Article Text

Abstract
Background Patients with rheumatoid arthritis (RA) are at increased risk of cardiovascular disease. Lipid changes related to inflammation have been described in RA. Tumour necrosis factor α (TNFα) inhibitor (TNFi) treatment is effective in controlling inflammation and decreasing the number of cardiovascular events.
Objective To assess the change in lipid levels with TNFi treatment in patients with RA by systematic review and meta-analysis.
Methods A Medline search was performed for articles published up to March 2011. Reports describing values for total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides (TGs), atherogenic index (AI) and apolipoprotein B/A (apoB/A) collected before and after TNFi initiation were included. Data were analysed according to short-, mid- and long-term treatment. Statistical analysis of pre–post data was performed by comprehensive meta-analysis. A random effects model was used when there was evidence of heterogeneity.
Results The search retrieved 32 articles, of which 13 prospective before/after studies were analysed. Long-term TNFi treatment was associated with increased levels of HDL (+0.27 mmol/l, p<0.0001) and TC (+0.27 mmol/l, p=0.03), whereas LDL levels and AI remained unchanged. After long-term treatment, TG levels increased (+0.28 mmol/l, p<0.001) and apoB/A decreased (−0.3, p<0.0001).
Conclusion The presumed cardioprotective effects of TNFi in RA do not seem to be explained by quantitative lipid changes since long-term treatment has no effect on LDL levels or on AI. Increased HDL levels could have some beneficial effects, but this needs to be confirmed by prospective studies with long-term follow-up.
Statistics from Altmetric.com
Introduction
Cardiovascular mortality is increased in patients with rheumatoid arthritis (RA) compared with the general population,1 and is the leading cause of increased mortality.2 The risk of myocardial ischemia in patients with RA is about 1.6 compared with the general population and is similar to the magnitude of risk with type 2 diabetes mellitus.3 4 The chronic systemic inflammatory state in RA may enhance atherogenesis beyond the presence of traditional risk factors such as diabetes, smoking, obesity and dyslipidaemia.
The notion that inflammation and atherogenesis are linked in RA is supported by the decrease in cardiovascular mortality in patients receiving adequate disease-modifying antirheumatic drug (DMARD) therapy.5 6 Published reports on lipid abnormalities in RA are few and contradictory. However, inflammation seems to be responsible for a decrease in high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol levels.7 8 Despite the decrease in LDL-cholesterol, the level of small dense LDL, a particle believed to be proatherogenic, increases during inflammation.9 Thus, the pattern of lipid metabolism during inflammation is proatherogenic and believed to contribute to atherosclerosis, especially in chronic inflammatory diseases such as RA. Tumour necrosis factor α (TNFα), a proinflammatory cytokine involved in pathogenesis of RA, has pronounced effects on lipoprotein metabolism by decreasing lipoprotein lipase activity and liver metabolism.10 TNFα inhibitors (TNFi) can reduce disease activity and structural damage in RA and could also diminish the increased cardiovascular risk associated with RA by attenuating systemic inflammation associated with atherogenesis.11 12
This study aimed to assess changes in lipid levels after short-, mid- and long-term treatment with TNFi in patients with RA by systematic review of the literature and meta-analysis.
Methods
Search strategy
We searched Medline via PubMed for articles published up to March 2011 and abstracts of 2009 and 2010 European League Against Rheumatism (EULAR) and American College of Rheumatology (ACR) congresses. The MeSH terms used were (‘Lipids’ (Mesh) or ‘Dyslipidaemia’ (Mesh)) and ‘Arthritis, Rheumatoid’ (Majr: NoExp) and (‘TNFR-Fc fusion protein’ (substance name) or ‘Infliximab’ (substance name) or ‘Adalimumab’ (substance name) or ‘AntiTNF’ or ‘Golimumab’ or ‘Etanercept’ or ‘Certolizumab’). No limits were added. The full text of relevant abstracts was retrieved. Two independent rheumatologists analysed each article. The inclusion of articles was determined by consensus.
Inclusion criteria
To be selected for analysis, a study had to meet all of the following criteria:1 designed for studying the effects of TNFi on lipid levels2 and to have values before and after treatment of at least one variable among triglycerides (TGs), total cholesterol (TC), HDL, atherogenic index (AI, corresponding to the TC/HDL ratio), LDL, apolipoprotein A (apoA), apolipoprotein B (apoB) or apoB/A.
Given the characteristics of the included studies, the classic scales for evaluating the methodological strength of the studies was adapted only for some items. The items extracted were taken from three quality assessment scales: the Newcastle Ottawa Scale; the quality assessment of studies of diagnostic accuracy included in systematic reviews; and the Cochrane Collaboration tool for assessing risk of bias. The results of this quality assessment are available in the online supplement.
Data extraction
Values of TC, LDL, HDL, TG, AI, apoA, apoB and apoB/A before and after initiation of TNFi treatment were extracted. The data were analysed according to the effects at three time-points: short-term (2–6 weeks), mid-term (12–16 weeks) and long-term (22 –52 weeks). No reported data between these time-points were found. For studies with two values for the same time-point as previously described (eg, data at 24 and 52 weeks), only the latest data were used.
Statistical analysis
Statistical analysis of pre–post data was performed by comprehensive meta-analysis. Analysis of standardised mean differences was carried out using a fixed or random effects model. A p value <0.10 was considered to suggest statistical heterogeneity and prompted random effects modelling. The percentage heterogeneity in the study results beyond chance was determined by the I2 statistic, with a value of 0% indicating no heterogeneity and larger values indicating increased heterogeneity. Publication bias was assessed by the Egger test and represented graphically by funnel plots of the standard difference in means versus the standard error; p<0.10 was considered statistically significant. The Trim and Fill analysis for publication bias involved the Duval and Tweedie method; p<0.05 was considered statistically significant in all analyses.
These meta-analysis methods enabled determination of heterogeneity and publication bias. However, these methods do not include all studies because of missing data at some time-points. Moreover, some studies could not be included because the exact p value was missing. In order to confirm the robustness of the results by evaluating the missing data (missing time-points and exact p values), a multivariate linear mixed model was secondarily used and the results obtained by the two methods were compared.
Results
The search retrieved 38 articles.13,–,50 Sixteen articles were excluded because they were off the topic, six were excluded because they were reviews/comments, one article was excluded because it pooled data for RA and psoriatic arthritis and two articles were excluded because of missing p values and/or CIs. Thus, 13 articles were included in the meta-analysis (figure 1).15 22 24 27 29 32,–,36 39 43 45 Sub-meta-analyses were performed for each factor of interest.

Flowchart.
Study characteristics
Table 1 shows the characteristics of the studies included in the meta-analysis. Ten articles reported on patients receiving only monoclonal antibodies, one with etanercept only and two with 47% and 21% of patients receiving soluble receptors. The follow-up varied from 2 weeks to 2 years, and the number of patients from 19 to 149. The 13 articles reported on a total of 702 patients.
Characteristics of included studies
Long-term study outcomes
HDL-cholesterol
The effect of TNFi on the HDL-cholesterol level was documented in six articles (6–12 months, 338 patients; figure 2). Hetero- geneity was significant (I2=77.7%, p value for heterogeneity (p-H)=0.001; and I2=72.3%, p-H=0.003) and was mainly explained by inclusion of the findings of Jamitski et al for soluble receptors.15 Controlling for this study resulted in non-significant heterogeneity (5 studies, 226 patients, I2=36%, p-H=0.18). The HDL-cholesterol level increased significantly with TNFi therapy (+0.27 mmol/l, p<0.0001) but, in the study by Jamnitski et al, the HDL-cholesterol level decreased, which may explain why this study was responsible for the heterogeneous results. When random effects modelling was used, including the results of Jamnitski et al, the HDL-cholesterol level increased with long-term treatment, although not significantly (+0.20 mmol/l, p=0.07).
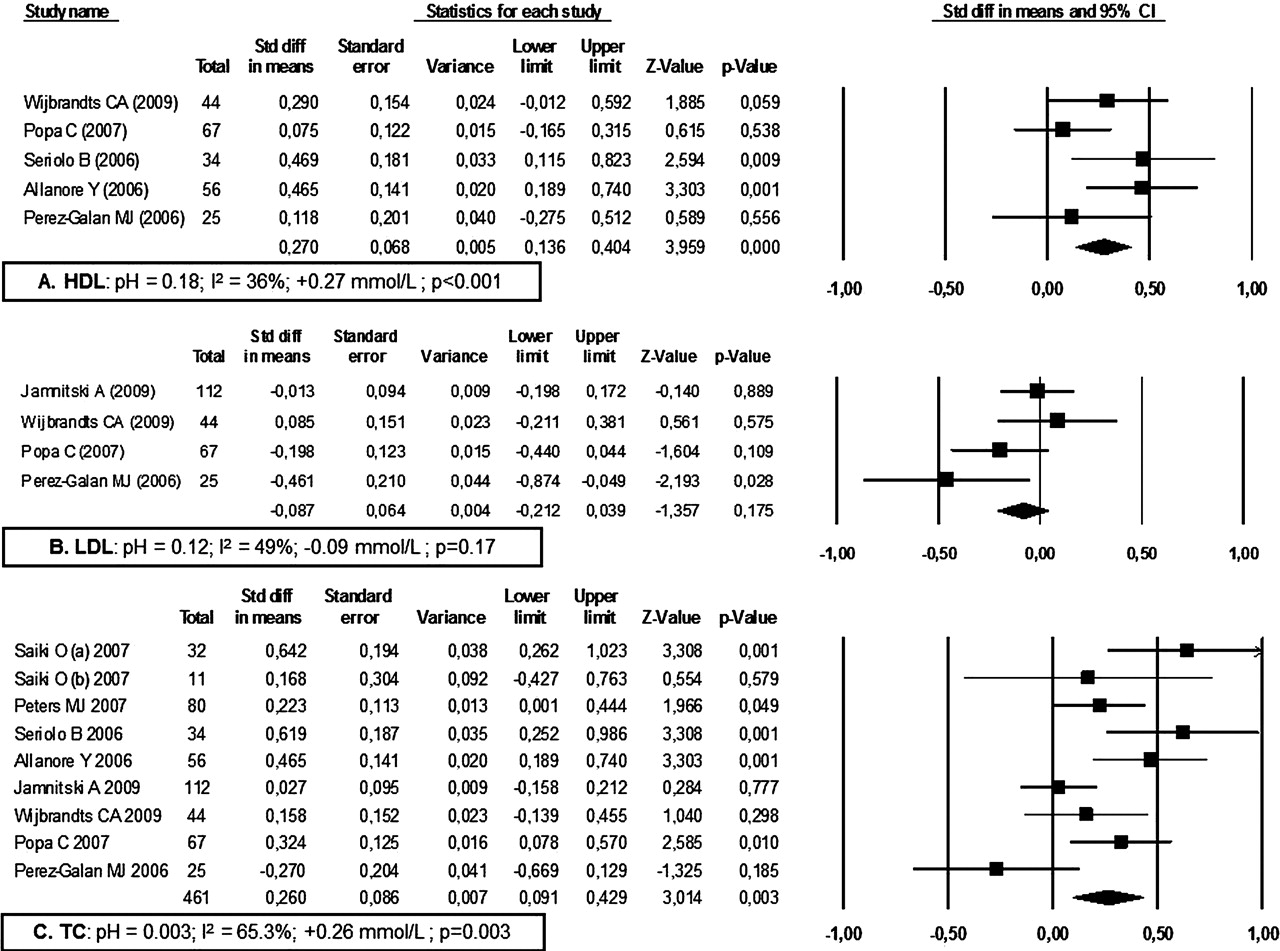
Observed changes after treatment with tumour necrosis factor α inhibitor at long-term (6–12 months) in (A) high-density lipoprotein (HDL)-cholesterol level, (B) low-density lipoprotein (LDL)-cholesterol and (C) total cholesterol (TC). In the study by Saiki et al,29 data for responders and non-responders were given separately. pH, p value for heterogeneity; I2, percentage of heterogeneity.
LDL-cholesterol
Changes in the LDL-cholesterol level associated with TNFi treatment were documented in five studies (304 patients; figure 2). Heterogeneity was high despite random effects modelling (I2=72.2%; p-H=0.006), which was explained by the study by Allanore et al which reported the LDL-cholesterol level at 6 months compared with 1 year for the other four articles. After controlling for the findings of Allanore et al, heterogeneity was not significant with long-term treatment (4 studies, 248 patients, I2=49%, p-H=0.12; table 1). The LDL-cholesterol level did not change significantly after treatment with TNFi (−0.09 mmol/l, p=0.175). With inclusion of the Allanore et al findings and with random effects modelling, the LDL-cholesterol level was not modified with long-term TNFi treatment (+0.02; p=0.83).
Total cholesterol (TC)
The TC level was documented in eight articles (461 patients; figure 2). Heterogeneity was high despite random effects modeling (I2=65.3%; p-H=0.003). The TC level was significantly increased after initiation of TNFi treatment (+0.26 mmol/l, p=0.003).
Atherogenic index (AI)
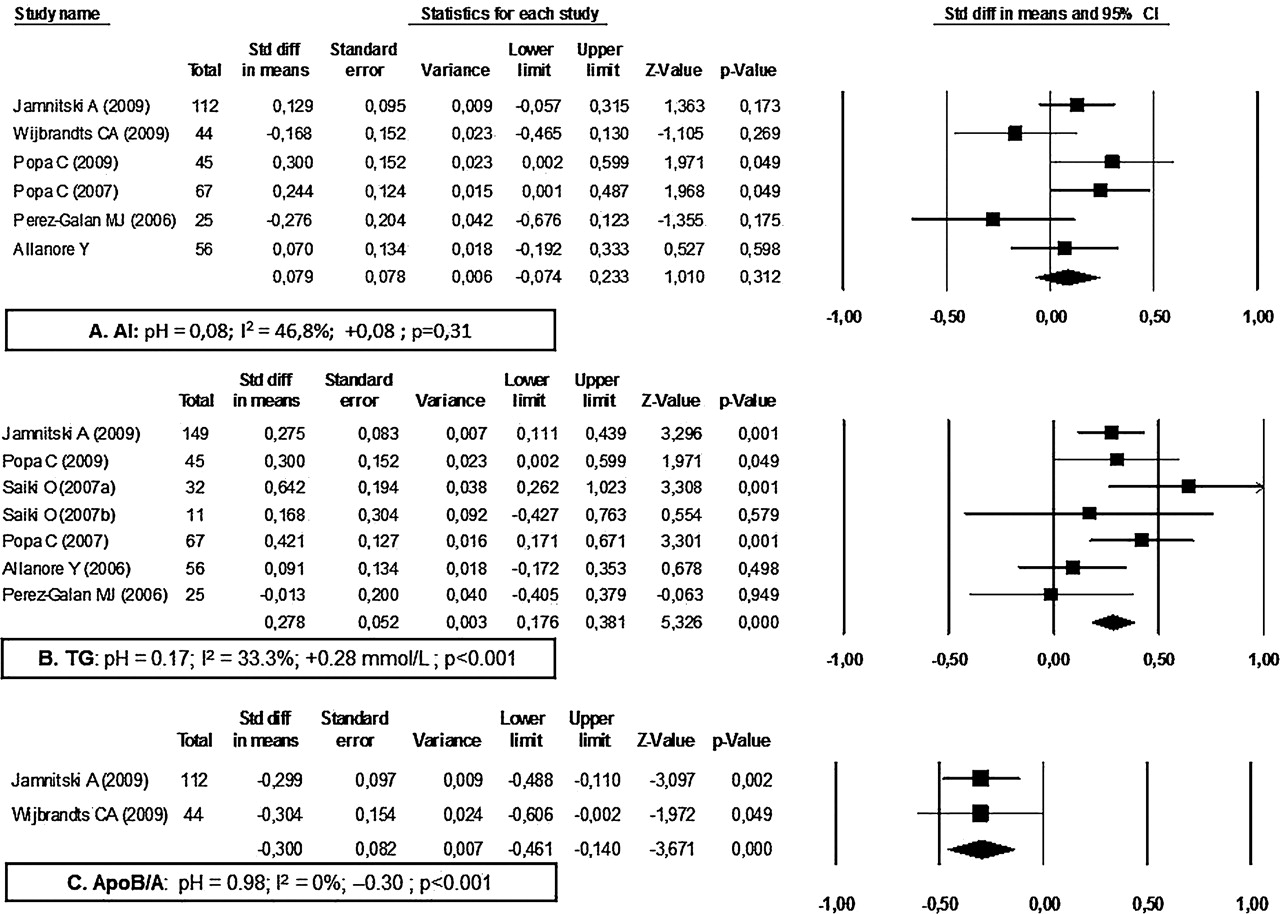
AI was documented in six studies (349 patients; figure 3). The study results were heterogeneous (I2=46.8%, p-H=0.08 after random effects modelling). AI was not affected by TNFi treatment (+0.08; p=0.31).
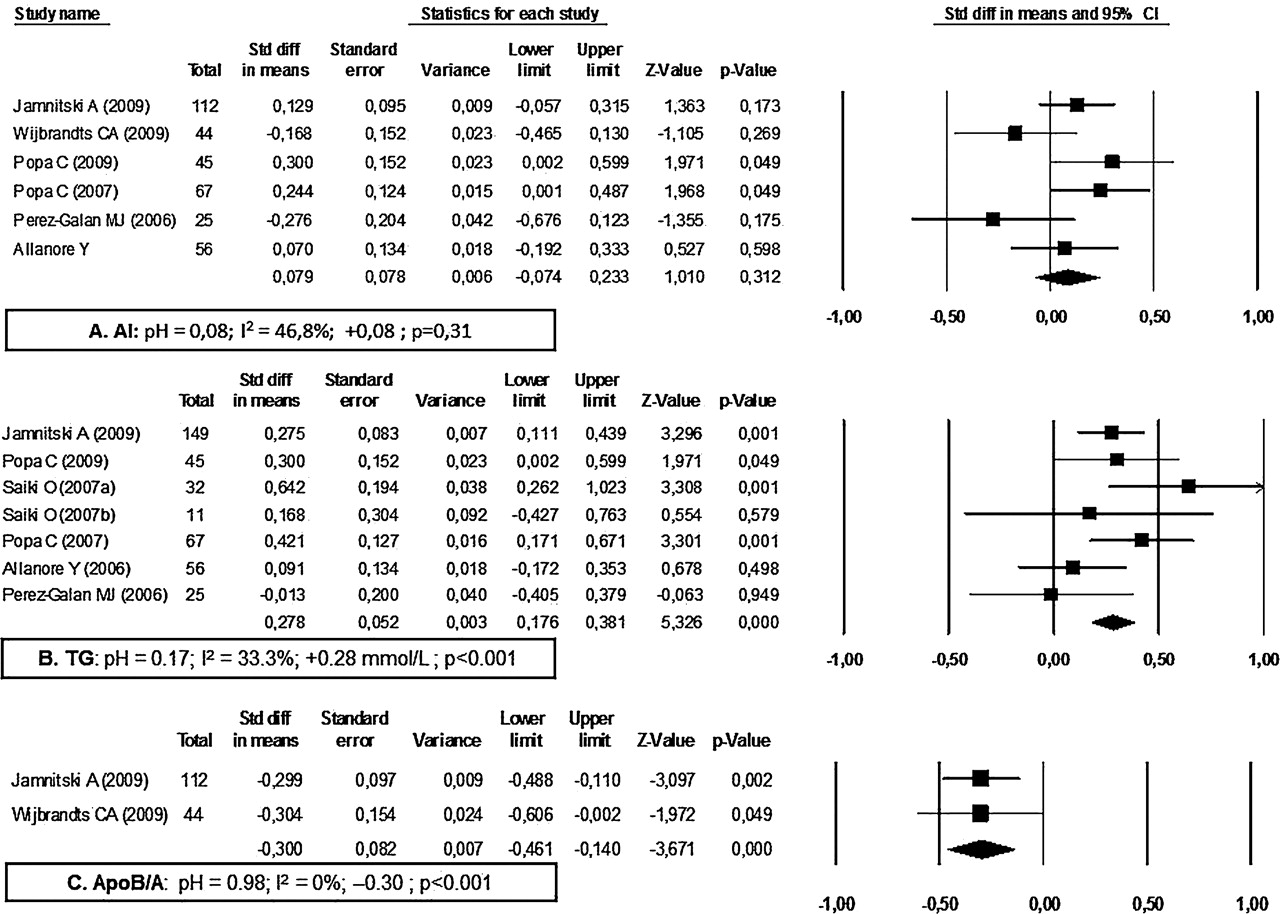
Observed changes after treatment with tumour necrosis factor α inhibitor at long-term (6–12 months) in (A) atherogen index (AI), (B) triglycerides (TG) and (C) apolipoprotein B/A (ApoB/A). In the study by Saiki et al,29 data for responders and non-responders were given separately. pH, p value for heterogeneity; I2, percentage of heterogeneity.
Total glycerides (TG)
The TG level was reported in seven studies (401 patients; figure 3). In the study by Saiki et al, data from responders and non-responders were given separately. Heterogeneity was significant with long-term treatment after random effects modelling (I2=55%, p-H=0.05). The heterogeneity was explained by the results of the study by Wijbrandts et al.22 On controlling for these findings, heterogeneity was not significant (6 studies, 385 patients, I2=33.3%, p-H=0.17). The TG level increased significantly after TNFi treatment (+0.28 mmol/l, p<0.001; +0.10 mmol/l, p=0.15). The findings of Wijbrandts et al differed from other results in patients with RA of shorter duration.22 With inclusion of the study by Wijbrandts et al, the TG level still increased with long-term treatment (+0.08 mmol/l, p=0.006).
Apolipoprotein B/A
Two studies were included (156 patients; figure 3). Heterogeneity was not significant (I2=0%, p-H=0.98). The ApoB/A level decreased significantly (0.30, p<0.0001). The ApoA level increased significantly (4 studies, 340 patients, I2=0%, p-H=0.83; +0.28 mmol/l, p<0.0001) while ApoB remained at similar levels before and after TNFi treatment (3 studies, 223 patients, I2=0%, p-H=0.51, difference −0.03 mmol/l, p=0.63).
Short- and mid-term study outcomes
A significant increase in HDL and TC was observed at short- and mid-term analysis (HDL: +0.41 mmol/l, p<0.0001 and +0.38 mmol/l, p<0.0001, respectively; TC: +0.39 mmol/l, p<0.0001 and +0.20 mmol/l, p=0.002, respectively). LDL-cholesterol increased at short-term analysis (+0.44 mmol/l, p<0.0001) but returned to pretreatment values at mid-term analysis (−0.01 mmol/l, p=0.88). AI was not affected by TNFi treatment at short-term analysis (+0.07, p=0.31). TG increased at short-term (+0.18 mmol/l, p=0.009) but not at mid-term analysis (+0.10 mmol/l, p=0.15). ApoB/A tended to decrease at mid-term analysis (−0.13, p=0.08).
Publication bias
No publication bias was found at long-term (Egger p>0.10) but some publication bias (Egger p<0.10) was found for short and mid-term analyses. Using the Duval and Tweedie method, we built estimator and 95% CI and symmetrised the funnel plot by adding data for fictitious studies. This correction confirmed the significance of our previous results.
Linear mixed model and Tukey–Kramer adjusted p values
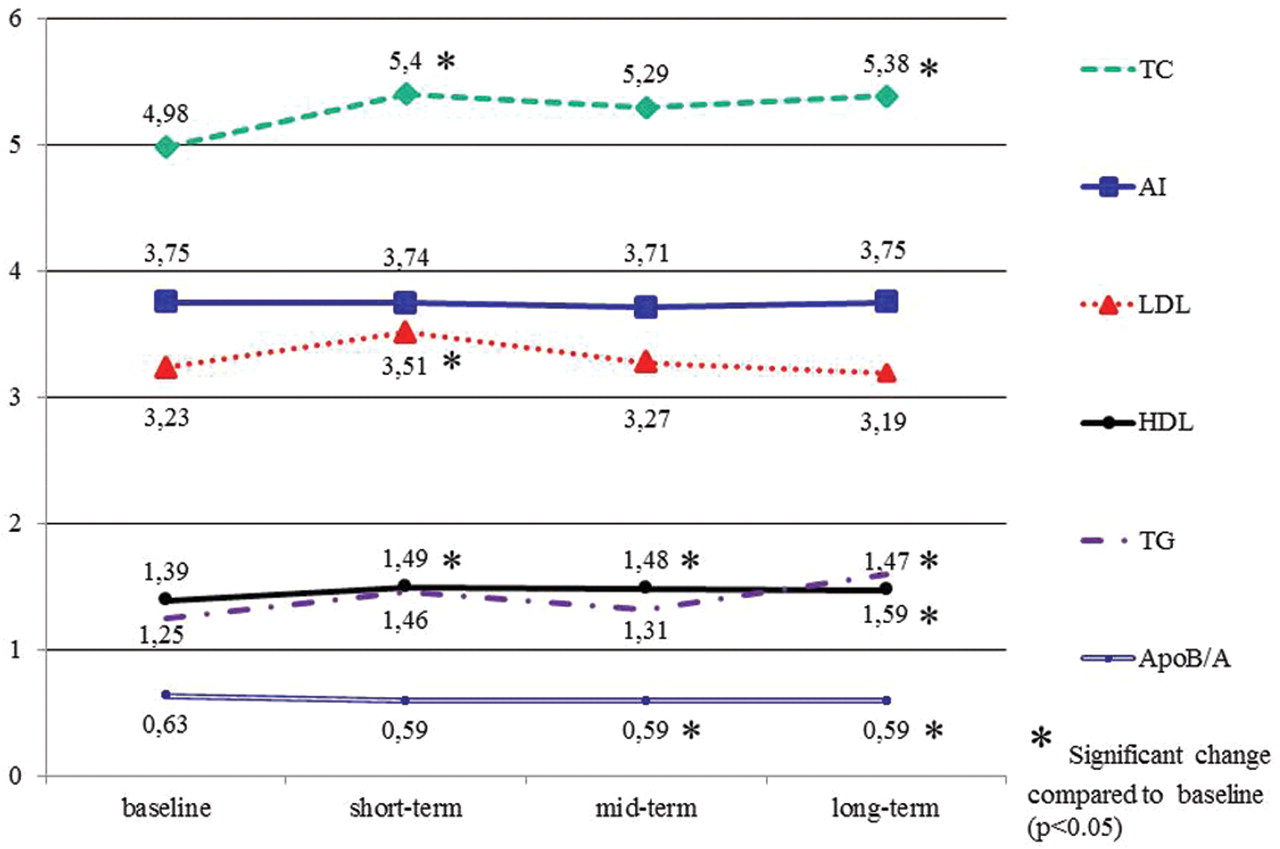
All results previously presented were confirmed using a multivariate linear mixed model (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Variations in lipid parameters determined by multivariate linear mixed model. Values expressed in mmol/l except for atherogen index (AI). For total cholesterol (TC), n=702 (13 studies); for AI, n=626 (11 studies); for low-density lipoprotein (LDL)-cholesterol, n=485 (9 studies); for high-density lipoprotein (HDL)-cholesterol, n=659 (12 studies); for trigycerides (TG), n=566 (10 studies); and for apolipoprotein B/A (ApoB/A), n=308 (4 studies). Short-term, 2–6 weeks; mid-term, 12–16 weeks; long-term, 22–52 weeks.
Discussion
Our data from a systematic review and meta-analysis of studies investigating the modification of lipid levels with TNFi treatment in RA suggest that TNFi is associated with a significant increase in HDL-cholesterol, TC and TG levels (about +0.2, 0.3 and 0.3 mmol/l corresponding to 0.08, 0.12 and 0.26 g/l, respectively). The LDL-cholesterol level and AI were not affected by TNFi treatment. The ApoB/A ratio seemed to decrease with long-term treatment but this result was based on only two studies. However, it was also observed in the linear mixed model of four studies. More studies are needed to confirm the effect on ApoB/A.
The cardioprotective effect of TNFi has been suggested in several studies. The incidence of first cardiovascular events was lower in patients with RA treated with TNFi than in patients with RA not treated with TNFi in a Swedish cohort (age-, sex- and disability-adjusted incidence rate; n=983; ratio 0.46; 95% CI 0.25 to 0.85, p=0.013).51 In the same cohort, after adjustment for age, sex, disability and baseline comorbidity, patients receiving TNFi also had a lower incidence of cardiovascular deaths than patients not receiving TNFi treatment (n=1430; standardised mortality ratio (SMR) 0.65; 95% CI 0.46 to 0.93).12 The effect was significant for women (SMR=0.52; 95% CI 0.33 to 0.82) but not for men (SMR=0.95, 95% CI 0.52 to 1.71).12 In the CORONNA registry the risk of cardiovascular events in patients treated with anti-TNF agents (n=4684) was 60% lower than the risk in patients treated with synthetic DMARDs other than methotrexate (n=1785; HR=0.39; 95% CI 0.19 to 0.82).52 Methotrexate treatment was not associated with a decreased risk of cardiovascular events (n=4969; HR=0.94; 95% CI 0.49 to 1.80). However, the cardioprotective effects of anti-TNF agents are not always clear. In a North American study of 3501 patients with RA, those receiving biological agents (including etanercept, adalimumab, infliximab and anakinra) had the same number of cardiovascular events as patients receiving methotrexate monotherapy (biological agent monotherapy: OR 1.0, 95% CI 0.5 to 1.9; biological agents plus methotrexate combination therapy: OR 0.8, 95% CI 0.3 to 2.0).53 In a national prospective observational study of data from the British Society for Rheumatology Biologics Register, patients with RA receiving TNFi therapy (n=8670) showed no reduction in the rate of myocardial infarction compared with those receiving DMARDs (n=2170) (incidence rate 1.44; 95% CI 0.56 to 3.67) after adjustment for baseline risk factors.11 Among patients receiving TNFi treatment, responders had a lower risk of myocardial infarction than non-responders (adjusted incidence rate 0.36; 95% CI 0.19 to 0.69).11
The increase in HDL-cholesterol and apoB/A levels observed in this meta-analysis could have a cardioprotective effect.54 Low HDL-cholesterol is strongly associated with cardiovascular risk; however, a low HDL-cholesterol level correlates with the presence of other confounding atherogenic factors such as increases in serum TG, remnant lipoproteins or small dense LDL particles and insulin resistance. It is therefore uncertain whether raising HDL-cholesterol levels per se, independent of other changes in lipid and/or non-lipid risk factors, can reduce the risk for coronary heart disease.55 Moreover, the increase observed in this meta-analysis was limited. Conversely, LDL is the major atherogenic lipoprotein and has long been identified as the primary target of cholesterol-lowering therapy. This focus on LDL has been strongly validated by recent clinical trials which show the efficacy of LDL-lowering therapy for reducing the risk of cardiovascular disease.55 In the present meta-analysis, LDL-cholesterol was not modified after treatment with TNFi. so it is not likely that the presumed decrease in the risk of cardiovascular disease by TNF blockers is mediated via quantitative changes of the lipid profile.
This effect could be explained by favourable effects on homeostasis and stabilisation of coronary plaques, as suggested by Karpouzas et al.56 Indeed, they found that patients treated with TNFi (n=47) had a 76% reduced risk for the presence of ‘vulnerable’ plaque (p=0.006) than patients treated with DMARDs (n=27) after adjustment for age, sex and Framingham risk factors. The cardiovascular protective effect could also be explained by the decrease in left ventricular mass and the correction of left ventricular hypertrophy which is known to be associated with a decreased cardiovascular risk.57
Nine of the 13 studies aimed to determine whether the observed effects of TNFi treatment on lipid levels were due to variation in the disease activity score in 28 joints (ΔDAS28) or inflammation parameters. One study did not find any link between the response to treatment and changes in lipid levels.39 Six studies reported an association between ΔDAS and/or variation in the erythrocyte sedimentation rate and C reactive protein and HDL-cholesterol levels.22 32,–,35 43 A decrease of one point in the DAS28 increased the HDL-cholesterol level by 0.045 mmol/l.33 The TC level was increased only in responders in the study by Saïki et al,29 and changes in TC were inversely correlated with DAS28 in three studies.32 33 35 Jamnitski et al and Popa et al showed that AI increased in EULAR non-responders (p=0.03 and p=0.09, respectively) but did not find any changes in responders.15 32 Peters et al and Popa et al also found a positive correlation between changes in AI and DAS28 (a decrease of one point in DAS28 resulted in a decrease of 0.016 in AI).32 33 One report described a significant decrease in apoB/A in responders but an increase in non-responders, and another reported variations in the apoB/A and apoA level correlated inversely with ΔDAS28.15 33 Only the study by Saiki et al showed an effect of inflammation on the TG level, which increased only in responders.29
To determine the effect of TNFi treatment we also studied changes in lipid levels in patients receiving conventional DMARDs. Three papers reported results at 12 months in 119 patients.58,–,60 No changes were observed in LDL-cholesterol or TG levels. TC and HDL-cholesterol levels were significantly increased at 12 months (3 studies, n=119 for both; I2=0%, p-H=0.46, +0.37 mmol/l, p<0.001; and I2=22.6%, p-H=0.28, +0.454 mmol/l, p<0.001, respectively) and AI was significantly decreased (2 studies, n=77; I2=0%, p-H=0.68, −0.434, p<0.001; unpublished data). Conventional DMARDs therefore seem to have the same effect as TNFi on TC and HDL-cholesterol levels but a significant positive effect on AI. With regard to other biological agents, rituximab has been poorly studied with only two studies of five and six patients published.61 62 The effect of tocilizumab effect was studied in a meta-analysis of the results of six initial trials and five long-term extensions in Japan.63 TC, LDL-cholesterol and HDL-cholesterol levels increased in the first weeks of treatment and then remained stable (at 7 years) whereas AI did not change. Similar results for Caucasian patients from a phase 3 programme with a 2.4-year follow-up were presented at an ACR meeting in 2009 (OPTION, AMBITION, RADIATE, TOWARD, LITHE studies).33
Our data could suggest a different effect of TNFi treatment on soluble receptors and monoclonal antibodies. For HDL-cholesterol and apoA analyses, heterogeneity was explained by the Jamniki et al study,15 the only one which exclusively analysed the effects of etanercept. This study showed no significant effect of TNFi but, unlike other reports, there was a non-significant decrease in the HDL-cholesterol level after long-term treatment (−0.13 mmol/l, 95% CI –0.32 to 0.05, p=0.16). In other analyses, etanercept showed results similar to those of monoclonal antibodies. Further studies are needed to compare the effect of soluble receptors and monoclonal antibodies on the lipid profile.
Our study has some limitations. First, the studies differed in the three time-points so care should be taken in interpreting the comparisons between time-points. The linear mixed model nevertheless allows partial correction of this problem. In addition, the differences seen with etanercept in one study need to be confirmed in further studies. Finally, this meta-analysis studied quantitative lipid abnormalities, but qualitative disorders (proinflammatory HDL-cholesterol, small dense LDL-cholesterol or oxidative LDL levels) were not addressed. The lipid variables were analysed in different laboratories. However, we did not study absolute values but, rather, changes in levels after TNFi treatment so this should not significantly influence the results.
Conclusions
This meta-analysis shows that long-term treatment with TNFi is significantly associated with increased HDL, TC and TG levels and may be associated with a decreased apoB/A level, whereas the LDL level and AI are not significantly modulated after treatment. The increase in the HDL level could be beneficial, but it is unlikely that the presumed decrease in the risk of cardiovascular disease by TNF blockers is mediated via quantitative changes in the lipid profile. With the exception of TG, these modifications may be due to the correction of inflammation and similar effects might be found with other treatments.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Web Only Data - This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Competing interests None.
-
Funding Abbott France pharmaceutical company provided support by organising a meta-analysis methods workshop but played no further role in the project.
-
Provenance and peer review Not commissioned; externally peer reviewed