Article Text

Abstract
Objectives To investigate the ability of whole-body MRI (WBMRI) to detect axial and peripheral enthesitis in patients with psoriatic arthritis (PsA) and axial spondyloarthritis (axSpA), and in healthy subjects (HS). Furthermore, to develop MRI enthesitis indices based on WBMRI and validate these by use of clinical measures of disease activity.
Methods Prospective cross-sectional study of patients with PsA (n=18) and axSpA (n=18) with moderate to high disease activity, and HS (n=12). Enthesitis at 35 individual sites located at upper and lower limbs, chest and pelvis were evaluated by WBMRI and clinical examination, and compared. Three new WBMRI enthesitis indices were developed.
Results WBMRI allowed evaluation of 888 (53%) of 1680 sites investigated, and 19 (54%) of 35 entheses had a readability >70%. The percentage agreement between WBMRI and clinical enthesitis was 49–100%, when compared at the level of the individual entheses. Enthesitis on WBMRI was observed in 148 (17%) of the entheseal sites, and was frequently present at greater trochanters (55%) and Achilles (43%) and supraspinate (23%) tendon insertions in patients and HS. At the first mentioned two locations enthesitis often appeared without clinical signs of enthesitis. Patients and HS differed significantly in one of the new WBMRI enthesitis scores. Patients and HS differed significantly in one of the new WBMRI enthesitis scores, and this score correlated weakly with BASDAI question 4 (tenderness in relation to entheses), BASDAI and patient global (ρ=0.29–0.31, p<0.05).
Conclusions WBMRI is a promising new imaging modality for evaluation of enthesitis in patients with PsA and axSpA, but requires further investigation before clinical use.
Statistics from Altmetric.com
Introduction
Psoriatic arthritis (PsA) and axial spondyloarthritis (axSpA) are inflammatory arthritides, in which the presence of heel enthesitis often is a prominent clinical feature.1–3 Nevertheless, clinical enthesitis is also frequently present at other anatomical locations.4–13 Currently, the diagnosis of enthesitis is primarily based on clinical examination of tenderness, and more objective methods demonstrating inflammation at tendons, ligaments and fascia at their insertion in bone and/or the adjacent soft tissue are needed. MRI is a promising method for improving enthesitis assessment, by its ability to visualise extraosseous and intraosseous inflammations.14 ,15 In contrast to conventional MRI, which only covers one anatomical area in one scan, whole-body MRI (WBMRI) is a new imaging modality that allows assessment of all peripheral and axial joints and entheses from ‘head-to-toe’ in one examination.16 ,17 Only four prospective studies have investigated the ability of ‘head-to-toe’ WBMRI to evaluate the presence of enthesitis in patients with PsA18 and axSpA.19–21 However, none of these studies have directly and systematically compared WBMRI findings of enthesitis at the individual entheseal sites with clinical examination in patients with PsA or axSpA or included a control group. Furthermore, no WBMRI indices have previously been developed.
The aim of this pilot study was systematically to investigate the ability of ‘head-to-toe’ WBMRI to detect axial and peripheral enthesitis in patients with PsA, axSpA and in healthy subjects (HS), and to compare with clinical examination of the same anatomical areas. Furthermore, to develop MRI enthesitis indices based on WBMRI, and to validate these by use of clinical measures of disease activity.
Methods
Patients
Inclusion and exclusion criteria
Patients were eligible for this prospective study if they had either PsA according to Moll and Wright's criteria22 or spondyloarthritis according to the European Spondylarthropathy Study Group criteria.3 Patients with PsA were included if they had active disease defined as ≥ three tender and/or swollen joints and ≥ one swollen finger joint and/or dactylitic finger. Patients with spondyloarthritis were included if they had a Bath Ankylosing Spondylitis Disease Activity Index (BASDAI)23 ,24 score of ≥30 mm and active spinal disease according to the rheumatologist. Treatment with glucocorticoids or initiation of tumour necrosis factor α inhibitor was not allowed within 4 weeks before study investigations. HS could not be included, if they had pain from peripheral joints or spine, a family history of PsA, spondyloarthritis or rheumatoid arthritis, or a medical history of psoriasis, anterior uveitis, inflammatory bowel disease or heel pain.
Clinical examinations
Clinical enthesitis was defined as tenderness, when the enthesis was palpated with a pressure of the thumb until the tip of the nail bed blanched.12 One of two experienced clinicians examined each of the study participants at 18 peripheral and axial entheses at 35 different locations (figure 1): the medial and lateral humeral epicondyles, supraspinate tendon insertion into the greater tuberosity of humerus, 1st and 7th costochondral joints, iliac crest, anterior superior iliac spine, posterior superior iliac spine, 5th lumbar spinous process (L5), ischial tuberosity, greater femoral trochanter, medial and lateral femoral condyles, quadriceps tendon insertion into patella, patellar ligament insertion into patella and tibia, Achilles tendon insertion and plantar fascia at the insertion into calcaneus. These entheses have been included in clinical enthesitis indices such as the Berlin,7 ,8 Major,8 ,9 Gladman,10 Leeds,9 Maastricht Ankylosing Spondylitis Enthesitis Score,11 SPondyloArthritis Research Consortium of Canada12 and Infliximab in PsA Clinical Trial13 indices (figure 1). Furthermore, 78 tender and 76 swollen joint counts were performed.25 All study participants filled in BASDAI, pain and patient global visual analogue scale. Serum C reactive protein was measured, and the Ankylosing Spondylitis Disease Activity Score26 calculated.
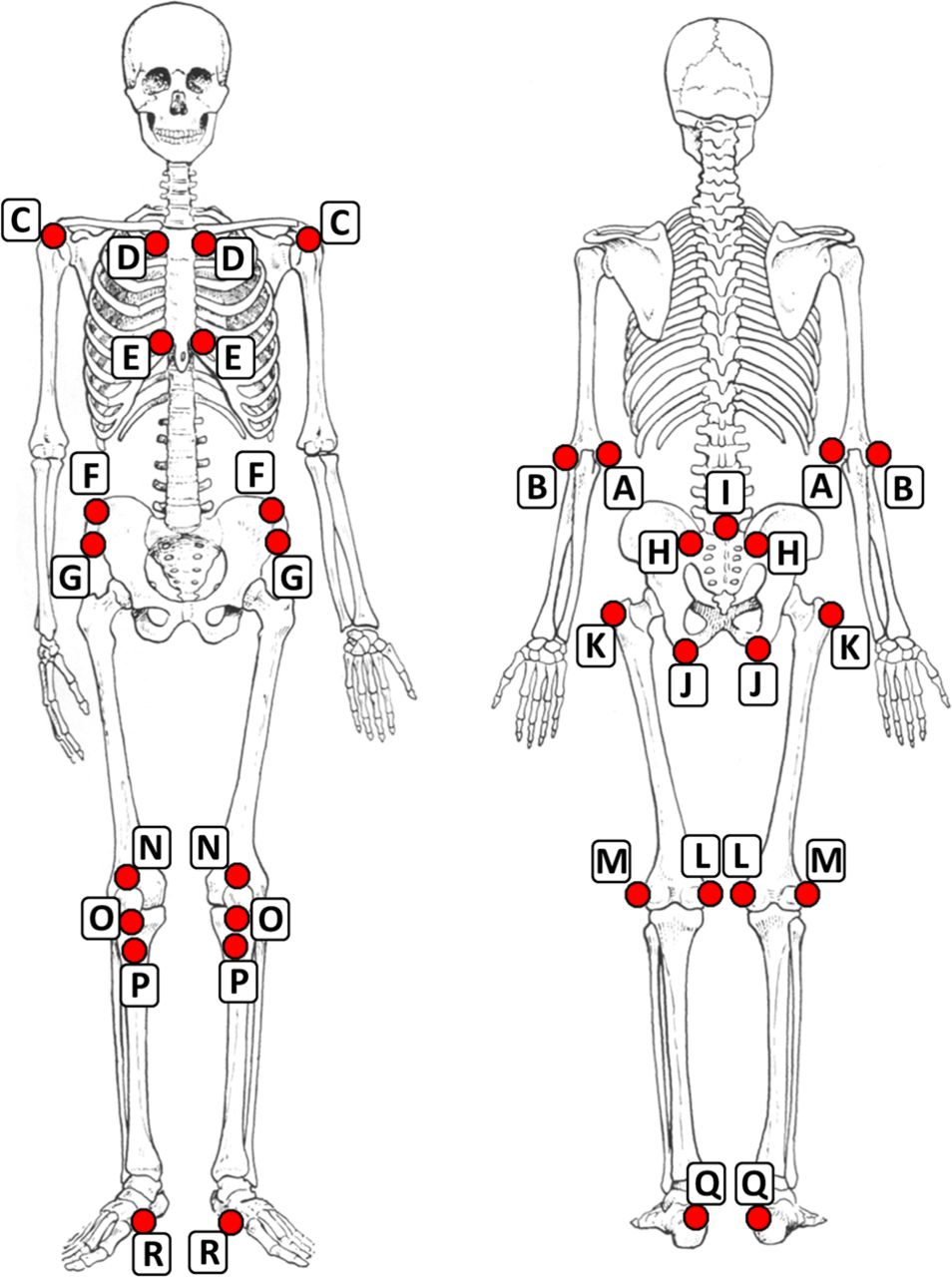
The 35 entheseal sites assessed by WBMRI and clinical examination. The entheseal sites examined on the upper limbs: (A) the medial and (B) lateral humeral epicondyle and (C) supraspinate tendon insertion into humerus; at the chest: (D) the 1st and (E) 7th costochondral joint; at the pelvis: (F) the iliac crest, (G) anterior superior iliac spine, H) posterior superior iliac spine, (I) 5th lumbar spinous process and (J) ischial tuberosity; and at the lower limbs: (K) the greater femoral trochanter, (L) medial and (M) lateral femoral condyle, (N) quadriceps tendons insertion into patella, O) the patella ligaments insertion into patella and into (P) tibia, (Q) Achilles tendon insertion and (R) plantar fascia. The enthesitis indices investigated in this study comprised the following entheses: WBMRI Index 1: C, F-H and J-L; WBMRI Index 2: C, J, K, Q and R; WBMRI Index 3: C, H and Q. The clinical indices Berlin7 ,8: F, H, K, L, Q and R; Major index8 ,9: A, B, F, K, Q and R; Gladman index10: C, P-R; Leeds index9: B, L and Q; MASES index11: D-I and Q; SPARCC index12: A-C, K, N-R; and IMPACT index13: Q and R. Abbreviations: IMPACT, Infliximab in PsA Clinical Trial; MASES, Maastricht Ankylosing Spondylitis Enthesitis Score; WBMRI, whole-body MRI; and SPARCC: SPondyloArthritis Research Consortium of Canada. The illustration of the skeleton was made by Erik Lenders and is from “Finn Bojsen-Møller. Bevægeapperatets Anatomi”, Munksgaard Denmark 1996 (with permission from Munksgaard Denmark).
MRI
Technical aspects of MRI
WBMRIs were performed on a 3 tesla MRI unit using the built-in Q-Body coil (Philips Achieva). MRI scans were performed in six stations with coronal slice orientation for the spine, hip, knee and ankle, sagittal orientation for the neck and axial orientation for the feet. The scan included T1-weighted sequences acquired before and after administration of intravenous contrast agent (gadoteric acid, Dotarem, Guerbet, 0.5 mmol/mL, 0.2 mL/kg body weight) and short τ inversion recovery sequences acquired before contrast injection. The technical MRI parameters are shown in table 1. Total scan time was 61 min and was well tolerated by the study participants.
Technical parameters of the WBMRI scan
Evaluation of MRI
WBMRIs were assessed by a musculoskeletal radiologist (IE) experienced with WBMRI.14 The radiologist was blinded to all clinical and biochemical information. The images were evaluated in random order. Readability of the scans was assessed for each enthesis as ‘readable’, ‘not readable’ (eg, due to artefacts) or ‘not in field of view (FOV)’ (ie, not scanned). Enthesitis was defined as suggested by Eshed et al,14 as presence of bone marrow oedema, soft tissue oedema, change in tendon thickness, erosions or enthesophytes in adjacent bones, and additional findings such as fluid around tendons or adjacent to bursa, alone or in combination. The decision was based on all available sequences, and it also included a comparison with the opposite site for paired entheses. All entheses were scored dichotomously (present/absent). WBMRI scans with examples of enthesitis are shown in figure 2.

{kind=link}
{kind=link}
(A)–(C) Images from whole-body MRI (WBMRI) of the right shoulder of a 34-year-old male patient with ankylosing spondylitis with disease duration of 7 years. The T1-weighted fat-saturated (FS) sequence performed after intravenous contrast injection (B) shows bone marrow oedema at the insertion of the supraspinate tendon at the humeral head and synovitis at the acromioclavicular joint. Clinically, the patient had no supraspinate enthesitis, and no swelling or tenderness of the shoulder or at the acromioclavicular joint. (D)–(F) Images of WBMRI of the left hip of a 52-year-old healthy woman. The short τ inversion recovery (STIR) sequence (E) shows thickening and high signal intensity of the medial gluteal tendon at its insertion on the greater femoral trochanter compatible with medial gluteal enthesitis. There is also a small amount of fluid in the adjacent trochanteric bursa and minimal bone marrow oedema of the trochanter itself. In the hip joint, there is a small amount of effusion which is within the normal limits. Clinically, the subject was tender when examined at the greater trochanter enthesis, but without tenderness at the hip joint. (G)–(I) Images of WBMRI of the left hip in a 57-year-old male patient with psoriatic arthritis (PsA). The STIR sequence (H) shows thickening and high signal intensity of the hamstring tendon at its insertion on the ischial tuberosity. Slight bone marrow oedema is also noted in the ischial tuberosity. Clinically, the patient was tender at the left hip joint, but not at the ischial tuberosity. (J)–(L) Images of WBMRI of the right ankle of a 48-year-old female patient with PsA. The STIR sequence (K) shows high signal intensity of the Achilles tendon and in the soft tissue in the hind foot, both compatible with Achilles enthesitis. A small subchondral cyst is also seen in the distal tibia. Clinically, the patient was tender at the Achilles tendon insertion and had swelling and tenderness of the ankle joint. (A), (D), (G) and (J) are T1-weighted sequences. (B) is T1-weighted with FS after gadolinium injection. (E), (H) and (K) are STIR sequences, (C), (F), (I) and (L) are cartoons on the same images illustrating the inflammatory findings in white.
Construction of new MRI enthesitis indices
After image assessment, three data-driven WBMRI enthesitis indices were constructed. They were based on the following definitions: (1) entheseal sites with high readability on MRI defined as ≥90% for all study participants; (2) entheses often involved in PsA and axSpA, that is, supraspinate tendon insertion, ischial tuberosity, greater femoral trochanter, Achilles tendon insertion and plantar fascia; (3) selected entheseal sites, where patients and HS differed in the frequency of enthesitis on WBMRI: supraspinate tendon insertion, posterior superior iliac spine and Achilles tendon insertion. WBMRI enthesitis indices scores were also calculated based on the previously developed seven clinical enthesitis indices (figure 1).7–13
Statistics
Data were described by use of median, IQR and percentage. Percentage agreement was calculated as the sum of the corresponding positive and negative findings on MRI and clinical examination, divided by the number of readable entheses. Comparisons between groups were performed with Fisher’s exact test and Mann-Whitney test. Spearman's rank correlation coefficient ρ was used for assessment of correlations. Reliability analysis included calculation of absolute agreement and intrareader correlation coefficients (ICCs) after rescoring of 10 WBMRIs using sum scores of entheses readable at both reads. Rescoring was done 1 year after the primary read. The ICC was calculated by use of a two-way mixed model, and the results are provided as absolute agreement for single measures. The statistical analyses were performed in SAS V.9 (SAS, Cary, North Carolina, USA), except for ICC which were performed in SPSS V.19 (SPSS, Chicago, Illinois, USA). A p value <0.05 was considered statistically significant.
The study was performed in accordance with the Declaration of Helsinki27 and approved by the local ethical committee. A written informed consent was obtained from all study participants before inclusion into the study.
Results
Clinical characteristics of study participants
Eighteen patients with PsA and axSpA, respectively, and 12 HS were included in the study. Baseline characteristics of the study participants are shown in table 2. Compared with HS, patients with PsA and axSpA had higher disease activity, including swollen and tender joint counts.
Baseline characteristics
Readability of entheses on WBMRI
The readability of WBMRI for evaluation of individual entheses is shown in table 3. WBMRI allowed evaluation of 888 (53%) of 1680 sites investigated, and 19 (54%) of 35 entheses had a readability >70%. All pelvic entheses, supraspinate tendon, greater femoral trochanter and medial femoral condyle could be assessed in ≥94% of the study participants. The Achilles tendon could be evaluated in 71%, but were not in FOV in 21% and were scanned, but impossible to evaluate in 8% of the study participants. In contrast, readability was low for the anterior chest wall and elbows, as they were only in FOV in 29% and 1%, respectively. Furthermore, readability was compromised at the patellar ligament insertion into patella (readable in 5%) and tibia (2%). The plantar fascia and lateral femoral condyle could not be visualised by WBMRI, because sagittal slices were not available. Consequently, these entheses were only evaluated clinically.
Readability of 35 entheses when assessed on WBMRI and presence of enthesitis on WBMRI and clinical examination, shown for all study participants
Enthesitis at the individual entheseal site on WBMRI and at clinical examination
The frequency of WBMRI and clinical enthesitis for the individual entheses are also shown in table 3. WBMRI enthesitis was observed in a total of 148 of 888 (17%) entheseal sites, whereas clinical enthesitis was present at 193 (22%) of the corresponding entheseal sites (ie, based on readable MRIs only). The three entheseal sites most frequently observed with MRI enthesitis were the greater trochanter (52 entheses (55% of the readable entheses)), Achilles (30 (43%)) and supraspinate (21 (23%)) tendons. Tenderness was most often recorded at the 1st and 7th costochondral joints, greater femoral trochanters and supraspinate tendons (30–33 (31–35%)).
The frequency of enthesitis at the individual entheseal sites in patients with PsA, axSpA and HS is shown in table 4. Patients with PsA had 57 (18% (95% CI 14% to 22%)) and 95 (29% (25% to 35%)) corresponding entheseal sites with enthesitis on WBMRI and clinical examination, whereas patients with axSpA had 57 (18% (14% to 22%)) and 75 (23% (19% to 28%)) sites, and HS had 33 (14% (10% to 20%)) and 18 (8% (5% to 12%)) entheseal sites with enthesitis on WBMRI and clinical examination, respectively. The entheseal sites most frequently observed with enthesitis in the three subgroups were the same as for the whole study population (tables 3 and 4).
The presence of enthesitis on WBMRI and clinical examination in patients with PsA, axSpA and healthy subjects (entheses with low readability (<25%) are not shown)
The percentage agreement between WBMRI and clinical enthesitis was 68–100% for all entheseal sites, except for the medial femoral condyle (64%), Achilles tendon (52%) and greater trochanter (49%). All κ values were <40% or could not be calculated due to no positive findings (‘zero-only’ values) on MRI.
WBMRI enthesitis indices
Patients and HS did not differ significantly in WBMRI scores when based on assessment of all 35 entheseal sites (median 3.5 (IQR 1–4) vs 2.5 (1.5–3.5), p=0.49), WBMRI Index 1 (2 (1–4) vs 2 (1–2.5), p=0.62), and Index 2 (2.5 (1–4) vs 2 (1–2.5), p=0.33), whereas the patients had higher scores when assessed by WBMRI Index 3 (1 (0–2) vs 0 (0–0), p=0.047). There were no differences between patients and HS when assessed with the previously developed clinical enthesitis indices when MRI data was applied (data not shown). The association between all WBMRI enthesitis indices and disease activity (table 1) were assessed systematically for all indices including all study participants (results not shown). Significant correlations were observed between MRI Index 3 and BASDAI question 4 (tenderness in relation to entheses) (r=0.31, p=0.04), BASDAI (r=0.30, p=0.04) and patient global (r=0.29, p=0.04).
Ten WBMRIs were reanonymised and reread after 1 year. The intrareader ICC for the total number of entheses with enthesitis on WBMRI (total WBMRI score) was 0.58. The absolute agreement for positive and negative findings was 0.85.
Discussion
This prospective, cross-sectional pilot study showed that enthesitis can be detected on WBMRI with moderate agreement between WBMRI and clinical examination. On WBMRI, enthesitis is frequently observed in patients with PsA, axSpA as well as in HS, and most frequently occurs at the greater femoral trochanter, supraspinate and Achilles tendon insertions. Although the MRI enthesitis scores were higher in the patients, the entheseal sites with WBMRI enthesitis were the same in patients and HS, except for the posterior superior iliac spine which was observed in patients only. Three WBMRI enthesitis indices were developed, of which one may be of clinical value for assessing disease activity and for differentiating patients from HS.
Only few studies have investigated WBMRI enthesitis systematically by use of ‘head-to-toe’ WBMRI in prospective studies of patients with PsA18 and/or axSpA.19 ,20 Comparable with our results, Weckbach et al18 observed MRI enthesitis in 68% of the hip regions of 30 patients with PsA, but did not observe MRI enthesitis at the shoulder. In contrast, Althoff et al20 in the ESTHER trial demonstrated low frequencies of MRI enthesitis at greater trochanter and Achilles tendons (both 2 lesions in 75 patients), ischial tuberosity (5 lesions), plantar fascia (3 lesions) and supraspinate insertion (0 lesions), whereas MRI enthesitis most frequently was seen in other pelvic areas (14 lesions) and in particular at the sacrococcygeal entheses (11 lesions), which we did not investigate. However, they did not report findings for the posterior superior iliac spine, where we observed MRI enthesitis in 15% of patients with axSpA and 17% of patients with PsA. The ESTHER trial included patients with axSpA with a symptom duration of <5 years initiating tumour necrosis factor α inhibitor therapy. The observed differences may be related to longer symptom duration and the wider MRI definition of enthesitis used in our study, since patients in both groups had moderate to high disease activity. In addition, little is known about other pelvic structures involved in axSpA, and inflammation may hypothetically be more prominent at ligaments adjacent to the sacroiliac joints in the very early disease stage, while it may be located more peripherally at later stages.
Patients with PsA had a higher frequency of clinical enthesitis than patients with axSpA, whereas they did not differ in frequency of enthesitis on WBMRI. The clinical results are in concordance with other studies,28 ,29 while no other MRI data are available. Furthermore, patients had more enthesitis at clinical examination than on WBMRI, whereas it was the opposite for HS. Moreover, enthesitis was more frequent on WBMRI than by clinical examination at greater trochanter, Achilles tendons and ischial tuberosity, which also frequently were observed with WBMRI enthesitis in the HS. This may be explained by the presence of subclinical enthesitis, which may be related to other conditions inducing mechanical stress such as high body mass index or physical overuse. Several HS were frequent runners, and this may explain the general high frequency of enthesitis in the lower limbs and the difference in the frequency of clinical and MRI enthesitis. Studies based on conventional MRI have also demonstrated enthesitis at the shoulders30 and Achilles31 tendons in asymptomatic patients with axSpA and HS. Future studies of enthesitis should therefore also take other factors such as weight and physical activity into account, which may be associated with enthesitis.
The WBMRI enthesitis index that best discriminated patients from HS were those based on a combination of clinically relevant entheses for patients with PsA and axSpA, whereas indices based on readability and entheses often involved in PsA and SpA were less discriminatory. Furthermore, the proposed WBMRI Index 3 was associated with clinical measures of disease activity. To our knowledge no other WBMRI enthesitis indices have been developed. The discriminative capacity and responsiveness should be investigated in future studies.
This study also showed it is possible to detect enthesitis by ‘head-to-toe’ WBMRI with moderate percentage agreement between MRI and clinical findings at the entheseal level. Only Weber et al32 have investigated the association between clinical and WBMRI findings for individual entheses but only for the anterior chest wall, and they found no association. Similarly, Song et al21 found no significant correlations between an MRI enthesitis score and clinical parameters of disease activity. Weckbach et al18 reported MRI enthesitis at more locations than at clinical examination in 80% of patients with PsA. They assessed clinical enthesitis with the Maastricht Ankylosing Spondylitis Enthesitis Score index,11 which comprises the 1st and 7th costochondral joints, Achilles tendon and the pelvic entheses included in the present study except for ischial tuberosity. Consequently, their WBMRI protocol covered more entheses than assessed clinically, whereas we assessed the same anatomical areas on WBMRI and clinical examination.
It should be emphasised that, although we consider clinical examination to be the gold standard, previous studies only have documented a moderate reliability of clinical assessment (ICC range 0.40–0.80) among rheumatologists with expertise in spondyloarthritis,7 and this undoubtedly contributes to the lack of association with MRI findings. Furthermore, the rheumatologists in the present study were not blinded for diagnosis and clinical data, whereas the radiologist was blinded for all information. The moderate ICC (0.58) for 1 year reproducibility was partially caused by the variable readability of the MRI scans, and by the small sample size for the reproducibility study.
The readability of the MRIs varied substantially, from very high for entheses at pelvis, shoulder and hip to very low for entheses at elbow, knee and foot. Weckbach et al18 reported good quality at centrally located joints and lower quality at distal peripheral joints. In ‘head-to-toe’ WBMRI the slices are usually thicker (5–6 mm) than on conventional MRI, which makes the images less suitable for assessment of some entheses for example, at the costochondral joints. Furthermore, only one scan plane is used, which not always is the optimal plane for the individual entheses. This was in particular a problem for the costochondral joints, patellar ligaments and plantar fascia. Moreover, image quality is lower if the area scanned is located in the periphery of the scanner (off-centre artefact), for example, elbows. Furthermore, the movement of thorax through the respiratory cycle leads to motion artefacts, which is a major problem for assessment of small joints at the anterior chest wall. Finally, the supine position in the scanner facilitates external rotation of the legs and feet, resulting in an oblique sagittal scan plane that make evaluation of the plantar fascia difficult. All these technical issues can be improved in future studies by optimising patient positioning, adding sagittal slices to the knee scan, and use of external coils besides the build-in coil. All together this will increase readability substantially.
In conclusion, this study showed that WBMRI is a promising new imaging modality for investigating axial and peripheral entheses in patients with PsA and axSpA. Readability was high for entheses at shoulder, pelvis and hip, and can potentially be optimised for anterior chest wall, elbow, knee and foot. The new WBMRI enthesitis index including clinical relevant entheses performed best when compared with clinical measures of disease activity. However, introduction of WBMRI as a clinical tool should be preceded by more research including optimisation of image acquisition, before clinical implementation is considered.
Acknowledgments
The authors acknowledge the assistance of study participants, radiographers, study nurses and laboratory staff, who participated in the study. The study was conducted without any financial support. RPP has during his PhD study received grants from The Danish Rheumatism Association, the Scandinavian Journal of Rheumatology and The Danish Psoriasis Research Foundation, and was furthermore supported by The Capital Region of Denmark. SJP's PhD study was funded by the University of Copenhagen, Denmark.
References
Footnotes
Handling editor Tore K Kvien
-
Contributors All authors were involved in drafting the article or revising it critically for important intellectual content, and all authors approved the final version to be published. RPP had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study conception and design: SJP, MØ, RPP. Acquisition of data: RPP, IE, MØ, IJS, JMM, ORM, SJP. Analysis and interpretation of data: RPP, IE, MØ, IJS, JMM, ORM, SJP.
-
Competing interest None.
-
Ethics approval This study was conducted with the approval of the Ethical Committee of The Capital Region of Denmark and the Danish Data Protection Agency.
-
Provenance and peer review Not commissioned; externally peer reviewed.