Article Text

Abstract
Objectives To develop a score for assessment of patients' symptoms in primary Sjögren's syndrome (SS): the EULAR SS Patient Reported Index (ESSPRI).
Methods Dryness, pain, somatic and mental fatigue were identified as the main symptoms of patients with primary SS, in studies developing the Profile of Fatigue and Discomfort (PROFAD) and Sicca Symptoms Inventory (SSI). It was suspected that a single 0–10 numerical scale for each domain was sufficient to assess these symptoms. These four scales were gathered to form the ESSPRI. 230 patients, from 12 countries completed the ESSPRI, SSI and PROFAD questionnaires and a 0–10 patient global assessment (PGA). Correlations between each symptom and PGA were obtained. Multiple regression modelling, using PGA as ‘gold standard’ was used to select domains and estimate their weights.
Results PGA had good correlation with dryness, limb pain, fatigue and mental fatigue (r=0.49–0.59, all p<0.0001), but correlated less well with individual dryness features. In multivariate analysis, dryness, limb pain and fatigue, but not mental fatigue, were significantly associated with PGA; weights derived from the regression were identical for these three domains. Thus, ESSPRI was redefined as the mean of the three scales: dryness, limb pain and fatigue. Lastly, ESSPRI significantly correlated with PGA (r=0.70), PROFAD (r=0.73) and SSI (r=0.66).
Conclusion ESSPRI is a very simple index designed to measure patients' symptoms in primary SS. It has good construct validity and is well correlated with SSI and PROFAD. ESSPRI should now be validated for use as an outcome measure in clinical trials.
Statistics from Altmetric.com
Primary Sjögren's syndrome (SS) is a systemic disorder characterised by lymphocytic infiltration and progressive destruction of exocrine glands. The inflammatory process extends beyond the exocrine glands and can potentially affect any organ. As a result, clinical features can be divided into two facets: (1) benign but disabling patients' symptoms such as dryness, pain and fatigue that affect most patients and (2) systemic potentially severe manifestations that affect 20–40% of patients.
Since evidence-based evaluation of treatments has became important to conduct clinical trials and for clinical evaluation, great efforts have been made to determine a core set of outcome measure in primary SS. This core set includes both patients' symptoms (sicca features, fatigue, health-related quality of life) and systemic activity (composite activity score and laboratory measures).1 2
Different indexes have then been developed for evaluation of both disease facets: (1) for patients' symptoms, such as Profile of Fatigue and Discomfort (PROFAD) and Sicca Symptoms Inventory (SSI)3 4 and (2) for systemic features, such as SS Disease Activity Index5 and Sjögren's Systemic Clinical Activity Index.6 However, theses scores are either non-exhaustive5 or quite long.3 6 Thus, the European League Against Rheumatism (EULAR) has sponsored an international collaboration aiming to develop consensus disease activity indexes, one for each facet. We previously developed a consensus clinical index to assess disease activity in patients with systemic complications of primary SS: the EULAR SS Disease Activity Index (ESSDAI).7 This tool was designed for clinicians to assess systemic activity of patients with primary SS and was not designed to evaluate patients' symptoms and complaints.
This study aims to develop a patient-administered questionnaire to assess patients' symptoms, the EULAR SS Patient Reported Index (ESSPRI). This index was developed following a multinational collaboration and used the patient global assessment (PGA) of disease activity as a ‘gold standard’. As for the ESSDAI, the aim was to develop a tool to be used in both clinical trials and daily clinical practice.
Patients and methods
Patient recruitment
Between 4 December 2008 and 30 November 2009, 230 patients were included by 21 primary SS experts from 12 countries (UK, France, Italy, Germany, The Netherlands, Slovenia, Norway, Spain, Sweden, Argentina, Greece and USA) participating in this international EULAR collaborative project (project code CLI 010). All patients fulfilled EU–USA consensus group criteria.8 This study was conducted with the approval of the institutional review board of GHU Paris Nord (n° IRB0006477). Depending on local rules, ethical approval was obtained in other countries, when necessary. In each country, local ethical constraints were observed.
Selection of items
In previous studies developing the PROFAD and SSI, patients' interviews were conducted to identify the main symptoms and complaints in patients with primary SS. Dryness, discomfort (including pain), global fatigue and mental fatigue were identified as being the main symptoms of patients with primary SS.3 4 For sicca features, six components were identified as affecting patients with primary SS: ocular, oral, skin, nasal, tracheal and vaginal.
Measurement
It was expected that a single 0–10 numerical scale for each of the four domains was sufficient to assess patients' symptoms. These four scales were gathered to form the ESSPRI. All patients completed the ESSPRI questionnaires. In addition, patients were asked to rate individually the severity of each dryness feature (ocular, oral, skin, nasal, tracheal and vaginal) and to evaluate the global severity of their symptoms related to their primary SS (PGA) using a 0–10 numerical scale for each individual domain. Patients had to select, among all dryness features and among the four ESSPRI domains, the one they considered to be most in need of improvement. They were also asked to rate, independently of the severity of their symptoms, how important it was for them to get rid of each four ESSPRI domains using a 0–10 numerical scale. Patients assessed, on a 0–10 scale the difficulty they experienced in completing all these questions. Finally, patients also completed the SSI and PROFAD. All questionnaires were translated locally into the different languages, by two of the local experts of the panel.
Statistical analyses
Derivation of indices
PGA of symptom severity was used as a ‘gold standard’. Bivariate analysis involved Pearson's correlation between PGA and each domain and dryness feature, separately. Domains that were significantly correlated with PGA were entered into multivariate models using multiple linear regression modelling. The PGA was used as a dependent variable and items as explanatory variables. Different models were tested. The final ESSPRI score was selected among criteria depending on both statistical properties and clinical relevance. With a similar process, using overall dryness scale as dependent variable and each separate dryness feature as explanatory variable, we derived a score that determined, among all dryness features which ones contributed to the evaluation of the overall dryness: the EULAR Sicca Score (ESS). For both scores, the weights assigned to each domain were derived from the regression coefficients of the multivariate model and rounded to form simplified indices.
Preliminary validation
To assess the content validity, correlations were obtained between each separate scale of the questionnaire and the matching SSI or PROFAD subscales. The ESSPRI was then calculated for all patients. Construct validity was assessed by the strength of correlation of the ESSPRI with PGA, and PROFAD and SSI.
For all statistical analyses, a p value <0.05 was considered statistically significant. All statistical analyses involved use of SAS release 9.1 and R release 2.2.1 statistical software packages.
Results
Patients' characteristics
Two hundred and thirty patients (219 (95.2%) women) were included with a mean age of 55.9 ± 13.9 years and mean disease duration of 8.3 ± 5.6 years. One hundred and forty (60.9%) had past or present systemic involvement and 184 (80.0%) were anti-SSA and/or SSB positive (table 1).
Characteristics of patients with primary Sjögren's syndrome
Priority symptoms: the patient's perspective
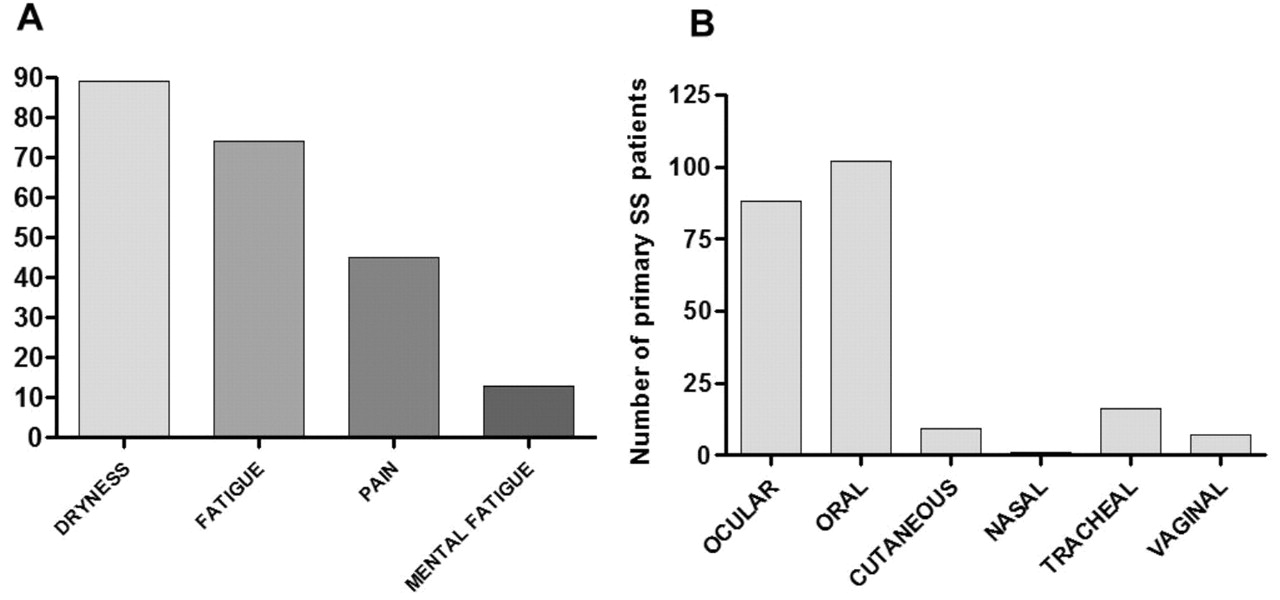
Dryness, fatigue and limb pain were considered to be the symptom the most in need of improvement by 89 (38.7%), 74 (32.2%) and 45 (19.6%) patients, respectively; whereas mental fatigue was considered to be a priority by a minority of patients (figure 1A) and also the symptom the least in need of improvement by 109 (47.4%) patients. In addition, plots of intensity against importance of each symptom improvement showed that dryness, pain and fatigue were considered as being extremely important by 40–50% of patients, even those having low intensity for these symptoms (see online supplementary figure). Among dryness features, oral and ocular dryness were considered as being the priority dryness by 102 (44.3%) and 88 (38.3%) patients, respectively. In contrast, cutaneous, tracheal, vaginal and nasal dryness were considered as being a priority by <7% of patients, each (figure 1B).

Symptom (A) and dryness feature (B) selected as being the most in need of improvement for primary Sjögren syndrome (SS) symptoms.
Derivation of the ESSPRI and ESS
In bivariate analysis, PGA had good correlation with dryness, limb pain, fatigue and mental fatigue (r=0.49–0.59, all p<0.0001), but correlated less well with each separate dryness feature (r=0.38–0.48), except ocular dryness (r=0.54; table 2). Different multivariate models were evaluated, the final model was selected for its statistical properties, clinical relevance and ease of use (table 3). In this model, dryness, limb pain and fatigue, but not mental fatigue, were significantly associated with PGA; weights derived from the regression were identical for these three domains. Thus, ESSPRI (score ranging from 0 to 10) was redefined as the mean of the three scales: (dryness + limb pain + fatigue)/3.
Correlations between ESSPRI, patient global assessment, patients' symptoms and other primary SS scores
Comparisons of different models for derivation of the EULAR Sjögren's Syndrome Patient Reported Index (ESSPRI)
Both ocular (r=0.65) and oral (r=0.76) dryness were more strongly correlated with overall dryness than other dryness features (r between 0.47 and 0.49; all p<0.0001). Even if all dryness features were significantly correlated with overall dryness in univariate analysis, multivariate analyses retained only ocular and oral dryness as independent determinants of overall dryness (table 4). The dryness score was defined as follows: ESS (score ranging from 0 to 10) = (2 × oral dryness + ocular dryness)/3.
Derivation of the EULAR Sicca Score (ESS)
Preliminary validation
Content validity
Each separate dryness scale correlated strongly with the matching SSI subscale (r=0.77, 0.66, 0.71 and 0.84 for ocular, oral, cutaneous and vaginal dryness, respectively; p<0.0001). Similarly, fatigue and mental fatigue were highly correlated with equivalent PROFAD domains (r=0.79 for both; p<0.0001), and also with each other (r=0.69; p<0.0001). The ESSPRI articular scale was also strongly correlated with PROFAD articular domain (r=0.77; p<0.0001).
Construct validity
ESSPRI scores were significantly correlated with PGA (r=0.70; figure 2), PROFAD (r=0.73) and SSI (r=0.66). Also the ESS had good correlation with overall dryness (r=0.80), SSI (r=0.70) and less with other global tools such as PGA (r=0.54), PROFAD (r=0.45) and ESSPRI (r=0.62), which confirms that this tool preferentially measures dryness features. In addition, most patients found the whole ESSPRI questionnaires easy to complete with a mean evaluation of difficulty of 2.29 ± 2.42 on a 0–10 scale; with a score ≤3 for 167 (72.6%) patients.

{kind=link}
{kind=link}
Construct validity of EULAR Sjögren's Syndrome Patient Reported Index (ESSPRI): plots of correlation with patient global assessment (A), Sicca Symptoms Inventory (SSI) (B) and Profile of Fatigue and Discomfort (PROFAD) (C).
Discussion
The ESSPRI is a patient-reported index designed to assess the severity of patients' symptoms in primary SS. This index was modelled by the judgement of a multinational panel of patients from European, North and South American countries. This methodology ensured the inclusion of different transcultural patients' views on the severity and the importance of their symptoms. Compared with the PGA, and the existing tools PROFAD, SSI, the ESSPRI performed satisfactorily for evaluation of patients' symptoms in primary SS, and has the advantage that it is easy to use.
Since correlation between objective measures of dryness and symptoms is poor,4 9 the evaluation of symptoms, along with objective measures such as Schirmer's test and salivary flow, is necessary. Furthermore, the choice of the best objective measure for oral dryness (basal or stimulated salivary flow) or for ocular dryness (Schirmer's test or ocular surface damage score after fluorescein staining) is still unresolved. In addition, it is still unclear whether these objectives measures of dryness are markers of disease damage or activity. Finally, in most cases, all these objective features had modest variations over time and therefore did not clearly exhibit a sufficient sensitivity to change.10,–,13 In this debate, recent-onset symptoms and/or disease should probably be differentiated from longlasting stable features of disease, as suggested by a possible improvement of subjective and objective dryness measures with new treatments, including B-cell targeted therapies in recent trials.14,–,16 Thus, these observations emphasised the need for a subjective evaluation of symptoms by patients themselves in addition to objective measures of dryness. This study did not involve objective assessment of dryness. A comparison of subjective and objectives measures is planned in the prospective validation of the EULAR scores, where evaluations will be performed at two time points.
Until now, two disease-specific scores existed to assess patients' symptoms in primary SS—namely, the SSI for evaluation of dryness features and the PROFAD for fatigue and discomfort. However, no global score was available. Therefore, we herein developed a global score, the ESSPRI, able to capture all important and disabling symptoms of the disease, including those of the core set. Having such a global score will be a consistent help to design and conduct of clinical trials in primary SS. In addition, each component of the ESSPRI, measured with a single 0–10 numerical scale, was highly correlated with the corresponding PROFAD and SSI domain. This suggests that compared with a long list of items, a single numerical scale is sufficient to measure each of the symptoms without loss of content validity. Also, the ESSPRI is extremely easy to calculate, and is even easier to use than the 28-joint count Disease Activity Index routinely used in rheumatoid arthritis,17 and the recently published short form of PROFAD-SSI,18 which is essential for its use in clinical practice.
In this study, as in others,19 20 dryness was the predominant complaint of patients with primary SS. Each component of dryness was highly correlated to similar domains of the SSI; the least correlated domain was oral dryness, but in the SSI this domain includes tracheal and nasal dryness, which were evaluated separately in our questionnaires. Compared with the ESSPRI, which include a unique overall evaluation of dryness, the SSI evaluates separately each dryness feature. In the SSI, even if oral and ocular domains include respectively five and three items, they have the same weight on the final score as cutaneous and vaginal dryness. However, we clearly showed that among all dryness features, oral and ocular dryness were far and away the most important features to patients with primary SS, compared with nasal, tracheal and vaginal dryness. Also, these two components were the only ones that contributed to patient evaluation of overall dryness intensity and severity, in multivariate analysis. Therefore, except in particular settings and conditions, evaluation of overall, oral and ocular dryness is probably sufficient to address important dryness features. In addition, we derived from our analyses a simple dryness score including these two components that could be useful for assessing the efficacy of secretogogues.
Our method of questionnaire translation differed from that usually used when scores are developed in one country and then translated to be validated in other countries. In this study, the translations were performed initially before the development, then the ESSPRI was simultaneously developed in a large number of countries and languages, and these different versions will be finally validated in a large prospective study. In addition, the questions included in the ESSPRI were simple (PGA and 0–10 anchored scales for pain, fatigue and dryness) and have been already been translated for use in other scores; this is a quite different situation from quality-of-life questionnaires where translation of each question may be debatable. For all these reasons, we did not perform back translations.
Together with evaluation of symptom severity, we here assessed their importance and, particularly, the perceived need for each symptom to be improved. With this methodology we selected the more relevant domains and symptoms from a patient's perspective. Therefore, the selection of the ‘best’ model for ESSPRI was based on its statistical performance together with the clinical relevance of its domains. Effectively, model 1, which included ocular dryness and overall dryness, was not selected because of item redundancy, and model 2, including mental fatigue, was not retained, although it had similar properties to the selected model, because mental fatigue was shown to be the least important symptom (figure 1). In this study a larger number of patients were included than in previous studies, coming from different countries. This large and transcultural panel of patients ensures inclusion of a wide spectrum of patients' views of the disease symptoms. Both these facets enhance the content validity of the ESSPRI.
ESSPRI is a patient index designed to measure patients' symptoms in primary SS. ESSPRI content validity was ensured by participation of a large multinational panel of patients with primary SS. This very simple index has good construct validity when PGA is considered as the ‘gold standard’ and good correlations with more complicated validated indexes such as the SSI and PROFAD. ESSPRI should now be evaluated for sensitivity to change and validated in association with ESSDAI to be used as an outcome measure in clinical trials and clinical practice. These both indexes ESSPRI and ESSDAI are designed to be complementary and should be used together to assess all disease facets.
Acknowledgments
The authors thank Maxime Dougados, Alan Tyndall and Iain McInnes for their guidance and support. We thank the EULAR house in Zurich for their hospitality and outstanding organisation (Ernst Isler, Anja Schönbächler and their associates). We also thank the other members of the EULAR Sjögren's task force who helped us with patient recruitment: John Hamburger and Andrea Richards, Birmingham Dental Hospital & School, Saaeha Rauz, Academic Unit of Ophthalmology, University of Birmingham, Birmingham UK; Emmanuel Chatelus, Strasbourg University Hospital, Strasbourg, France.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
{kind=link}
Footnotes
-
Funding This project was supported by a grant from EULAR.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the institutional review board of Paris North Hospitals, Paris 7 University, AP-HP (N° IRB0006477).
-
Provenance and peer review Not commissioned; externally peer reviewed.