index (OR=2.05, p=0.032); restricted spinal mobility measured by the Bath Ankylosing Spondylitis Metrology Index (OR=1.94, p=0.009); and younger age (OR=0.85, p=0.013). No clear association was found for human leucocyte antigen-B27 status, presence of peripheral arthritis, enthesitis, uveitis, psoriasis, intake of non-steroidal anti-inflammatory drugs and family history of SpA. The prevalence of gut inflammation in non-radiographic axial SpA and ankylosing spondylitis was comparable.
Conclusions The prevalence of microscopic gut inflammation in SpA remains unaltered over time. Younger age (shorter symptom duration), progressive disease, male sex and higher disease activity are independently associated with microscopic gut inflammation in axial SpA.
- Spondyloarthritis
- Ankylosing Spondylitis
- Inflammation
Statistics from Altmetric.com
Introduction
It has been recognised for a long time that ∼60% of all patients with spondyloarthritis (SpA) show microscopic inflammatory gut lesions, a fraction of which evolve into Crohn's disease. However, since the first report of these findings (1984–1985),1 the field of SpA has experienced major developments, among them the possibility to decrease the gap between onset of symptoms and diagnosis, particularly by the introduction of MRI of the sacroiliac joints (SIJs). As a consequence of the introduction of the new Assessment of SpondyloArthritis international Society (ASAS) classification criteria,2 it is now possible to identify early in the disease course patients with non-radiographic axial SpA. In addition, improved hygiene has resulted in altered exposure to, and colonisation by, micro-organisms (hygiene hypothesis).3 This has led to a shift in pathologies, possibly suggesting that the prevalence of mucosal inflammation may have declined.
This study was designed to ascertain whether the prevalence of gut involvement in SpA has changed. Furthermore, we aimed to develop a predictive model for microscopic gut inflammation in axial SpA using clinical and biological parameters.
Methods
Study population
The Gent Inflammatory Arthritis and spoNdylitis cohorT is a prospective observational cohort in which patients diagnosed with SpA and classified according to the ASAS criteria are prospectively followed. Ileocolonoscopy was performed in 65 consecutive patients, naive to tumour necrosis factor (TNF) blockers. None of the patients reported suggestive gastrointestinal complaints for, or had a previous diagnosis of, inflammatory bowel disease (IBD).
History and investigations
All patients were interviewed about their disease history, their family history of SpA, drug intake and smoking habits. The use of non-steroidal anti-inflammatory drugs (NSAIDs) was defined as continuous use at the time of endoscopy or within 1 week before. Before ileocolonoscopy, all patients underwent a complete clinical examination. Radiographs of the SIJs, the spine and involved joints were obtained. MRI of the SIJs was performed in 37 out of 49 patients diagnosed with axial SpA. In the other patients, diagnosis and classification was made on the basis of x-ray and/or human leucocyte antigen (HLA)-B27 positivity. The results were interpreted by a group of rheumatologists and a musculoskeletal radiologist (LJ). Laboratory tests included inflammatory parameters, HLA-B27 determination and peripheral blood cell examination. All patients were asked to complete the following questionnaires: the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI) and Visual Analogue Scale (VAS) global disease activity.
Ileocolonoscopy
For each patient, 4–14 biopsy samples were taken of ileum and colon, with a median number of six per patient. The biopsy specimens were classified by an experienced pathologist, who was unaware of macroscopic findings and the patient's diagnosis.
Histological classification
Two histological types of microscopic gut inflammation can be distinguished in SpA: acute and chronic as previously reported.4 This classification refers to the observed morphological characteristics, not the disease duration. Similarly to previous ileocolonoscopic studies,5 a diagnosis of chronic inflammation was made whenever a biopsy specimen featured chronic lesions, regardless of acute inflammation in other fragments.
Acute lesions
The normal mucosal structure is preserved and changes are limited to infiltration of the epithelium with neutrophils and eosinophils, crypt abscess formation, and infiltration of the lamina propria with polymorphonuclear cells.
Chronic lesions
The normal mucosal architecture is disturbed, with crypt distortion, villous blunting and fusion, increased mixed lamina propria cellularity, and presence of basal lymphoid aggregates.
Statistical analysis
Data were analysed using SPSS V.19. A univariate analysis was performed to compare all demographic, clinical and biochemical variables between the patients with and without microscopic gut inflammation. Normally distributed numeric variables were tested by an independent-samples t test. In the case of a skewed distribution, the Mann–Whitney U test was performed. For categorical variables, the Fisher exact test was used. Multivariate binary logistic regression analysis (backward selection) was performed to estimate the associations between patient and disease characteristics that are potential predictors of microscopic gut inflammation. Model quality was checked by calculating the area under the receiver operating characteristics curve (ROC AUC) and the Hosmer–Lemeshow test. For all analyses, p<0.05 was considered significant. Analyses were restricted to individuals with complete data.
Results
Patients
Sixty-five patients were included in the study, of which 49 were diagnosed with axial SpA (ASAS classification criteria) with or without peripheral manifestations, and 16 were diagnosed with peripheral SpA without axial involvement. Baseline characteristics of all patients are presented in table 1.
Baseline demographic and clinical characteristics
Prevalence of microscopic gut inflammation in axial and peripheral SpA
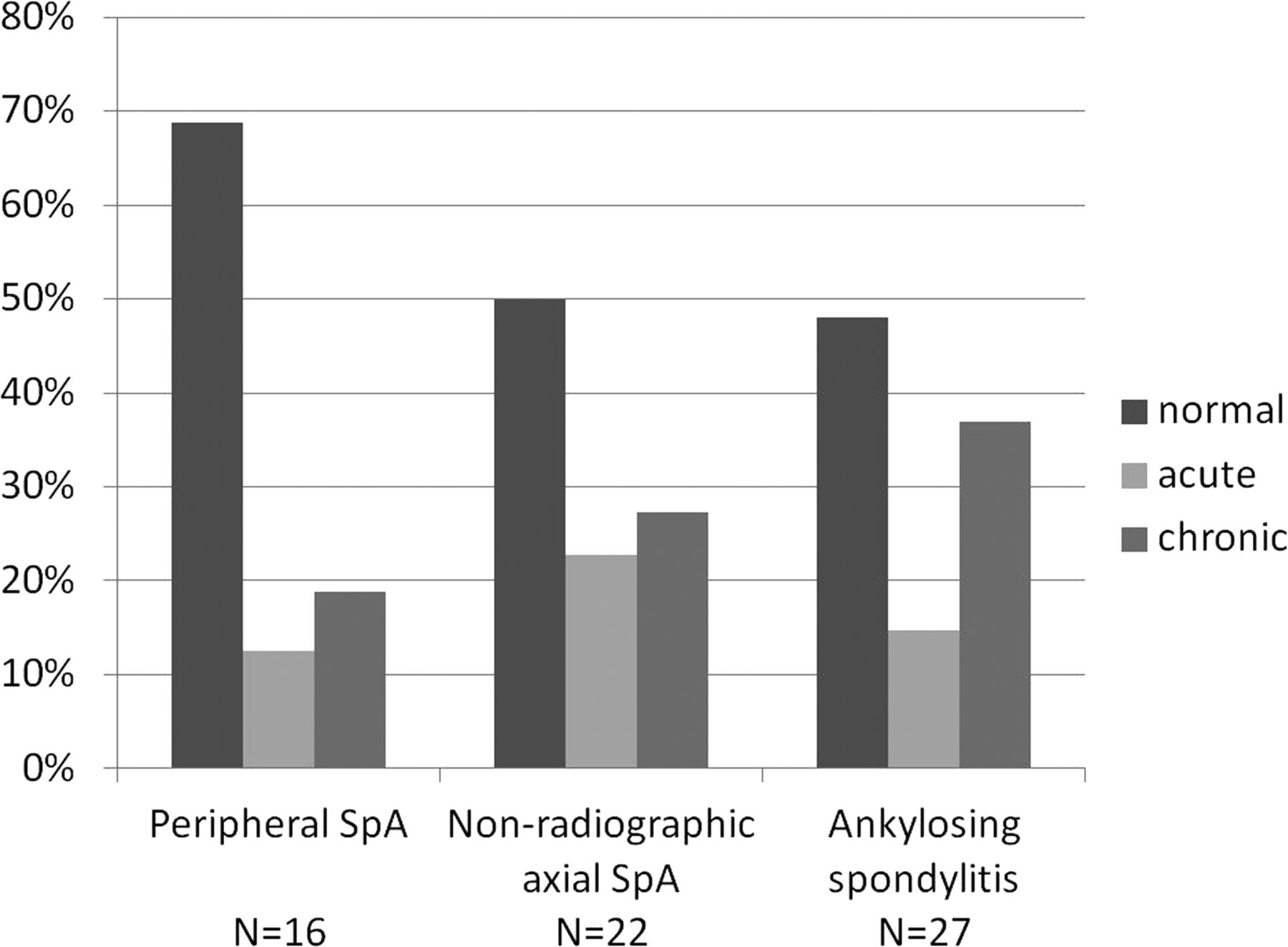
Overall, 46.2% of the patients showed microscopic gut inflammation. The acute type of inflammation was present in 16.9%, and the chronic type in 29.2% of patients (figure 1). Figure 2 shows the distribution according to classification. The inflammation was located in the ileum in 50% of cases, in the colon in 23.3%, and in 26.7% both ileum and colon were affected. There was a strong similarity between the microscopic and macroscopic findings. All but two patients with a normal microscopic appearance also had a perfectly normal macroscopic aspect of the mucosa. Eighteen out of 30 patients with microscopic inflammatory involvement showed macroscopic abnormalities, ranging from erythema, oedema and friability of the mucosa to ulcerations, granulation and cobblestoning.
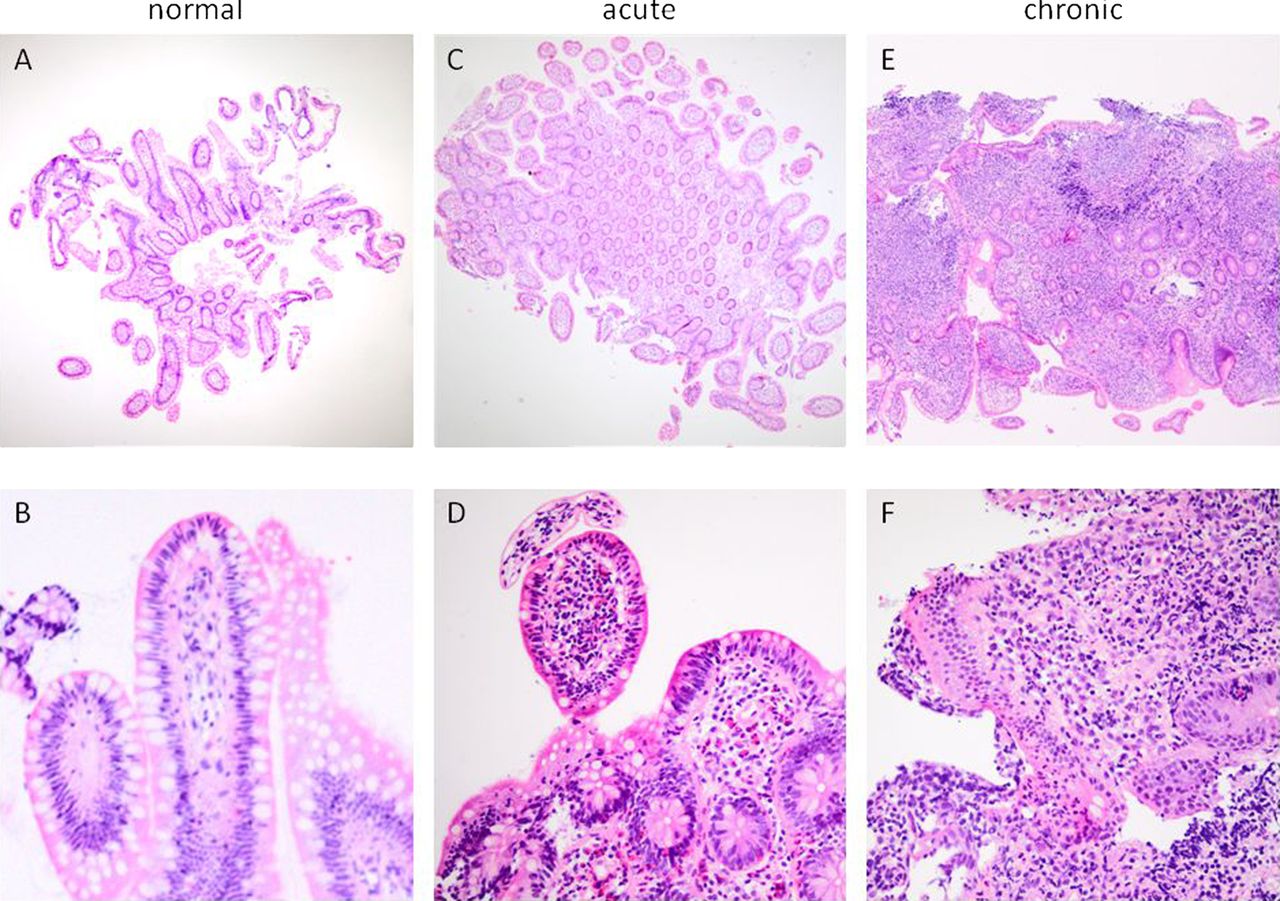
Different patterns of ileal biopsy findings in SpA patients. (A) Normal histology of ileal mucosa featuring slender villi and straight crypts; absence of inflammatory cell infiltrates (H&E; original magnification ×4). (B) Higher magnification emphasising lack of inflammatory cell infiltration in villus epithelium (H&E; original magnification ×20). (C) Focal active inflammation in mucosa with preserved architecture of villi and crypts (H&E; original magnification ×4). (D) Increased amount of granulocytes in villus and crypt epithelium with well-preserved epithelium (H&E; original magnification ×20). (E) Chronic dense inflammatory cell infiltration of lamina propria with crypt and villus alterations (H&E; original magnification ×4). (F) Active granulocytic infiltration of villus epithelium and chronic dense lymphoplasmocytic cellular infiltrate in the lamina propria (H&E; original magnification ×20). This figure is only reproduced in colour in the online version.
{kind=link}
{kind=link}
Prevalence of gut inflammation according to classification.
Prediction of microscopic gut inflammation in axial SpA
No significant differences were observed in the univariate analysis (see online supplementary data table 1) comparing patients with axial SpA with or without microscopic gut inflammation.
We next conducted a multivariate analysis. For 45 of the 49 patients with axial SpA, complete data were available. Using a backward procedure, we included five variables in our model. The model is presented in table 2. Bootstrap validation showed no indication for overfitting and confirmed the results found in our original model (data not shown). Male sex and a higher BASDAI were independently associated with microscopic gut inflammation (OR 8.9, 95% CI 1.18 to 67.37 and OR 2.05, 95% CI 1.06 to 3.95, respectively), as well as higher Bath Ankylosing Spondylitis Metrology Index (BASMI) (OR 1.94, 95% CI 1.18 to 3.19) and younger age (OR 0.85, 95% CI 0.75 to 0.97). Our final model has a sensitivity of 81.8% and a specificity of 78.3% for detecting microscopic gut inflammation in axial SpA. No indication for multicollinearity was found.
Multivariate analysis of microscopic gut inflammation in axial SpA
No clear association was found for HLA-B27 status, NSAID use, smoking habits, presence of peripheral arthritis, enthesitis, family history of SpA, uveitis and psoriasis.
Discussion
In this cohort of patients with axial and peripheral SpA, nearly half showed microscopic gut inflammation. A high frequency in patients with different forms of SpA was originally discovered in the 1980s by Mielants et al5 and has been validated by several other investigators.6–8 Almost 30 years later, new classification criteria enable us to identify early axial and peripheral SpA. This study thus provides substantial new insights into the link between gut inflammation, symptom duration and disease activity in patients with axial SpA.
Over the past few years, striking progress has been made in our understanding of SpA and IBD. Nevertheless, the exact role of microscopic gut inflammation in SpA has not been determined, nor has the link with outcome measures been investigated. We have focused on clinical and biological parameters predictive of the presence of microscopic gut inflammation in patients with axial SpA; future work will address predictive parameters in peripheral SpA. In axial SpA, we found younger age (equivalent to shorter symptom duration), male sex, higher disease activity (BASDAI) and higher BASMI to be independently associated with microscopic gut inflammation.
We selected BASDAI for inclusion in the final model instead of Ankylosing Spondylitis Disease Activity Score (ASDAS) because we found that the value of ASDAS in predicting gut inflammation was explained by the BASDAI component, not by the C-reactive protein (CRP) component (see multivariate analysis in online supplementary data table 2). Both younger age and shorter symptom duration (with a correlation of 0.47) had a significant influence on the odds of having microscopic gut inflammation. We included age in the final model, as it was a more accurate predictive parameter (ROC AUC and Nagelkerke R2). The fact that CRP did not show a significant association with gut inflammation was surprising. However, a recent study by Soliman et al showed no significant association between CRP and disease activity measured by bone marrow oedema on MRI of the SIJ.9 Another study by Machado et al also found weak to moderate correlations between CRP and MRI scores.10 Future research will address the association between gut inflammation and the quantification of bone marrow oedema on MRI.
Despite the putative link between NSAID use and bowel inflammation, the association between NSAIDs and IBD flares cannot be considered definitive, because, in the only two available randomised controlled, double-blind trials in patients with quiescent IBD receiving a cyclo-oxygenase 2-selective inhibitor (celecoxib/etoricoxib) or placebo,11 ,12 no significant difference in the frequency of disease exacerbation was found. Considering microscopic gut inflammation, Mielants and Veys13 observed an equal prevalence among patients receiving NSAIDs and patients not receiving anti-inflammatory drugs. In the present study, we controlled for intake of NSAIDs in our predictive model. However, no association was found with microscopic gut inflammation in either the univariate or the multivariate analysis.
Prospective follow-up studies on SpA revealed microscopic gut inflammation to be an important risk factor for developing ankylosing spondylitis14: evolution of non-ankylosing spondylitis SpA to full-blown ankylosing spondylitis was always associated with gut involvement at disease onset, and remission of joint inflammation was associated with disappearance of gut inflammation. The present study identified shorter symptom duration and higher disease activity to be associated with microscopic gut inflammation, suggesting its important pathogenic role. Male patients overall show more rapid radiographic progression,15 which supports our finding that male sex is a major risk factor for underlying microscopic gut involvement. Future prospective studies are needed to assess the real impact of microscopic gut inflammation on the long-term outcome of early axial SpA as defined by the new criteria, and to evaluate the impact of more aggressive therapeutic strategies, including early intervention trials based on the presence or absence of microscopic gut inflammation.
The acute and chronic types of gut involvement were pooled in this analysis, as it can be expected that the development of chronic bowel inflammation occurs through a transition phase, in which inflammation evolves from an acute to a chronic state. This has been termed the transition model.16 In line with this, no significant differences in baseline characteristics were found between the two groups. The higher prevalence of chronic gut inflammation found in ankylosing spondylitis compared with axial SpA supports this transition model and indirectly validates the new ASAS criteria for axial SpA. Overall, our results underscore the role of bowel inflammation in SpA.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
-
Contributors LVP, FEVdB, PJ, PC, MDV, HM, DE: study conception and design. LVP, PJ, EG, MDV, HP: acquisition of data. LVP, CC, RC, LJ, DE: analysis and interpretation of data.
-
Funding This study was supported by a grant from the Clinical Research Funding of Ghent University Hospital to LVP.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study protocol was approved by the ethics committee of Ghent University Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.