Article Text

Abstract
Objectives To agree terminology and to develop recommendations for the diagnosis of calcium pyrophosphate deposition (CPPD).
Methods The European League Against Rheumatism (EULAR) CPPD Task Force, comprising 15 experts from 10 countries, agreed the terms and recommendations for diagnosis of CPPD using a Delphi consensus approach. Evidence was systematically reviewed and presented in terms of sensitivity, specificity and positive likelihood ratio (LR) to support diagnosis; ORs were used for association. Strength of recommendation (SOR) was assessed by the EULAR visual analogue scale.
Results It was agreed that ‘CPPD’ should be the umbrella term that includes acute calcium pyrophosphate (CPP) crystal arthritis, osteoarthritis (OA) with CPPD and chronic CPP crystal inflammatory arthritis. Chondrocalcinosis (CC) defines cartilage calcification, most commonly due to CPPD and detected by imaging or histological examination. A total of 11 key recommendations were generated on the topics of clinical features, synovial fluid (SF) examination, imaging, comorbidities and risk factors. Definitive diagnosis of CPPD relies on identification of SF CPP crystals. Rapid onset inflammatory symptoms and signs are suggestive but not definitive for acute CPP crystal arthritis. Radiographic CC is not highly sensitive or specific, whereas ultrasonography appears more useful (LR=24.2, 95% CI 3.51 to 168.01) for peripheral joints. Recognised risk factors for CPPD include ageing, OA and metabolic conditions such as primary hyperparathyroidism, haemochromatosis and hypomagnesaemia; familial forms are rare. SORs varied from 53 to 99 (maximum 100).
Conclusion New terms for CPPD were agreed and 11 key recommendations for diagnosis of CPPD were developed using research evidence and expert consensus.
Statistics from Altmetric.com
Introduction
Calcium pyrophosphate deposition (CPPD) occurs almost exclusively in articular tissues, most commonly fibrocartilage and hyaline cartilage,1 and is the most common cause of chondrocalcinosis (CC). Calcium pyrophosphate (CPP) associated arthritis is the third most common inflammatory arthritis.2 Recognised risk factors are ageing, osteoarthritis (OA), previous joint trauma/injury, metabolic disease and familial predisposition.3 ,4
The complexity of CPPD in terms of variable phenotypes is compounded by use of different terminologies and classification. In 1961 McCarty and colleagues first identified CPP crystals in synovial fluid (SF) from knees of patients with acute synovitis and CC,5 introducing the term ‘CPPD’ for ‘calcium pyrophosphate dihydrate’ crystals.6 Similarity to gout prompted the term ‘pseudogout’ for this ‘crystal-induced arthropathy’. Subsequently other presentations were recognised, many appearing to mimic other forms of arthritis, encouraging proliferation of ‘pseudo’ syndromes and a complex clinical classification of ‘pseudogout’ (type A), ‘pseudo-rheumatoid arthritis’ (type B), ‘pseudo-osteoarthritis’ (with acute attacks, type C; without inflammation, type D), ‘lanthanic or asymptomatic’ (type E) and ‘pseudoneuropathic’ (type F), to which other forms were later added.7 The term ‘CPPD crystal deposition disease’ was introduced to incorporate all instances of CPP deposition, even though CPPD does not always appear injurious or causal in ‘disease’. The term ‘pyrophosphate arthropathy’ (PA) was later used, particularly in Europe, for CPPD with accompanying structural arthritis.4 However, some clinicians use the terms CC or pseudogout for any phenotype, whereas others restrict CC for radiographic calcification, pseudogout for acute synovitis and PA for CPPD plus OA.3 ,8
The group that developed European League Against Rheumatism (EULAR) recommendations for gout9 ,10 considered it desirable to agree a uniform terminology for CPPD and to address issues relating to diagnosis and management. Therefore, the EULAR CPPD Task Force was formed to produce evidence-based recommendations using a combined systematic review and expert consensus approach.11 Part I, terminology and diagnosis, is presented here.
Methods
Expert consensus
The Task Force comprised 15 experts from 10 countries. A meeting was organised to agree terminology; subsequently, preagreed terms were circulated for voting. Each participant independently submitted up to 10 propositions on key aspects of diagnosis; consensus was reached using the Delphi technique.9 ,12 A second meeting was organised to discuss recommendations and supporting evidence and to score strength of recommendations (SORs).13 ,14
Systematic review of research evidence
As with previous projects,9 research evidence for each proposition was systematically searched (January 1950 to January 2009). Search terms included: calcium pyrophosphate dihydrate and/or deposition, CC, PA, pseudogout, crystal associated diseases/arthropathy/arthritis, crystal deposition diseases and calcium crystals. Studies informing diagnosis of CPPD were included. Case reports, reviews, editorials and commentaries were excluded.
Wherever possible, sensitivity, specificity, likelihood ratios (LR), probability of CPPD and reliability (κ or intraclass correlation coefficient) were calculated for diagnostic tests; RRs or ORs were estimated for association.9 Statistical pooling was undertaken as appropriate and a random effects model was used for heterogenous results.15 The EULAR level of evidence (LOE) for diagnosis,9 and EULAR 0–100 mm visual analogue scale (VAS)13 ,14 were used to rank LOE and SOR.
Future research agenda
After the second meeting each participant submitted independently up to 10 future research propositions; consensus was obtained by the Delphi technique.
Results
Terminology of CPPD and its related conditions
The following terms and definitions were agreed:
CPP crystals: the simplified term for calcium pyrophosphate dihydrate crystals (similar to ‘sodium urate’ for monosodium urate monohydrate crystals)
CPPD: the umbrella term for all instances of CPP crystal occurrence.
CC: cartilage calcification, identified by imaging or histological examination. This is not always due to CPPD and may occur as an isolated finding in an apparently otherwise normal joint or coexist with structural changes resembling OA.
Clinical presentations associated with CPPD:
▶ Asymptomatic CPPD: CPPD with no apparent clinical consequence. This may be isolated CC, or OA with CC. Often this is identified incidentally following imaging for other reasons.
▶ OA with CPPD: CPPD in a joint that also shows changes of OA, on imaging or histological examination.
▶ Acute CPP crystal arthritis: acute onset, self-limiting synovitis with CPPD (replacing the term ‘pseudogout’).
▶ Chronic CPP crystal inflammatory arthritis: chronic inflammatory arthritis associated with CPPD.
Risk factors that, if present, may be noted in phenotype characterisation:
▶ Previous joint injury.
▶ Hereditary/familial predisposition to CPPD.
▶ Specific diseases (eg, haemochromatosis, primary hyperparathyroidism, hypophosphatasia, hypomagnesaemia).
EULAR recommendations
Of 102 initial propositions, 11 were agreed after 2 Delphi rounds. Recommendations covered four domains: clinical features, SF, imaging and risk factors/associations (see table 1 for the full propositions). Evidence regarding validity for each test/feature are summarised in table 2, and risk factors and associations in table 3.
Propositions and strength of recommendation (SOR), ordered according to topic (clinical features, synovial fluid, imaging, comorbidities and risk factors)
Validity of diagnostic tests for calcium pyrophosphate deposition (CPPD)
Risk factors and comorbidities associated with calcium pyrophosphate deposition (CPPD)
Clinical features
Proposition 1 (also see detailed proposition in table 1)
CC may be an apparently isolated phenomenon or occur with structural changes of OA.16,–,18 Hospital-based series suggest that OA with CPPD may differ from OA without CPPD in showing more osteophytosis,18,–,21 different joint involvement22,–,26 and more inflammatory features (table 3). However, whether OA with CPPD is a distinct OA ‘subset’ remains unclear. Isolated CC and OA with CPPD may be clinically occult or associate with acute CPP crystal arthritis; OA with CPPD may also associate with pain, stiffness and functional limitation. Much less commonly, atypical or periarticular CPPD may associate with tendinitis,27 tenosynovitis,28 bursitis,29 tumorous CPPD30 or syndromes relating to spinal involvement31
Proposition 2
Direct literature evidence to support this recommendation was not found. However, one nested case-control study of postmeniscectomy knees showed those with CC had five times more risk (LR=5.00, 95% CI 2.27 to 11.02) of self-limiting acute attacks compared to those without CC.32 One hospital series observed that in acute CPP crystal arthritis symptoms and signs usually resolve within 3–4 days.33 Rapid development of acute synovitis with pain, stiffness, swelling/effusion and marked tenderness (±erythema) is highly characteristic of crystal synovitis but these features are not specific to one crystal9 so crystal identification is required for precise diagnosis.
Proposition 3
A community cross-sectional survey in Sweden found that CC is most common in knees (8.5%), then wrists (5.1%) and hands (1.7%).34 Prevalence of knee CC in this study was similar to that in the USA (8.1%)17 and UK (7.0%)18 studies so this distribution may be generalisable to other populations. Several hospital series report similar distribution but greater prevalence for each joint1 ,35 ,36 (figure 1). The glenohumeral joint appears less commonly affected.35

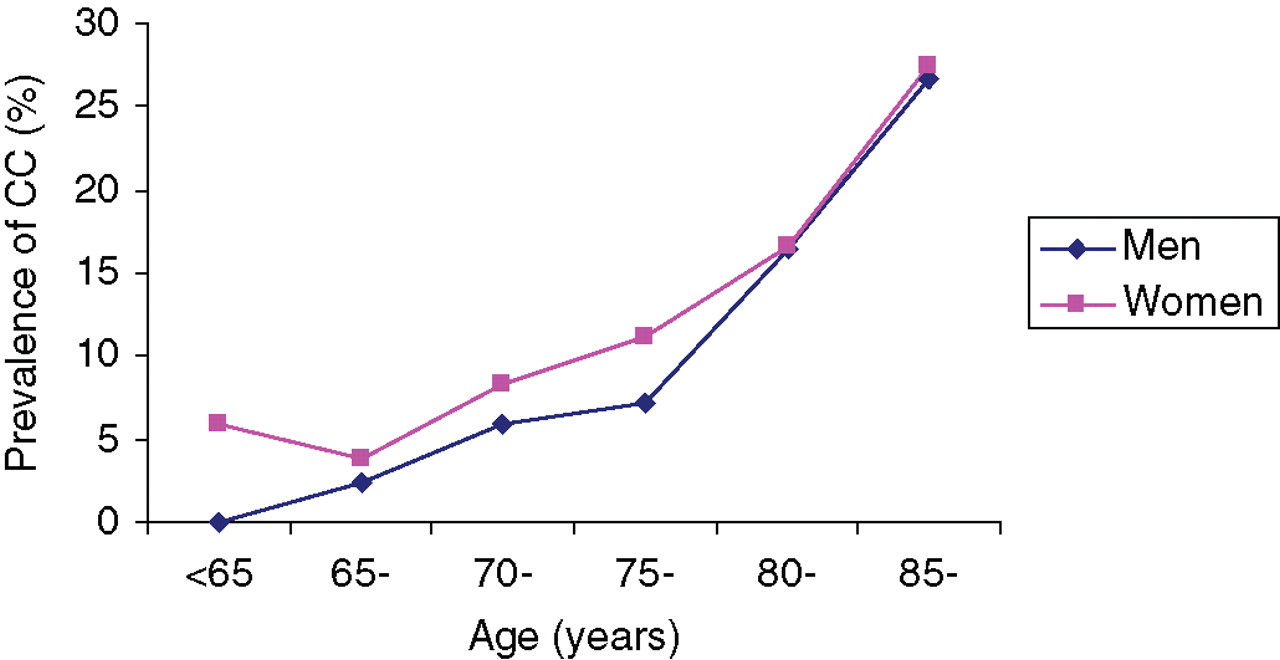
Ageing is a major risk factor. CPPD is rare under age 50,18 but increases dramatically afterwards2 ,17 ,18 ,36,–,40 (figure 2). The risk doubles every decade between 45 and 85 years (OR=2.25, 95% CI 1.79 to 2.82) independently of other risk factors.41 CPPD under age 45 should raise the possibility of familial42 ,18 ,43 or metabolic disease predisposition, especially if polyarticular. Gout is the main differential diagnosis of acute CPP crystal arthritis. Gout prevalence also increases with age,9 but the first attack classically involves joints in the feet, (especially first metatarsophalangeal).9 However, the first attack can affect the knee, and rarely the wrist, but the relative likelihood of urate or CPP crystal-induced synovitis according to site and age has not been calculated. Radiographic CC is often taken as a surrogate for CPPD but does not necessarily predict SF CPP crystal identification according to limited evidence for the wrist44 (table 2) and the knee.35 ,45 Definitive diagnosis of CPPD has to be crystal proven usually by examination of SF (occasionally histological).

Prevalence of knee chondrocalcinosis by age and gender (data obtained from Felson et al 198917).
Proposition 4
The knee is a target site for OA46,–,48 and the most common site for CPPD1 ,34,–,36 (figure 1). A total of 4 cross-sectional and 5 case-control studies (4517 subjects in all) provided quantitative data for analysis of the association between OA and CPPD.1 ,17 ,18 ,20 ,38 ,49,–,52 The pooled OR was 2.66 (95% CI 2.00 to 3.54). Results were consistent between cross-sectional (2.52, 95% CI 1.86 to 3.44) and case-control (2.80, 95% CI 1.44 to 5.47) studies, suggesting people with OA are three times more likely to have CPPD.
CPPD may associate with more inflammatory features (eg, pain, stiffness, effusion, more severe pain and disability) and more rapid progression53 than in knees without CPPD, but the associations are marginal and not useful for diagnosis (table 2).
CPPD may associate with an atypical distribution of OA. Compared with isolated OA, OA with CPPD may occur in less typical locations (eg, radiocarpal joints, elbows) and show more patellofemoral compartment involvement.22 ,26 ,25 Triangular fibrocartilage CC and calcification of intrinsic carpal ligaments (particularly lunotriquetral) and capsules is also seen;24 calcification of the gastrocnemius tendon origin may also associate with CPPD in knees.25 Other sites of CC include the pubic symphysis and hip labrum.23 It is unknown whether CPPD within an individual associates with atypical OA (systemic association), or whether atypical OA only occurs in joints with CPPD (local association).
Whether osteophytosis is a characteristic of CPPD is unclear. One community study found the main association between OA and CC was with osteophyte, not joint space narrowing (JSN).18 This is supported by some19,–,21 but not other studies.54 ,55 Overall pooled ORs were 1.26 (95% CI 0.76 to 2.09) for osteophyte and 1.24 (95% CI 0.91 to 1.69) for JSN (table 3). However, studies for osteophyte were heterogeneous (p=0.0004) whereas those for JSN were homogenous (p=0.10). Similarly the association with cysts remains uncertain (OR=2.94, 95% CI 0.92 to 4.96) (table 3).
Proposition 5
Although the population prevalence is unknown, hospital series of chronic CPP crystal inflammatory arthritis show that most are mono/oligoarthritis (89%) though some (11%) are polyarticular.35 There may be non-specific elevation of C reactive protein and erythrocyte sedimentation rate33 but diagnostically, identification of CC is more useful since this mainly results from CPPD and is less likely to occur with rheumatoid arthritis (OR=0.18, 95% CI 0.08 to 0.41)38 ,56 (table 3). Nevertheless, definitive diagnosis relies on CPP crystal identification, usually in SF.
SF examination
Proposition 6
Identification of SF CPP crystals (usually by light, compensated polarised light or phase contrast microscopy) is the recommended reference standard for diagnosis of CPP crystal-associated arthritis (figure 3). First suggested by McCarty in 1962,57 this has been used repeatedly as a major diagnostic feature for CPP syndromes.4 Its validity and reliability have been systematically reviewed.58 Training in SF CPP crystal identification results in better sensitivity (0.95, 95% CI 0.92 to 1.02) and reasonable specificity (0.86, 95% CI 0.80 to 0.93) compared to expert (‘gold standard’) identification 59(table 2). Trained observer reliability is very good (κ=0.79, 95% CI not reported).59 No quantitative cut-off of crystals is recommended; even one or a few crystals are clinically significant. The more characteristic the crystal morphology, the more confident the diagnosis.

Synovial fluid calcium pyrophosphate crystals (phase contrast, 1000×).
Proposition 7
Although there are no specific studies, examination of SF for CPP crystals should be undertaken for any undiagnosed inflammatory arthritis since CPPD is a common cause of joint inflammation2 and may present atypically.
Imaging
Proposition 8
Radiographic CC is a useful imaging marker, often taken as a surrogate for CPPD (figure 4), but common discordance with positive SF crystal identification reduces its diagnostic usefulness.35 ,44 ,45 ,60 Detection of CC in proven cases of CPP crystal arthritis varies from 29% to 93% depending on population and joint examined.35 ,44 ,45 ,60 The sensitivity and specificity of CC against the ‘gold’ standard remain unknown. However, one small case control study (n=18)44 suggested that at the wrist CC is neither sensitive (0.29) nor specific (0.20) for diagnosis (table 2); the likelihood of a patient with wrist CC having SF CPP crystals identified was only 3%. However, results of this small study may not be generalisable and further studies are required.

Radiographic chondrocalcinosis of hyaline cartilage and fibrocartilage at the knee, occurring as an isolated phenomenon in an otherwise normal joint (above) and in association with changes (marginal osteophyte, medial compartment narrowing) of osteoarthritis (below).
There are several possible reasons for discordance between CC and SF crystal positivity including: lack of specificity of CC for CPPD (basic calcium phosphates may also cause this); low sensitivity of radiographs for detecting CC; possible greater difficulty in identifying small numbers of SF CPP crystals in situations other than acute CPP crystal synovitis (especially when there is isolated CC and no cartilage fibrillation to encourage crystal shedding); and reduced ability to identify CC when there is significant cartilage loss. Also being small and weakly, or non-birefringent,61 CPP crystals may be underdetected.
Proposition 9
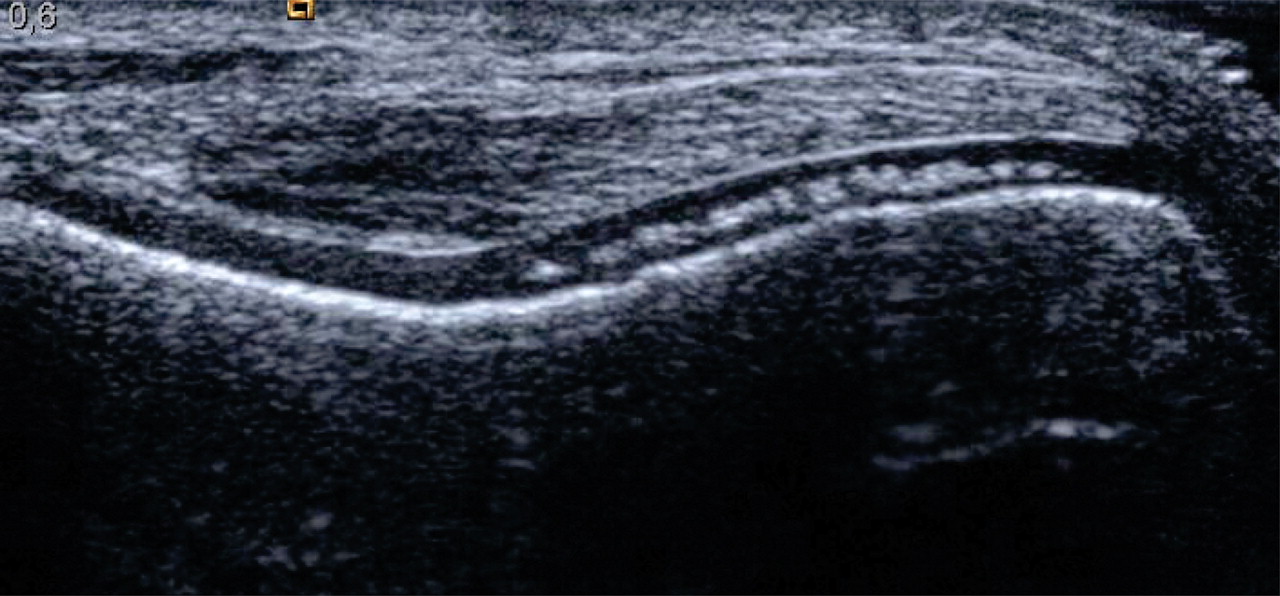
Case-control studies have examined the usefulness of ultrasonography (US) in detecting calcification in knees (figure 5),62 ,63 wrists and shoulders.63 US of the knee appears sensitive (0.87, 95% CI 0.69 to 1.04) and specific (0.96, 95% CI 0.90 to 1.03) for detection of SF CPP crystals.62 Positive US findings may strongly suggest the diagnosis of CPPD (LR=24.2, 95% CI 3.51 to 168.01). Given a positive US result, the likelihood of a patient having SF CPP crystals in the same joint (eg, knee) in the UK population, for example, would be 65%. Suitability of US to detect calcification varies between sites (table 2) and it is insensitive for deep structures (eg, spine). One direct comparison showed US to be more sensitive (100%) than x-rays (82%) in identifying CPPD.63 However, although US seems a promising technique for crystal identification the few published studies emanate from just a few centres and further studies are required.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ultrasound of knee showing hyperechogenicity of the midzone of femoral hyaline cartilage, consistent with chondrocalcionosis due to calcium pyrophosphate (CPP) crystals.
Comorbidities and risk factors
Proposition 10
One study in a tertiary centre retrospectively reviewed all cases with crystal positive SF samples identified over a 7-year period. Of 265 positive samples, 183 (69.0%) contained MSU crystals, 81 (30.6%) contained CPP crystals and 1 (0.4%) contained both. Four (1.5%) also had positive cultures; of these, three were from joints with CPP crystals64.
Proposition 11
As discussed,3 ,4 OA and ageing are major risk factors/associations for CPPD. There are common risk factors for OA and CPPD (eg, ageing, joint injury) but OA cartilage also directly encourages deposition of calcium crystals (basic calcium phosphates as well as CPP).65 Conversely, CPPD could be a primary factor that causes, or amplifies joint damage in OA.65Whether gender influences CPPD remains controversial, but pooling of eight cross sectional/case-control studies yields a non-significant association (OR=0.89, 95% CI 0.58 to 1.38). Although body mass index is a major risk factor for OA, there is no evidence of association with CPPD (table 3).
Previous joint injury may predispose to CPPD. One retrospective cohort study found the risk of CC in postmeniscectomy knees to be five times greater (OR=5.00, 95% CI 1.77 to 14.11) than in contralateral unoperated knees32 (table 3).
Several studies have investigated the association between CPPD and primary hyperparathyroidism, of which five provided data to summarise the association.40 ,66,–,69 Patients with hyperparathyroidism are three times more likely to have CPPD than controls (OR=3.03, 95% CI 1.15 to 8.02) (table 3).
Evidence for the association between haemochromatosis and CPPD is relatively sparse. One hospital case-control study found no significant association (OR=1.04, 95% CI 0.42 to 2.60), although patients with haemochromatosis developed CPPD at a younger age (<60) than those without haemochromatosis (OR=3.05, 95% CI 1.12 to 8.33).67 In a study of 178 patients with untreated haemochromatosis (mean age 50 years) prevalence of CC was 30% and the number of joints with CC correlated positively with age, ferritin level and serum parathyroid hormone 44–68 pg/ml.70 In another hospital series of 54 patients with idiopathic haemochromatosis, (mean age 56, range 39–74 years), 31 (57%) had arthropathy which significantly associated with CC (OR=6.81, 95% CI 2.02 to 22.95)71.
Hypomagnesaemia associates with increased risk of CPPD. A case control study of 72 patients with chronic intestinal failure and 72 age and gender matched controls demonstrated increased risk of CC (OR=13.5, 95% CI 2.76 to 127.3) in those with intestinal failure.72 Diuretic use was a risk factor for CC in one community study18 and this might be explained by diuretic-induced hypomagnesaemia (table 3). Case reports and hospital series support associations with rare diseases such as hypophosphatasia.73 ,74
Although relatively uncommon, screening for hyperparathyroidism, haemochromatosis and hypomagnesaemia may be considered in patients with CPPD, and patients with these conditions are a high-risk population for CPPD.
Although rare families with young-onset polyarticular CPPD and monogenic inheritance pattern are recognised,75 current evidence does not support familial aggregation for patients with common CC (OR=1.10, 95% CI 0.58 to 2.08).41 ,76 However, a positive family history may relate to an earlier onset of CPPD.76
Future research agenda
After four Delphi rounds five propositions were agreed.
Whether there are significant differences (eg, in symptoms, joint distribution, clinical outcomes) between OA with and without CPPD requires further study.
Clinical studies (using crystal identification as the gold standard for diagnosis) are required to better define the spectrum of CPPD and its possible clinical subsets.
An optimal protocol (including training) and agreed European standard for the identification of CPP crystals in SF needs to be established.
The validity of different imaging techniques for the diagnosis of CPPD should be evaluated, leading to recommendations about their application in routine care.
Further studies are required to determine whether correction of associated metabolic disease (eg, primary hyperparathyroidism, haemochromatosis) influences progression and outcome of CPPD associated arthropathy.
Discussion
A large number of terms are used for CPPD and its clinical phenotypes. However, the plethora of ‘pseudo’ syndromes and inconsistent use of terms such as pseudogout and CC often cause confusion. The EULAR CPPD Task Force therefore suggests ‘calcium pyrophosphate deposition’ (CPPD) as the umbrella term for all instances of CPP crystal deposition. Under this umbrella, asymptomatic CPPD, OA with CPPD, acute CPP crystal arthritis and chronic CPP crystal inflammatory arthritis are included. It was felt that terms prefixed by ‘pseudo’ should be abandoned because they do not specify the causative crystal, are probably not discrete clinical subsets, are a source of potential confusion for patients, and intimate that CPP crystals are of secondary importance and interest compared to sodium urate. The term chondrocalcinosis is retained for cartilage calcification, which is most commonly due to CPPD. It is appreciated that introduction of new terminology may prove inconvenient in the short term, but would be beneficial in the long term for research, education and clinical practice.
There are several limitations to this project. Firstly, we established expert consensus prior to systematic review of research evidence. While this approach addresses clinically relevant questions, it is not comprehensive. Secondly, the recommendations are not intended to classify CPPD for research purposes but to provide recommendations for clinical diagnosis. Thirdly, clinical studies used different gold standards for diagnosis, making comparison between diagnostic tests difficult. Furthermore, research evidence for diagnosis of CPPD is generally sparse and of poor quality. We therefore provided a suggested future research agenda to encourage expansion of the evidence base.
Acknowledgments
We would like to thank the European League Against Rheumatism for financial support, Helen Richardson for coordination, Joanna Ramowski and Amanda Moody for assistance with the literature search and data collection and Daniel McWilliams for help in data analysis.
References
Footnotes
-
Competing interests None.
-
Funding Financial support was received from the European League Against Rheumatism.
-
Provenance and peer review Not commissioned; externally peer reviewed.