Article Text

Abstract
Objective To investigate the 2-year clinical and radiological outcomes of patients with early rheumatoid arthritis (RA; symptom duration <1 year) who had initially responded well to methotrexate monotherapy.
Methods In the SWEFOT trial, all 487 patients started methotrexate (target dose 20 mg/week). After 3–4 months, 147 had low disease activity, 28-joint based disease activity score (DAS28) ≤3.2. These patients were not randomly selected but were followed in regular care for 2 years. Clinical outcomes and radiographic progression according to the van der Heijde modified Sharp (SvdH) score were analysed.
Results The majority of the 147 patients continued on methotrexate monotherapy. After 1 and 2 years, DAS28 remission was achieved in 59.6% and 71.8% and mean observed DAS28 values were 2.53 and 2.25, respectively. Despite the favourable clinical course, a proportion of the patients progressed radiographically with a mean (SD) increase in the SvdH score after 2 years of 3.90 (6.84). There was no significant difference in progression between patients in DAS28 remission versus not in remission (p=0.73). At baseline, approximately half the patients had no radiographic damage, while after 2 years the proportion was approximately 20%.
Conclusion Most early RA patients who achieve low disease activity after 3–4 months of methotrexate monotherapy continue to have low disease activity during 2 years follow-up, and additional treatment is needed infrequently. Some radiological progression occurs in most patients, and may be marked or severe in some, even despite sustained DAS28 remission. Close monitoring for radiological progression is thus warranted.
Statistics from Altmetric.com
Methotrexate has been used to treat rheumatoid arthritis (RA) since the 1980s, and due to its well-documented effects and a favourable safety profile,1 it remains the first-line treatment of choice according to recent European League Against Rheumatism (EULAR) guidelines.2 Although studies have shown that combination therapy with methotrexate and glucocorticoids,3 4 other disease-modifying antirheumatic drugs (DMARD)5 6 or a tumour necrosis factor inhibitor7 8 is superior to methotrexate monotherapy, many patients respond well to methotrexate alone and might not need any additional treatment.3 9 It can thus be argued that an initial 3–4-month trial of methotrexate monotherapy is a rational treatment approach in early disease. Disease activity after 3–4 months has been shown to correlate well with that after 1 year.10 11 Therefore, patients who respond to this simple treatment could be continued on it without the need for additional more expensive therapies. However, as one of the goals of RA therapy is to prevent or retard joint damage as well as maintaining a good functional status, it is important to know how patients who respond well clinically to methotrexate do at later follow-up visits and, even more importantly, whether they progress radiographically. In the SWEFOT trial,12 we have previously shown that male gender, non-smoking, older age, shorter symptom duration, better physical function and concurrent low-dose glucocorticoid treatment predicted better response after 3–4 months of methotrexate treatment.13
Here we evaluate the clinical and radiological outcomes of patients who initially responded well to methotrexate and were followed in regular care during the subsequent 2 years.
Methods
Study population: the SWEFOT trial
The SWEFOT trial was a collaboration between 15 different rheumatology units in Sweden. All patients were initially treated with methotrexate at a starting dose of 10 mg a week, which was increased every 2 weeks by 5 mg increments up to at least 20 mg a week. Folic acid supplementation in tablet form was also added.12 Liver enzymes and blood counts were monitored in accordance with local guidelines, and abnormalities in these measures could lead to dose adjustment, based on established clinical routines.
Inclusion criteria included age above 18 years, symptom duration of less than 1 year and no previous DMARD treatment. The disease activity was measured by a rheumatologist using the 28 joint-based disease activity score (DAS28),14 and a score of more than 3.2 at the 3-month follow-up visit was required to enter the randomised portion of the trial. All participants fulfilled the American Rheumatism Association 1987 revised classification criteria.15 The main exclusion criterion was a contraindication to any of the trial medications. Patients who received glucocorticoid therapy had to have been on a stable dose of at most 10 mg a day prednisone (or equivalent) for at least 4 weeks before study entry.
The study was approved by regional ethics committees of all participating units and was registered at http://www.clinicaltrials.gov (NCT00764725). All patients were provided with oral and written information before inclusion, and consented to participate by signing the informed consent document.
At 3–4-month follow-up, patients with an incomplete response (DAS28 >3.2) to methotrexate as a monotherapy were randomly assigned to two different treatment strategies, as previously described.12
The patients who responded well to methotrexate monotherapy at the 3–4-month follow-up (DAS28 ≤3.2) did not enter the randomisation and were no longer, technically, part of the SWEFOT trial. These patients were followed in standard care.
Follow-up
The follow-up visits at the rheumatology clinics were scheduled according to the clinical guidelines for early RA management, every 3 months during the first year and thereafter at 6-month intervals, but depending on the disease activity. As for all early RA patients at these clinics, the patients were followed in the Swedish rheumatology quality registry, in which at each visit clinical and laboratory results were registered as well as information about current treatment. A total of 37 patients had incomplete data or were lost to follow-up at 2 years. Note that the Swedish rheumatology quality registry does not influence therapy decisions, which are based on physician judgement.
Measures of disease activity, functional status and response to treatment
Disease activity was measured by DAS28 based on the erythrocyte sedimentation rate, but was replaced by C-reactive protein when the erythrocyte sedimentation rate was missing.14 American College of Rheumatology (ACR) core set measures were calculated at each follow-up visit.16 17 The simple disease activity index (SDAI) and the clinical disease activity index (CDAI) were also calculated.18 The functional status was measured by the health assessment questionnaire disability index (HAQ).19 20
EULAR response criteria,21 ACR response criteria16 and also the SDAI and CDAI response criteria were used.18
Radiographic assessment
Radiographs of hands and feet were obtained at baseline, 1 year and 2 years in accordance with current practice guidelines in Sweden (missing for 16, 28 and 33 patients, respectively). Radiological progression was evaluated according to the van der Heijde modified Sharp (SvdH) score22,–,24 by two certified readers (KA, KF) and defined as an increase in total SvdH score of at least 10 units. The SvdH scoring system has a range from 0 to 448 units, in which the maximum erosion score of joints in the hands is 160 and in the feet 120 units, and the maximum score for joint space narrowing in the hands is 120 and in the feet 48 units.22 23
Statistical analysis
The distribution of the variables is given as the mean with SD. We used the χ2 test to compare dichotomous variables between groups, the independent two-tailed Student's t test and paired t test to compare continuous variables between and in groups. For non-normally distributed data, and in particular for the radiological scores, the Mann–Whitney test was used.
For patients who had missing data at the 1 or 2-year follow-up visits, the last observation carried forward (LOCF) method was used.
We performed statistical analysis with SPSS 15.0 and STATA version 11.0.
Results
Patient characteristics
Of the 487 patients who were included in the SWEFOT trial, 147 patients responded well to methotrexate monotherapy, that is, had a DAS28 value of 3.2 or less after 3–4 months. This group of patients received regular care, figure 1. At the 1 and 2-year follow-up, 82.4% and 77.9% of the patients with complete follow-up data were still on methotrexate monotherapy, respectively.

Study design and disposition of responders. Triple therapy is methotrexate, sulfasalazine and hydroxychloroquine. Biological agents are infliximab, etanercept or adalimumab. DAS28, 28 joint-based disease activity score; DMARD, disease-modifying antirheumatic drug; MTX, methotrexate.
The baseline characteristics of these patients are shown in table 1. Patients with complete follow-up data at 2 years (n=110) did not differ from the group as a whole. The mean (SD) methotrexate dose at 1 year was 18.1 mg (2.9) (n=117) and at 2 years 16.5 mg (4.4) (n=119). A small number of patients (n=6) were on no antirheumatic medications at 2 years.
Disease activity at follow-up visits
Patient characteristics and disposition
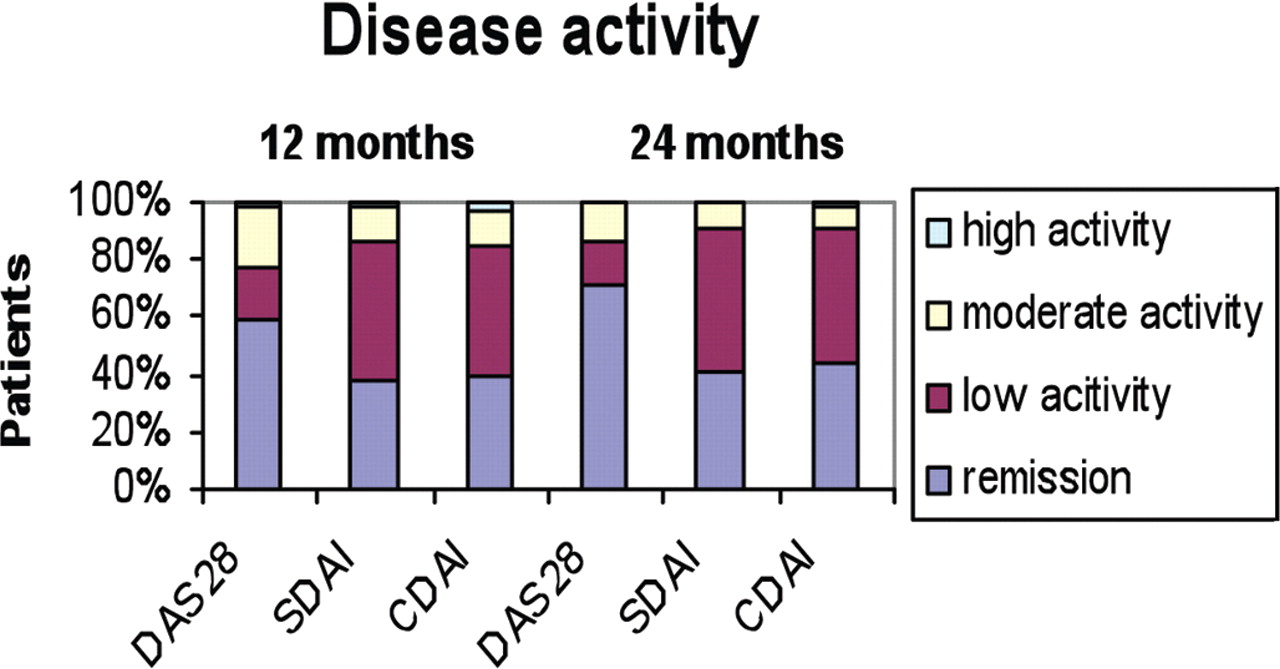
The proportion of patients achieving the various disease activity categories according to the DAS28, SDAI and CDAI measures after 1 and 2 years are shown in figure 2. Only a small proportion of the patients did not maintain low disease activity or remission at follow-up. After 1 year, DAS28 remission was achieved in 59.6%, while 37.4% and 39.4% achieved remission as defined by the SDAI and CDAI measures, respectively. After 2 years, the proportions in DAS28/SDAI/CDAI remission were 71.8%, 41.2% and 43.7%, respectively (p<0.0001).

{kind=link}
{kind=link}
Remission rates at 1 and 2 years. n=114/107/109//110/102/103. CDAI, clinical disease activity index; DAS28, 28 joint-based disease activity score; SDAI, simple disease activity index.
Mean (SD) observed DAS28 values were 2.53 (1.02) and 2.25 (0.82) at 1 and 2 years, respectively (p=0.03). A LOCF analysis for patients with missing data yielded mean DAS28 values of 2.50 (1.02) and 2.34 (0.85) at 1 and 2 years, respectively (p=0.03). Using the LOCF method, 60.5% of patients were in DAS28 remission at 1 year and 67.3% at 2 years (p<0.0001).
Proportion of patients achieving different response measures at follow-up visits
As seen in table 2, the clinical responses according to EULAR and ACR response16 21 criteria at the 3–4-month follow-up were very good, as expected because the patients had to have DAS28 of 3.2 or less to be included in this cohort. More importantly, the vast majority of the patients maintained good responses at the 1 and 2-year follow-up. Therefore, after 1 year, 76.3% of the 114 patients with follow-up data had achieved a good response according to EULAR criteria. At 2 years (n=110), this number had increased to 85.5%. A more conservative analysis was also performed, in which patients without data at 1 and 2 years were regarded as non-responders (table 2).
EULAR and ACR responses at 3, 12 and 24 months
Radiological progression at follow-up
As shown in table 3, the mean (SD) value for the total SvdH score at baseline, 1 and 2-year follow-up was 3.78 (7.72), 5.98 (8.66) and 7.87 (9.91), respectively, p<0.0001 compared with baseline at both time points. The same analysis limited to those patients who had complete radiological data at all follow-up time points (n=91) showed that the mean (SD) value for the total SvdH score was 3.88 (8.29), 6.20 (9.21) and 7.95 (10.10), respectively, p<0.0001 compared with baseline at both time points.
Radiological progression in patients who responded well clinically to methotrexate
At baseline, 48.1% of patients had no radiographic damage, that is, the total SvdH score was 0, but at 1 year this proportion had decreased to 26.9% and at 2 years to 20.2% (p<0.0001). An erosion score of 0 was found in 62.6% at baseline, 47.9% at 1 year and 45.6% at 2 years (p<0.0001).
The mean progression after 1 year (n=107) was 2.21 (4.15) and after 2 years (n=101) 3.90 (6.84) (p=0.0003). Progression was seen for both the erosion score and joint space narrowing score with a mean increase at 2 years of 1.40 (4.11) and 2.50 (4.45), respectively.
A subset analysis of the patients who were in DAS28 remission (n=47/52) and those who were not in DAS28 remission (n=33/22) at 1 and 2 years of follow-up with available radiographs showed a mean increase in the total SvdH score of 3.96 (7.56)/4.17 (7.28) and 4.76 (7.19)/4.82 (7.58) (p=0.63)/(p=0.73). No difference was seen either between patients in DAS28 remission at every follow-up visit compared with the other patients (3.79 (6.68) versus 4.75 (8.20) p=0.6).
The same analysis for patients in SDAI remission (n=33) versus not in SDAI remission (n=40) at 2 years showed an increase in the total SvdH score of 3.88 (6.35) and 4.85 (8.13), respectively (p=0.57). Patients who were on methotrexate monotherapy throughout the 2-year follow-up had a mean progression of 3.46 (6.28). Patients who received another antirheumatic treatment in combination with methotrexate or those who switched treatment to other antirheumatic treatment during the 2-year follow-up had a mean progression of 7.20 (9.82) (p=0.06). Analysis of the patients who had been on stable dose glucocorticoids according to the inclusion criteria (n=17) before inclusion versus patients without glucocorticoids (n=84) at 2 years of follow-up with available radiographs showed a mean increase in total SvdH score of 3.88 (7.63) and 3.90 (6.71), respectively (p=0.9). The mean prednisolone dose at baseline was 6.9 mg/day (3.4).
No radiographic progression was observed in 51.4% (n=107) and 38.6% (n=101) of patients at 1 and 2-year follow-up, respectively (p<0.0001). A change of one to five units in the total SvdH score was seen in 30.8% (n=107) at 1 year and 31.7% (n=101) at 2 years. Six patients had at least a 10 units increase in total SvdH score at 1 year and 15 patients had a 10 units or greater increase in the SvdH score after 2 years, of whom 11 patients were still on methotrexate monotherapy. There was no statistically significantly difference in DAS28 at 1 and 2 years between patients with progress greater than 10 units and the other patients. Seven of these 15 patients were in DAS28 remission after 1 year and 10 after 2 years. Three patients had progressed more than 20 units.
Functional status (disability)
Mean HAQ (SD) values decreased from 0.98 (0.51) at baseline (n=146) to 0.30 (0.41) at 1 year (n=108) and 0.26 (0.35) at 2 years (n=103) (p<000.1). There was no significance difference in HAQ change between progressors (0.70 (0.55)) and non-progressors (0.78 (0.48)) (p=0.64). The same analysis limited to patients with complete HAQ data at baseline, 1 and 2 years (n=83) showed the same results (data not shown).
Discussion
We have here presented the 2-year follow-up on 147 patients who after 3–4 months had responded well clinically to initial treatment with methotrexate monotherapy (achieving a low disease activity, ie, DAS28 ≤3.2) and who were therefore not randomly assigned but followed in regular care at 3–6-month intervals. The results show that they had good clinical responses over the first 2 years, but that radiological progression occurred in many patients in this cohort. The importance of this study lies in the fact that methotrexate therapy has been and remains the most commonly used drug for RA. Although anti-tumour necrosis factor biological agents in combination with methotrexate have been shown to be superior to methotrexate monotherapy, both clinically and radiologically, on a group level,7 the cost and risk of additional treatment has to be considered, and evidently many patients manage well without biological treatment. Therefore, both options can still be considered.2 25 Our data add further information regarding this important clinical decision.
Another clinically relevant question is whether patients who initially respond to methotrexate are likely to need additional therapy later on to control clinical disease activity.
As a group, these patients had excellent clinical results, as the vast majority stayed on methotrexate monotherapy and had low disease activity or remission throughout the 2-year follow-up period. Therefore, an early response to methotrexate is a reliable predictor of further therapeutic efficacy as was also demonstrated in other cohorts.10 Furthermore, we found a clinically significant improvement of function as measured by HAQ. There was no difference in the changes in HAQ between radiographic progressors and non-progressors, so the clinical relevance of the radiological progression on functional impairment over the first 2 years was less clear.
Despite these positive clinical results, a substantial proportion of the patients progressed radiographically, despite having a low disease activity or even remission. Most strikingly, the patients who were in DAS28 remission at every visit up to and including the 2-year follow-up showed at least equal progression to patients not in remission. Therefore, in this study, the clinical assessment can not reliably differentiate between patients who do and those who do not progress radiologically over 2 years. One important practice implication of this study is that, if methotrexate monotherapy is used, radiological progression should be monitored. In our practice setting, x-rays are now taken at baseline, after 3 months, again after 1 year and then yearly for at least the initial years of the disease. This is in line with the EULAR recommendations for the management of early arthritis, which state that joint damage should be assessed by x-rays of the hands and the feet every 6–12 months during the first few years.26
Fewer patients were in remission as defined by the CDAI and SDAI than by the DAS28, which is consistent with previous studies, which showed that SDAI and CDAI have more stringency in defining remission.27 28
The strengths of this study are that it originated within the frame of a trial and was then conducted as part of regular care. The latter observational design also is one of the limitations due to the relatively high proportion of missing data. Although these patients were initially enrolled in a clinical trial, the continued follow-up after having responded to initial methotrexate therapy was left up to the individual physician, and recording of data followed the usual procedures of early RA patients in the participating clinics. Therefore, these data were not reported as meticulously as would have been the case if the patients had been continued in the clinical trial as such, and indeed, complete data were available for 110 out of 147 patients. Nevertheless, the baseline characteristics for patients without follow-up data did not differ from the whole group.
We did not detect any significant difference between patients in remission versus not in remission by DAS28 with respect to radiological progression, but the number of patients in DAS28 remission with available radiological data was limited. Patients in SDAI remission had numerically (but not statistically significantly) less progression than those who were not in SDAI remission. Nonetheless, including patients with x-ray data but with incomplete clinical follow-up data and defining them as being not in remission (using a ‘non-responder’ imputation) results in even lower progression in the non-remission group, underscoring the disjunction between clinical and radiological results.
Emery et al8 compared methotrexate monotherapy with methotrexate combined with etanercept and reported a mean increase in the total SvdH score of 2.44 for the methotrexate monotherapy group after 52 weeks follow-up, which is in line with our study. Moreover, almost the same proportion of the methotrexate monotherapy group in that trial, compared with ours, did not progress radiographically. In that study 59% of patients in the methotrexate arm had radiological progression less than 0.5 point in total score during 1 year, whereas we found no radiological progression in 51.4% of our patients during the first year. A key difference between these studies is of course that in our study the whole cohort had already responded well to methotrexate monotherapy at the 3–4-month follow-up visit, suggesting that either our patient population had more destructive disease or the radiological benefit of methotrexate was very limited indeed.
In the BeSt study,3 the radiological results for patients who had sequential monotherapy (started with methotrexate monotherapy) were also similar to our study. The mean increase in the total SvdH score in this group of patients was 3.6 during 1 year, compared with 2.2 points in our cohort. The difference may be due, once again, to the fact that our patients were preselected for a good methotrexate response.
In the ASPIRE study, Durnez et al29 found that the proportion of patients on methotrexate monotherapy with rapid radiological progression after 1 year (increase in SvdH score ≥5 units) was 22.8%, which is in the line with our study. Furthermore, patients with initial DMARD combination therapy with corticosteroids had less radiological progression in that study.29 Our data are also consistent with those published by Cohen et al,30 in which 33% of patients with RA in sustained remission at 3 and 5 years had a significant increase in radiological damage; and by Molenaar et al,31 who showed that the progression of joint damage between baseline and 2 years occurred even in patients with RA in persistent clinical remission.
One key difference between our study and many published randomised trials is that the proportion of patients on concomitant low-dose glucocorticoid treatment, 17.7%, is lower. Low-dose daily glucocorticoids have been shown to prevent radiographic progression,4 and since that publication, the routine use of such therapy in Sweden has increased considerably. However, in our study there were no significant differences in radiological progression between patients with and without concomitant glucocorticoids.
Our data showed that a subset of patients had quite severe progression (eg, 15% of patients had progression of 10 points or more). Such changes might also have been expected to have resulted in changes in functional status, but we could not detect any difference in the decrease in HAQ for progressors versus non-progressors, nor any difference in DAS28 between these groups. Part of the explanation may be that HAQ values in our patient cohort were generally low and HAQ has a floor effect. Another explanation may be that HAQ mainly evaluates reversible disability in the short term and irreversible disability in the long term. The functional outcome for this cohort of methotrexate responders, in terms of mean HAQ scores, was better than for all treatment arms of the BeSt study in early RA, but our patients had lower baseline HAQ.
Radiographic progression can occur in early RA despite a clinically acceptable response. Similar findings were previously reported based on the early RA cohort in our unit.32 One explanation for this might be that the DAS28-based remission criterion allows for a few swollen joints and it does not include evaluation of the feet. It is possible that such patients were included and that they had erosions in the feet, but we were not able to extract this particular information. However, patients with x-ray progression did not have worse scores on patient-reported outcomes (HAQ score, global health assessment, data not shown). A new four-criteria-based definition of remission has recently been proposed by a EULAR/ACR working group,33 and in that paper it was suggested that the SDAI score could also be used for determining remission. In our study we did not observe any significant difference between patients who were or were not in SDAI remission at 2-year follow-up, although patients in SDAI remission had numerically less radiological progression. A new remission definition will of course need prospective validation against long-term outcomes such as radiographic progression.33
One of the problems with radiographs in daily clinical practice is that they are often obtained infrequently, when severe progression might already have occurred. Furthermore, assessments by radiologists vary greatly. Integrating ultrasound into clinical practice and possibly the extended use of MRI to detect synovitis may be of value in the future.
Identifying the patients in need of more aggressive therapy is certainly important. A recently published review34 of factors predictive of a favourable clinical and radiographic outcome following methotrexate monotherapy concluded that disease activity after 3–6 months after the start of treatment was probably a better predictor than baseline disease activity. Therefore, high disease activity both at treatment start and at the 3-month follow-up was predictive of radiographic progression. Recently, two matrix risk models35 36 for radiographic progression have been reported from two different early RA trials.
Taken together, we have shown that patients with an initial good response to methotrexate monotherapy continue to do well clinically during the first 2 years, but the finding that radiographic progression was surprisingly high in some of these patients leads us to question whether methotrexate monotherapy is an acceptable initial therapy for all patients. Most importantly, our study highlights the importance of monitoring the radiological response in patients on methotrexate monotherapy with a good clinical response.
Acknowledgments
The authors would like to thank all participating patients, as well as the study nurses, co-investigators and colleagues who made this trial possible.
References
Footnotes
-
The SWEFOT trial investigators group Lars Cöster, Linköping; Eva Waltbrand, Borås; Agneta Zickert, Stockholm; Jan Theander, Kristianstad; Åke Thörner, Eskilstuna; Helena Hellström, Falun; Annika Teleman, Halmstad; Christina Dackhammar, Mölndal; Finn Akre, Örebro; Lotta Ljung, Umeå; Rolf Oding, Västerås; Katerina Chatzidionysiou, Stockholm; Margareta Wörnert, Stockholm.
-
Funding The study was supported in part by a grant from the Swedish Rheumatism Association. The authors were supported by clinical research funds from Stockholm County (ALF funds). An annual unrestricted grant was provided by Schering-Plough Sweden that was used to support a study coordinator and a medical monitor. RFvV has received research funding and/or honoraria from Abbott, Bristol-Myers Squibb, Merck, Pfizer, Roche and UCB Pharma.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the regional ethics committees of all participating units and was registered at http//www.clinicaltrials.gov (NCT00764725).
-
Provenance and peer review Not commissioned; externally peer reviewed.