Article Text

Abstract
Background Psoriatic arthritis (PsA) recommendations state that the target of treatment should be remission or low disease activity (LDA). We used a real-life dataset to compare different potential targets.
Methods 250 patients with PsA considered in an acceptable disease state according to their rheumatologist were included. Targets for remission were the Disease Activity Index for Psoriatic Arthritis (DAPSA) and clinical DAPSA (cDAPSA) remission (≤4), very low disease activity (VLDA) and Psoriatic Arthritis Disease Activity Score ≤1.9. LDA targets analysed were the DAPSA ≤14, cDAPSA ≤13, minimal disease activity (MDA) and adjusted MDA targets: MDAjoints with both tender joint count (TJC) and swollen joint count (SJC) mandated, MDAskin (psoriasis area and severity index (PASI) mandated) and MDAjoints&skin with TJC, SJC and PASI mandated.
Results Comparison of the several candidate targets demonstrates that VLDA is achieved by the lowest proportion of patients and includes patients with the lowest residual disease activity compared with the other remission targets. The modified MDA measures are the most stringent targets for LDA in terms of residual disease on joints, psoriasis and enthesitis within patients achieving the target. In both remission and LDA, the inclusion of C reactive protein did not show an added value. The exclusion of a skin domain, as in the DAPSA measures, resulted in negligence of skin disease and a negative impact on the quality of life in some patients.
Conclusions The different remission and LDA targets show us significant overlap between measures, but these measures targeting the same definition do differ in terms of allowance of residual disease. Inclusion of laboratory markers seems unnecessary, although exclusion of a skin domain may result in psoriasis not being assessed resulting in residual impactful skin disease.
- psoriatic arthritis
- outcomes research
- disease activity
Statistics from Altmetric.com
Introduction
Treatment guidelines for psoriatic arthritis (PsA) by European League Against Rheumatism and Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) recommend to aim for remission or the lowest possible disease activity in all involved domains of the disease.1 2 Clinical remission in psoriatic arthritis is mostly defined as a complete absence of disease activity, with no signs or symptoms of in all domains of the disease.3 However, the specific target to define remission or low disease activity is not specified further by the treatment recommendations.
It is still under debate what the target to measure the disease state should be. Several composite scores are developed specifically for PsA, most focusing on multiple domains considered important to assess: (1) the minimal disease activity (MDA), which is a seven-component score including skin, enthesitis, tender and swollen joint counts (SJCs) and patient reported domains including pain and global disease activity score as well as the Health Assessment Questionnaire (HAQ),4 5 (2) the Psoriatic Arthritis Disease Activity Score (PASDAS), which includes SJW, enthesitis, dactylitis, skin, C reactive protein (CRP), patient-reported and physician-reported global disease activity and the short form 36 questionnaire (SF-36) questionnaire on physical functioning6 and (3) the Disease Activity Index for Psoriatic Arthritis (DAPSA), which focuses on peripheral arthritis and includes tender and SJCs, CRP and patient-reported pain and global disease activity scoring adjusted later to exclude the CRP, the clinical DAPSA (cDAPSA).7
All three measures can be used to define remission or low disease state. For MDA, a modified version was developed to use as a remission target, the very low disease activity (VLDA).8 Furthermore, adjusted versions of the MDA, with a focus on joint and skin symptoms, were developed. Specific cut-off values to define remission or low disease activity were developed for (c)DAPSA, as well as a cut-off for near remission in PASDAS.9 10 However, little data are published on comparing these measures, and it is unknown if these measures reflect the same clinical disease activity on the various disease domains. We have previously set up a cohort of patients with psoriatic arthritis focusing on a quiescent disease state.11 As the disease targets will be a complimentary tool in clinical practice, this cohort is an ideal group of patients to assess their performance in.
In the present study, we aimed to compare these composite scores proposed as a target for remission or low disease activity in PsA using an existing real-life data set of PsA patients with quiescent disease according to their rheumatologist. We investigated which patients fulfil definitions of these criteria, how much overlap there is in fulfilling the different targets and how much residual disease in the various domains is present in the different composite scores.
Methods
An existing dataset was used: data from a cross-sectional study of 250 PsA patients with quiescent disease according to the treating rheumatologist was used and recruited from routine clinical visits. Patients had to have been on stable treatment for at least 6 months, regardless of therapy. Mean age 55 years, two-thirds of the patients were male, mean disease duration was 12.7 (9.2) years, age at arthritis onset was 42.7 (12.3) years. On group level, disease activity was low, with a mean swollen joint count (SJC) of (median(IQR)) 0 (0–1), tender joint count of 1 (0–5), psoriasis area and severity index (PASI) score of 0.3 (0–1.5), enthesitis present in 17 of 250 patients and dactylitis in 2 of 250 patients. The patients’ characteristics are shown in more detail in see online supplementary file 1.11
Supplementary file 1
Four potential definitions of remission/inactive disease were used where all items required for the definitions were available in this dataset:
VLDA where all seven of the MDA cut points are met: tender joint count (TJC) ≤1; SJC ≤1; enthesitis count ≤1; PASI ≤1; patient global visual analogue scale (VASptGlobal) ≤20 mm; patient pain (VASptPain) ≤15 mm; and HAQ ≤0.5.
DAPSA remission4 where DAPSA ≤4: TJC+SJC+VASptGlobal (cm)+VASptPain (cm)+CRP (mg/L).
cDAPSA remission where cDAPSA ≤4: TJC+SJC+VASptGlobal (cm)+VASptPain (cm).
Near remission in the psoriatic arthritis disease activity score (PASDAS) where PASDAS ≤1.9.
Six potential definitions for low or minimal disease activity were used:
DAPSA low disease (DAPSA=TJC+SJC+bal+VASptPain +CRP) ≤14.
cDAPSA low disease (DAPSA=TJC+SJC+VASptGlobal+ VASptPain) ≤13.
MDA 5/7 where any five of the seven cut points are required to be met.
MDA joints where both the tender and swollen joint count cut points are required to be met with any 3/5 of the remaining cut points (enthesitis, skin, VASptGlobal, VASptPain and HAQ).
MDA skin where skin is required plus 4/6 remaining cut points (TJC, SJC, enthesitis, VASptGlobal, VASptPain and HAQ).
MDA joints and skin where the TJC, SJC and skin cut points are required to be met with any 2/4 of the remaining cut points (enthesitis, VASptGlobal, VASptPain and HAQ).
Proportions achieving each criteria were calculated. The agreement between the tested definitions was established using 2×2 tables and percentage exact agreement (PEA) and calculation of a kappa. The proportion of residual disease was established for key clinical domains of PsA (peripheral arthritis, enthesitis, psoriasis and dactylitis) and levels of systemic inflammation, as measured by CRP, were assessed.
Results
Comparisons of the measures for remission/inactive disease
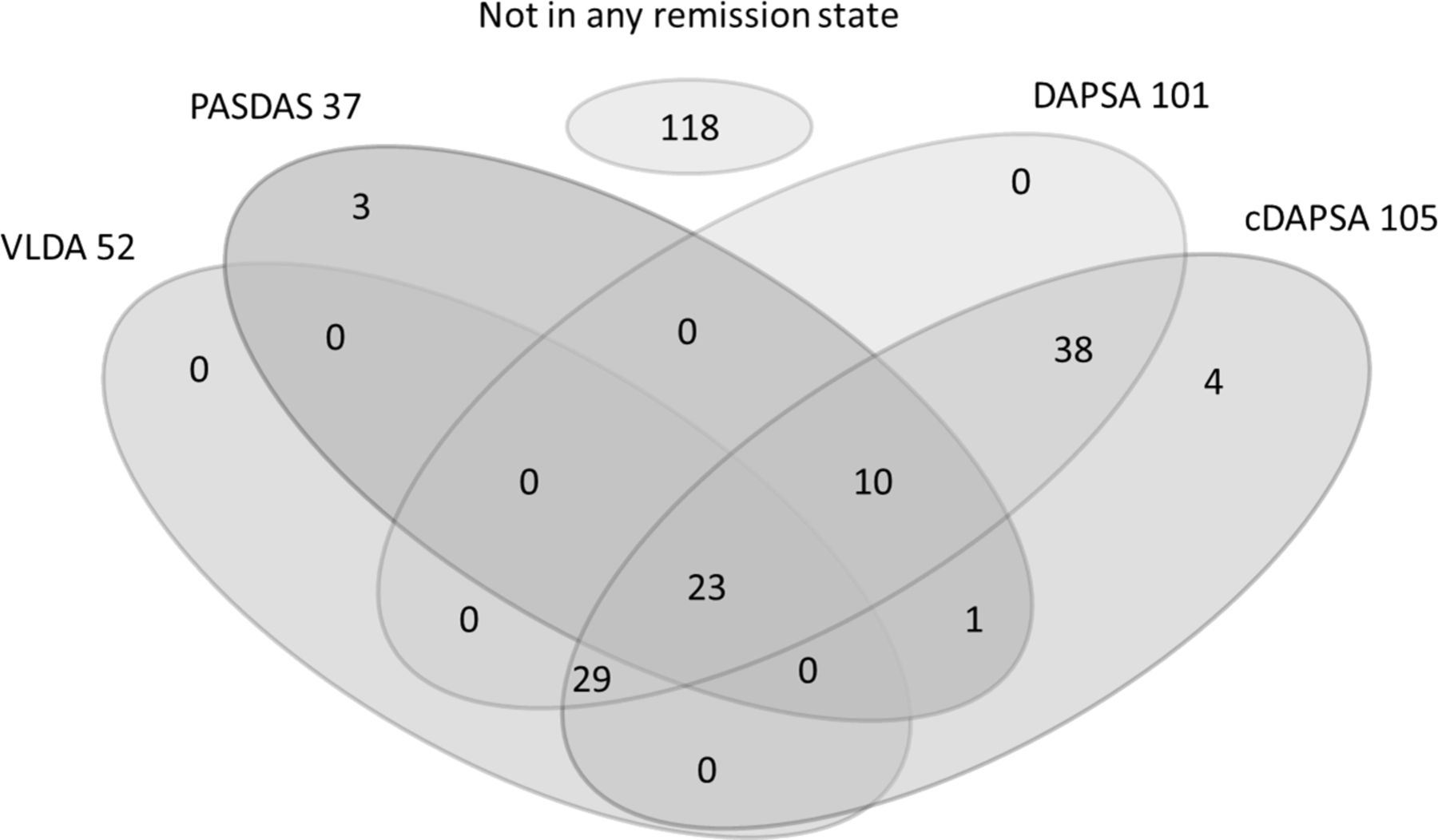
Of the total population (250 patients), 107 (43.7%) fulfilled DAPSA remission, 113 (45.7%) were in cDAPSA remission, 56 (22.5%) met VLDA and 37 (19.5%) were in PASDAS near remission. The DAPSA could not be calculated in 4/250 patients due to missing CRP values; 1/250 patients had incomplete data to calculate the VLDA (missing PASI score), the PASDAS score could not be calculated in 23/250 patients due to missing SF36 scores and the majority of these patients did not fulfil any of the remission targets (18/23). There was a very high agreement between DAPSA and cDAPSA remission (kappa 0.959) reflecting the similarity of the two definitions (the inclusion of CRP is different). The agreement between both DAPSA/cDAPSA and VLDA was moderate (kappa of 0.516 and 0.544, respectively). The agreement between VLDA/cDAPSA/DAPSA and PASDAS is considered fair, with a kappa of 0.403, 0.321, 0.319, respectively (table 1A).
Kappa scores
The concordance in fulfilment of the criteria is presented in figure 1. VLDA and PASDAS are the most stringent, and the DAPSA scores the least. All patients who met VLDA were in DAPSA/cDAPSA remission. Of those patients in DAPSA remission but not in VLDA, 43/56 patients did not fulfil 1/7 domains, while nine did not fulfil 2/7 domains. Domains not fulfilled were skin (n=33), tender joints (n=7), swollen joints (n=1), enthesitis (n=3), VAS scores (n=6) or HAQ (n=9). In the nine patients who did not achieve VLDA due to a high HAQ score, eight of them met the MDA criteria suggesting that they would have fulfilled an alternative LDA target. In 4/9, the HAQ domain was the only criteria that was not met; in 5/9, there were other residual domains (PASI n=2, enthesitis score n=2 and VASglobal n=2).

Venn diagram representing the number of patients meeting different remission criteria. The graph only includes those patients where all criteria were available (n=226). cDAPSA, clinical DAPSA; DAPSA, Disease Activity Index for Psoriatic Arthritis; PASDAS, Psoriatic Arthritis Disease Activity Score; VLDA, very low disease activity.
Residual disease activity in patients fulfilling the remission/inactive disease measures
Levels of residual disease activity in patients meeting the different measures for remission/inactive disease are shown in table 2 and figure 2.

The remaining residual disease activity in different disease domains within the subgroups of patients meeting the different remission criteria. The graphs show residual disease on different disease activity measures (top to bottom: swollen joints, tender joints, enthesitis, skin and CRP) in the patient groups fulfilling the different remission measure (left graphs) or LDA measure (right graphs). Stacked bars divide the patients fulfilling each remission/LDA measure in groups according to the amount of residual disease present. cDAPSA, clinical DAPSA; CRP, C reactive protein; DAPSA, Disease Activity Index for Psoriatic Arthritis; LDA, low disease activity; MDA, minimal disease activity; PASDAS, Psoriatic Arthritis Disease Activity Score; VLDA, very low disease activity.
Residual disease activity in different measures for remission
These measures do not represent similar numbers of residual disease in all domains. The presence of swollen joints and active enthesitis was similar across the different measures (SJC ≥1 in 5%–10% of patients and enthesitis ≥1 in 4%–0% of patients). TJCs were lower in VLDA (TJC ≥1 in 9%) and higher in the DAPSA, cDAPSA and PASDAS remission groups (TJC ≥1 in 17%, 18% and 25%, respectively). Skin disease was more prevalent in both DAPSA measures (a PASI ≥1 in resp. 30% of cDAPSA and 31% of patients with patients) in contrast with 14% in the PASDAS patients and 0% in VLDA. cDAPSA and VLDA had similar proportions of patients with raised CRP (10% and 9%) in comparison with DAPSA and PASDAS (8%), although CRP is not assessed in either cDAPSA or VLDA definitions.
VLDA presents as a more stringent cut-off with the least residual disease in PASI and tender joint count. PASDAS seems to include more patients with tender joints but less with an elevated CRP and less patients with active skin disease in comparison with the other measures. Both DAPSA scores considered more patients in remission but did allow for more residual disease activity in the domains tender joints, skin disease and enthesitis in comparison with the other measures.
Residual disease activity in remission measures related to quality of life (QoL)
In those patients with a raised CRP, no differences were found on patient reported outcomes (PROs) on QoL and functionality. Very few patients had residual enthesitis in any definition and those in remission with an enthesitis did not report significantly worse functioning or QoL, although some of the BASDAI scores were higher. Residual skin disease did affect DLQI, although not to a very high extent. For patients with ‘active’ skin disease (with PASI scores ≥1), no effect is seen on all quality-adjusted life year measures and the 74/110 patients fulfilling DAPSA with a PASI of ≥1 do not present with a higher score on the DLQI scale. The group with a PASI of >2 (present in 20/110 pts achieving DAPSA remission) was reflected by an impact on DLQI (2.85 (SD 2.9) vs 1 (2.3) p=0.003). No conclusions can be drawn on the effects of residual dactylitis as this cohort presented with a very low amount of patients with an active dactylitis during the trial visit.
Low disease activity and inactive disease measures
Comparisons of the low disease activity/inactive disease measures
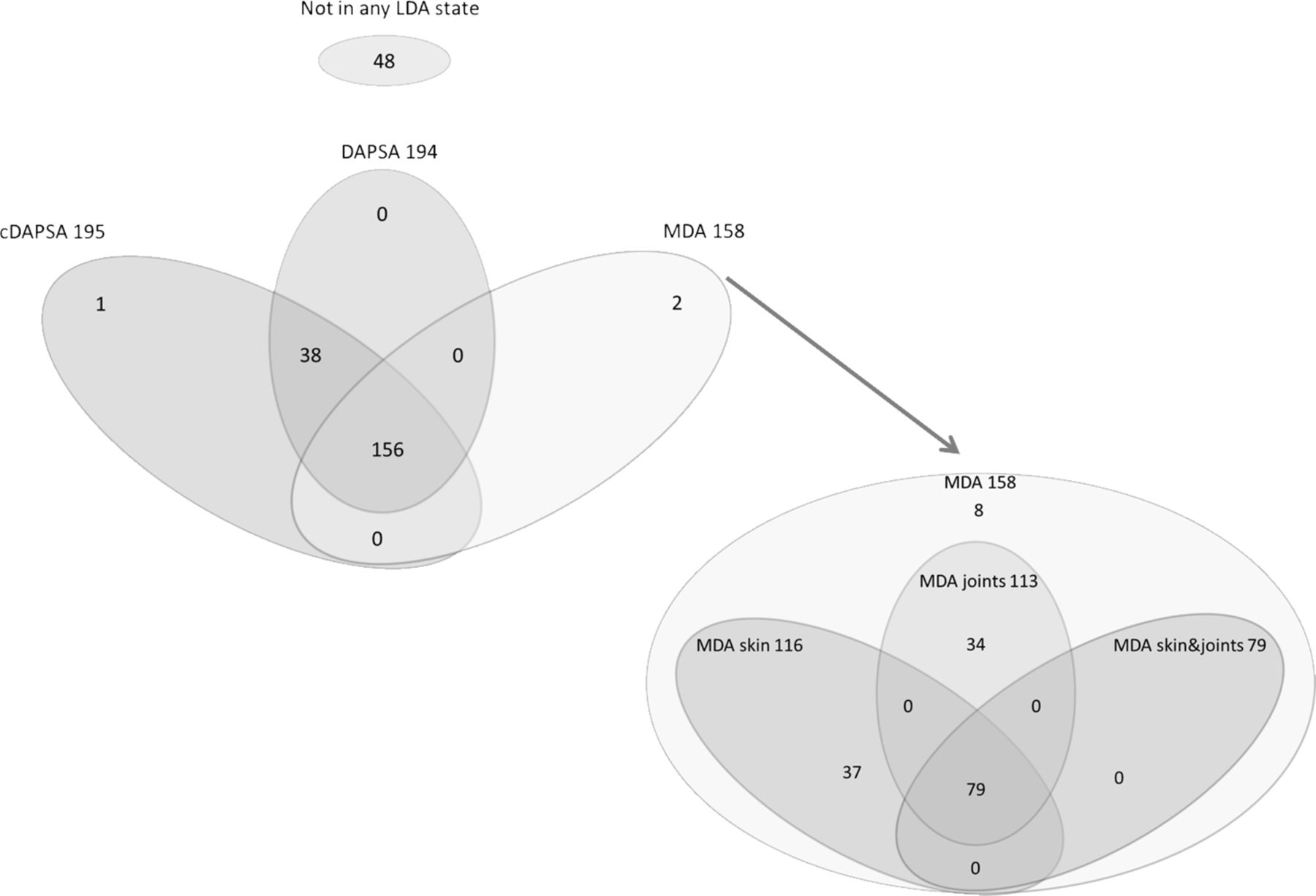
Of the total population, 162 (65%) achieved MDA, 113 (45.6%) achieved MDAjoints, 114 (46%) achieved MDAskin, 79 (31.6%) achieved MDAjoints&skin, 195 (78%) achieved DAPSA LDA, 195 (78%) achieved cDAPSA LDA.
The concordance in fulfilment of the criteria is presented in figure 3.
{kind=link}
{kind=link}
{kind=link}
Venn diagram representing the number of patients meeting different low disease activity criteria. The graphs only include those patients where all criteria were available (n=245). cDAPSA, clinical DAPSA; DAPSA, Disease Activity Index for Psoriatic Arthritis; LDA, low disease activity; MDA, minimal disease activity.
A high agreement is seen between the DAPSA/cDAPSA and the MDA5/7 (kappa of 0596 and 0611, respectively) table 1B. Agreement between the DAPSA and the alternative MDA measures (MDAjoints, MDAskin and MDAjoints&skin) is lower as these targets are more stringent.
Residual disease activity in patients fulfilling low disease activity/inactive disease measures
Levels of residual disease activity in patients meeting low disease activity/MDA/new MDA measures are shown in table 3 and figure 3.
Residual disease activity in different measures for low disease activity
Higher levels of tender and swollen joint counts and skin disease are seen in the DAPSA LDA measures in comparison with all four MDA scores. By their definition, MDAjoints and MDAjoints&skin show an even stricter cut-off on joint involvement, with a single swollen joint in only 10% and 5%, respectively, and a tender joint in only 14% and 2% of the patients.
Between the different outcome measures, the presence of patients with a raised CRP is similar (approximately 12% in all measures).
Residual disease activity in remission measures related to QoL
Not including an enthesitis measure in the score does not seem to make much difference; it does not result in a group of patients with active disease and a high disease burden, as only five patients with an active enthesitis fulfil (DAPSA) LDA criteria, these patients did not differ in QoL scores in comparison with other DAPSA LDA patients. No differences were found on PROs on QoL and functionality between patients with and without a raised CRP. A PASI score >1 was more prevalent in the DAPSA cut-off groups in comparison with the MDA/new MDA measures (46% in DAPSA LDA n and between 0% and29% in the different MDA measures). The patients with active psoriasis in the DAPSA LDA group did report significantly larger impact of skin disease on dermatology related QoL (DLQI scale) (PASI 0–1: 1 to 25 (SD2,4) vs PASI >1: 1.55 (SD2.7), p=0024.
Discussion
The analysis of different remission and low disease activity targets in this real life clinical cohort do show significant overlap between the measures. However, it is clear that these different measures targeting the same conceptual definition (ie, remission or low disease activity) do result in different levels of residual disease present in individuals. Comparison of the several candidate measures demonstrates that VLDA is achieved by the lowest proportion of patients in this cohort. This suggests that it may be the most stringent target for remission of inactive disease, although it could be difficult to attain and may be more stringent than patient and physician opinion of acceptable disease states. The modified MDA measures are the most stringent targets for low disease activity in terms of residual disease on joints, psoriasis and enthesitis within patients achieving the target. In both remission and LDA measures the addition of CRP did not show an added value. The exclusion of a domain for psoriasis, as in the DAPSA measures, resulted in negligence of skin disease and a negative impact on the QoL in some patients.
For this study, we used three different measure concepts validated for psoriatic arthritis, the MDA and the adjusted versions (MDAskin/MDAjoints and MDAjoints&skin as well as VLDA), DAPSA and PASDAS. The MDA and adjusted MDA measures all use a modular approach where an individual cut-off for each domain is specified and depending on the measure used, a number of cut-offs need to be met. In contrast, the DAPSA and PASDAS measures sum the scores of the individual components into one final number. In both the DAPSA and PASDAS measures for remission and low disease activity, higher levels of residual musculoskeletal disease were seen in comparison with the VLDA and the MDAskin/joint measures. An active domain can be hidden when other domains are relatively unaffected, resulting in the inclusion of patients with active disease within the group of patients seen as in remission or low disease activity state.
The DAPSA focuses specifically on peripheral joint disease, and some argue that this is ideal as it can reflect change accurately in this single domain. However, because it does not measure other domains of the disease, active disease in these domains is missed. Residual skin disease was highest in patients achieving DAPSA or cDAPSA remission when compared with the other remission targets as well as for the DAPSA and cDAPSA low disease cut-offs in comparison with the adjusted MDA measures. Within our group of patients, this resulted in a group of patients, seen as in a low disease activity state, with remaining skin disease impacting their QoL. This analysis highlights the need for multiple separate measures for different domains to be assessed if a multidimensional definition is not used to ensure that remission retains face validity for the patients.
The MDA domains include a measure of function as they were taken from the core domain of PsA and are in line with similar definitions in RA.12 13 Concern has been raised that, as the HAQ will be affected by non-reversible damage as well as disease activity, this may limit their applicability.14 In this cohort with established disease (mean disease duration of 12.7 years), very few patients failed to achieve VLDA due to HAQ alone, but they did achieve MDA and its more stringent variations. Another concern that has been raised is the influence of comorbid fibromyalgia on the outcome measures and potential targets. Brikman et al have shown that fibromyalgia impacts on both DAPSA, MDA and other scores. Unfortunately, we do not have fibromyalgia data on these patients but given that the items within the targets overlap significantly, we do not anticipate a differential effect of fibromyalgia between the different measures.15
Not all measures used in this comparison included an inflammatory marker. The DAPSA and PASDAS include a CRP, and cDAPSA and MDA measures do not. These data suggest that the inclusion of CRP is unnecessary to include as a similar proportion of patients have a raised CRP in all definitions. Those patients with a raised CRP that fulfilled the disease targets did not show a difference in other disease activity measures or on PRO scores. A target without an inflammatory marker will be more practical in clinical practice and if routine laboratory assessment is not needed for other reasons a lower burden for the patient as well.
Another important factor worth considering when choosing a tool for clinical practice is the feasibility and practicality of the tool. The tool should ideally be easy to calculate, as limited time during daily practice makes a simple to obtain target easier to incorporate in clinical practice. Second, when many different outcomes need to be assessed, it will be laborious to calculate these individual scores and the chance increases that information is missing. Third, the transparency and presentation of the tool after calculation is of importance as the individual components will still remain important to consider when targeting a therapy.
Several considerations can be made to the assessed measures in this study, all having their own strengths and weaknesses: the DAPSA focuses only on peripheral joint disease and does not include a skin or enthesitis component; the PASDAS is less transparent on individual components, and the complexity makes it more time consuming to calculate this measure; the MDA is a binary measure (and not a continuous one), therefore scores do not show an increase in disease activity after the bar for remission or LDA is achieved.
It is important to note that we made no attempt to perform new psychometric analyses on measures and only restricted our work to answer the question how the available, validated measures perform and compare with one each other. With the ongoing efforts on gaining consensus on a target for the treatment of PsA, more information on the impact of residual disease is needed. The cut-off for acceptable disease activity is of importance as with a stricter target more intensive treatments might be started, might lead to a more intensive treatment, and this eventually could result in overtreatment of patients with consequences in terms of side effects and an increase in costs. The ideal stringency of a target with assessment of residual disease in the various clinical domains of PsA should be a focus of future research. An observational study shows lower levels of disease activity in remission versus LDA states and better QoL.16 It remains unknown whether meeting a strict target such as VLDA is superior in reducing impact on patient outcomes such as QoL, radiographic progression and functioning, in comparison with less stringent targets. Ideally a trial comparing remission and low disease activity, incorporating efficacy, safety, cost–benefit and patient opinion is needed.
References
Footnotes
Handling editor Tore K Kvien
Contributors All authors fulfilled the ICMJE recommendations for authorship, were involved in drafting and reviewing of the manuscript and approved the final version.
Funding The original cohort was supported by an unrestricted grant from Pfizer B.V.
Competing interests LJJvM, none declared. MGHvdS has received speakers/consultancy fees from Takeda, Tillotts and Benecke MSD. DB has received research grants and speakers/consultancy fees from Pfizer, MSD, AbbVie, UCB, Novartis, Janssen, Boehringer Ingelheim; speakers/consultancy fees from Eli Lilly, Roche, BMS and Glenmark; and is currently an employee of UCB. AWRvK has received speakers/consultancy fees from Celgene, Janssen-Cilag, Novartis, MSD and Roche. LCC, none declared.
Patient consent Obtained.
Ethics approval METC AMC Amsterdam.
Provenance and peer review Not commissioned; externally peer reviewed.