Article Text

Abstract
Background: Chronic low back pain (LBP), the leading symptom of ankylosing spondylitis (AS) and undifferentiated axial spondyloarthritis (SpA), precedes the development of radiographic sacroiliitis, sometimes by many years.
Objective: To assign disease probabilities and to develop an algorithm to help in the early diagnosis of axial SpA.
Methods: Axial SpA comprises AS and undifferentiated SpA with predominant axial involvement. Clinical features include inflammatory back pain (IBP), alternating buttock pain, enthesitis, arthritis, dactylitis, acute anterior uveitis, a positive family history, psoriasis, inflammatory bowel disease, and good response to NSAIDs. Associated laboratory findings include raised acute phase reactions, HLA-B27 association, and abnormalities on skeletal imaging. Sensitivities, specificities, and likelihood ratios (LRs) of these parameters were determined from published studies. A 5% prevalence of axial SpA among patients with chronic LBP was used. The probability of the presence of axial SpA, depending on the presence or absence of the above clinical features of SpA, was determined. A probability of ⩾90% was used to make a diagnosis of axial SpA.
Results: The presence of inflammatory back pain features increased the probability of axial SpA from the background 5% prevalence to 14%. The presence of 2–3 SpA features was necessary to increase the probability of axial SpA to 90%. The highest LRs were obtained for HLA-B27 and MRI. Diagnostic algorithms to be used in daily practice were suggested.
Conclusions: This approach can help clinicians to diagnose with a high degree of confidence axial SpA at an early stage in patients with IBP who lack radiographic sacroiliitis.
- ankylosing spondylitis
- spondyloarthropathy
- spondarthritis
- inflammatory back pain
- prediction
- early diagnosis
- AS, ankylosing spondylitis
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- ESSG, European Spondylarthropathy Study Group
- IBP, inflammatory back pain
- LBP, low back pain
- LR, likelihood ratio
- MRI, magnetic resonance imaging
- NSAIDs, non-steroidal anti-inflammatory drugs
- SpA, spondyloarthritis
- uSpA, undifferentiated spondyloarthritis
Statistics from Altmetric.com
- ankylosing spondylitis
- spondyloarthropathy
- spondarthritis
- inflammatory back pain
- prediction
- early diagnosis
- AS, ankylosing spondylitis
- CRP, C reactive protein
- ESR, erythrocyte sedimentation rate
- ESSG, European Spondylarthropathy Study Group
- IBP, inflammatory back pain
- LBP, low back pain
- LR, likelihood ratio
- MRI, magnetic resonance imaging
- NSAIDs, non-steroidal anti-inflammatory drugs
- SpA, spondyloarthritis
- uSpA, undifferentiated spondyloarthritis
Chronic low back pain (LBP) is a common problem in general practice.1 The identification of treatable causes of back pain is therefore of great clinical relevance. Ankylosing spondylitis (AS) belongs to a group of related diseases termed spondyloarthritides (SpA), which also comprise diseases such as reactive arthritis, arthritis/spondylitis with inflammatory bowel disease, and arthritis/spondylitis with psoriasis, and also undifferentiated spondyloarthritis (uSpA).2 They share many clinical manifestations and the association with HLA-B27. The SpA as a group are one of the most common rheumatic diseases with a prevalence of 0.5–1.9%, and this makes them at least as common as rheumatoid arthritis. The most common subgroups of SpA are AS and uSpA,3–5 and all of them may progress to full-blown AS. Patients with inflammatory back pain (IBP) attributable to SpA are most likely to move on to AS and may develop a chronic disabling disease. The correct diagnosis of early disease has always been a challenge, which has become even more important because very effective new treatments have now become available.6–9
The established classification criteria for AS rely on the combination of clinical symptoms plus unequivocal radiographic sacroiliitis of at least grade 2 bilaterally or grade 3 unilaterally.10 The radiographs are often normal when first symptoms arise and it usually takes several years for definite radiographic sacroiliitis to evolve. Thus, the diagnosis of AS is commonly delayed by 8–11 years after the onset of symptoms.11–13 As a result, diagnosing axial SpA (AS and uSpA with predominant axial involvement but without radiographic sacroiliitis) in the absence of radiographic sacroiliitis poses a major challenge to many physicians and rheumatologists. None the less, patients with axial SpA represent a spectrum of the same disease, and the presence or absence of radiographic (bony) changes is rather an indicator for severity or disease duration than for different disease entities. Attempts have been made in the past to classify SpA with predominant axial involvement before changes are detectable by radiography.14–20 At present, making the diagnosis of axial SpA at an early stage is difficult and highly dependent on clinical experience and intuition of the treating physician. The most often cited classification criteria for SpA are the European Spondylarthropathy Study Group (ESSG) criteria that were proposed in 1991.14 The introduction of uSpA as one SpA subtype for classification of patients with features characteristic for SpA but not fulfilling the criteria for one of the defined subtypes was a major step forward in the ESSG criteria. However, in a recent study from Spain the performance of the ESSG criteria as diagnostic criteria in daily practice was moderate: only 46.6% of patients with possible SpA who all met the ESSG criteria at entry into the study were judged by their rheumatologists to have SpA after 5 years of follow up.19,20
We demonstrate that in patients with IBP but without radiographic sacroiliitis, an early diagnosis of axial SpA can be made with a high degree of confidence when at least two to three SpA features (clinical findings, laboratory tests, or skeletal imaging) are present. The decision trees proposed herein will help the physician in making an early diagnosis of axial SpA with greater confidence.
METHODS
The term “axial SpA” we use in this study includes AS and uSpA without radiographic sacroiliitis but with clinically predominant axial involvement. Clinical SpA features of axial SpA include IBP, alternating buttock pain, enthesitis, arthritis, dactylitis, acute anterior uveitis, a positive family history, and a good response to non-steroidal anti-inflammatory drugs (NSAIDs). Associated laboratory findings include raised acute phase reactants, HLA-B27 association, and abnormalities on skeletal imaging. The sensitivities, specificities, and positive likelihood ratios (LRs) of all these SpA parameters were extracted from published studies.10,12,14,21–44 Table 1 presents the size of the study groups and type of patients (AS or SpA) and controls (healthy controls or patients with musculoskeletal diseases other than SpA) of each of the studies, together with figures for sensitivity and specificity of each SpA parameter. As can be seen in table 1, the figures for sensitivity and specificity of individual SpA features were preferentially selected, if possible, from patients with AS (in contrast with the whole group of SpA) and from back pain controls (in contrast with healthy controls or patients with diseases other than SpA). In studies where the distinction between AS and SpA, and back pain controls and other controls, respectively, was not made we had to take figures for the whole group of SpA and controls (table 1). We then estimated an average figure for sensitivity and specificity for each parameter which appeared to be representative to be used in our calculations (shown in bold letters in table 1). In general, we decided on rather conservative estimates in order not to overestimate either sensitivity or specificity of an individual SpA feature.
Sensitivity, specificity, and positive likelihood ratios (LRs) of clinical and laboratory SpA features in patients with ankylosing spondylitis (AS), controls with back pain, patients with any spondyloarthritis, or any controls. Listing of references according to the year of publication
Scintigraphy of the sacroiliac joints can be helpful if unilateral sacroiliitis is present but, in general, scintigraphy showed a limited sensitivity and specificity of about 50% for each when appropriate controls were used.45,46 Because such figures do not change the disease probability, whether sacroiliitis on scintigraphy is present or absent, scintigraphy was not included in our calculations.
We did not include measures of spinal mobility tests such as Schober’s test because low to moderate sensitivities or specificities, or both, were reported in previous studies.22,25,34 Moreover, in patients with early axial SpA such figures can be expected to be even lower than in advanced disease.10,23
Pretest probability: prevalence of axial SpA among patients with low back pain
The starting point in our calculations was the prevalence of axial SpA (including AS and axial SpA without radiographic sacroiliitis) among patients with any kind of chronic LBP—that is, back pain of >3 months’ duration. Among patients with chronic LBP the prevalence of AS was found to be 4.6% in one study,32 and in another study the prevalence of SpA (includes AS and uSpA) was found to be 5%.33 Therefore, a prevalence of 5% for axial SpA is assumed to be representative among patients with chronic LBP attending primary care.
Pretest probability, sensitivity, specificity, post-test probability, and likelihood ratios
The knowledge of the sensitivity and specificity of a diagnostic test in combination with the pretest probability—that is, the prevalence of the target disorder, allows calculation of the post-test probability of the target disorder after a positive or negative test. In the case of a positive test result the post-test probability of having the disease is equivalent to the positive predictive value.47–49
The post-test probability can be calculated by applying the following formula based on Bayes’ theorem which is available at our website (http://www.rheumatologie-berlin.de/web/de/med_pre.htm). The probability of the presence of the disease in case of a positive test is:

and the probability of the presence of the disease in the case of a negative test is:

If a test is performed when the pretest probability is low—which is the case for axial SpA in general practice—this will hardly result in a high enough post-test probability and will therefore not suffice for making a diagnosis. Combining several tests, in that the post-test probability of the first test becomes the pretest probability of the subsequent test, can solve this problem.48,49 Accordingly, various tests have been combined in this study to assess the overall disease probability.
An LR expresses the odds that a given level of a diagnostic test result would be expected in a patient with (as opposed to someone without) the target disorder.49 LRs capture both sensitivity and specificity of a given test parameter in a single figure and may thus allow for better comparisons of diagnostic tests. Therefore, positive LRs are presented in table 1 in addition to sensitivity and specificity. LRs are defined as follows:

if the parameter is present and

if the parameter is absent.
Incorporation of negative test results
If negative test results are incorporated in the probability calculations they will usually decrease the disease probability. In a patient presenting with chronic back pain the following features if negative have been incorporated in the calculations: IBP, HLA-B27, response to NSAIDs, magnetic resonance imaging (MRI), and acute phase reactants. HLA-B27 testing gives a clear-cut yes/no answer with very few typing errors and is not subject to change. The absence of IBP, a lack of clinical response to NSAIDs, and a negative MRI should probably also be considered as truly negative test results and incorporated accordingly, although further studies to confirm the reported sensitivities and specificities are needed. For acute phase reactants there are no data on the consistency of findings in individual patients. Thus, negative findings should be incorporated with caution. Thus, in our opinion most clinical features should not be considered definitely negative in a given situation because they may turn positive in the future. Taking the family history may not be possible if family members are not available. Thus, negative assessments may be falsely negative. For these reasons we did not perform calculations for the latter features if they were negative.
RESULTS
Table 1 shows the study characteristics on which the calculations were based, and the sensitivities, specificities, and LRs of the various test parameters, together with the estimated average figure for each parameter. Table 2 shows examples of the resulting post-test probabilities, depending on the features present in a given patient. IBP has generally been accepted to be the leading symptom of the axial type of SpA and assessment of IBP was therefore used as the first diagnostic step. The probability of having axial SpA in a patient presenting to a physician because of symptoms suggesting IBP is only around 14%, if we assume the background prevalence of axial SpA to be 5%. To reach a high enough probability of axial SpA (that is, 90%), additional findings are needed; these can be clinical features, laboratory tests, and skeletal imaging procedures typical of axial SpA (table 2). In general, a probability of at least 90% can be achieved if IBP plus two to three further features are present. The sequence of the tests applied does not affect the final disease probability and can therefore be adjusted according to the physician’s preferences and/or experiences.
Selection of possible combinations of features in patients with low back pain presenting to primary care. The pretest probability refers to the prevalence of axial spondyloarthritis (SpA) among patients with chronic back pain, the post-test probabilities result from the presence (+) or absence (−) of various SpA features
Sensitivity analysis
The post-test probability of having axial SpA depends on the pretest probability—that is, the prevalence of the disease. A prevalence of axial SpA of 5% among patients with chronic back pain was assumed in our calculation because this figure appears to be representative based on available data.32,33 To increase the pretest probability of 5% to a post-test probability of around 90% a combination of several features, such as IBP, acute anterior uveitis, and HLA-B27 positivity, for example, is required. If the disease prevalence were lower or higher than 5%, then different post-test probabilities would emerge for the same features present. Table 3 shows examples for various prevalences of the disease and resulting post-test probabilities. Overall, the deviation of the resulting post-test probabilities was small if plausible figures for disease prevalence such as 2–3% or 7%, respectively, were taken.
Sensitivity analysis
A sensitivity analysis can also be done for each SpA feature in that different sensitivities and specificities are assumed according to the reported variation of these figures in different studies. A more detailed analysis on all SpA parameters shown in table 1 can be done but would be beyond the scope of this article. One example of such analysis has been done for the feature heel pain (enthesitis) alone and in combination with the additional variation of the prevalence, the results of which are also presented in table 3.
Diagnostic algorithm
For daily clinical practice we suggest the following two diagnostic algorithms:
-
For a physician experienced in taking care of patients with rheumatological problems, such as a rheumatologist, it seems logical that the assessment of IBP is going to result in the evaluation of other clinical features (fig 1), and this may be followed by HLA-B27 testing and skeletal imaging.
-
For a physician less experienced in taking care of patients with rheumatological problems, such as a primary care physician or a general practitioner (GP), the clinically assessed presence of IBP (14% probability of axial SpA) can be followed by testing for HLA-B27. A positive test result would mandate a subsequent referral to a rheumatologist for further evaluation because the probability of axial SpA in such a patient has risen to 59% (fig 2).

Decision tree on diagnosing axial SpA. Starting point is the presence or absence of inflammatory back pain (IBP) in patients presenting with chronic back pain. In general, for making the diagnosis of axial SpA a disease probability >90% is suggested. *Dependent on which features are positive (table 2). **If the probability of disease exceeds 90% we consider the diagnosis axial SpA as definite, if the probability is 80–90% we consider the diagnosis as probable (see also “Discussion”).
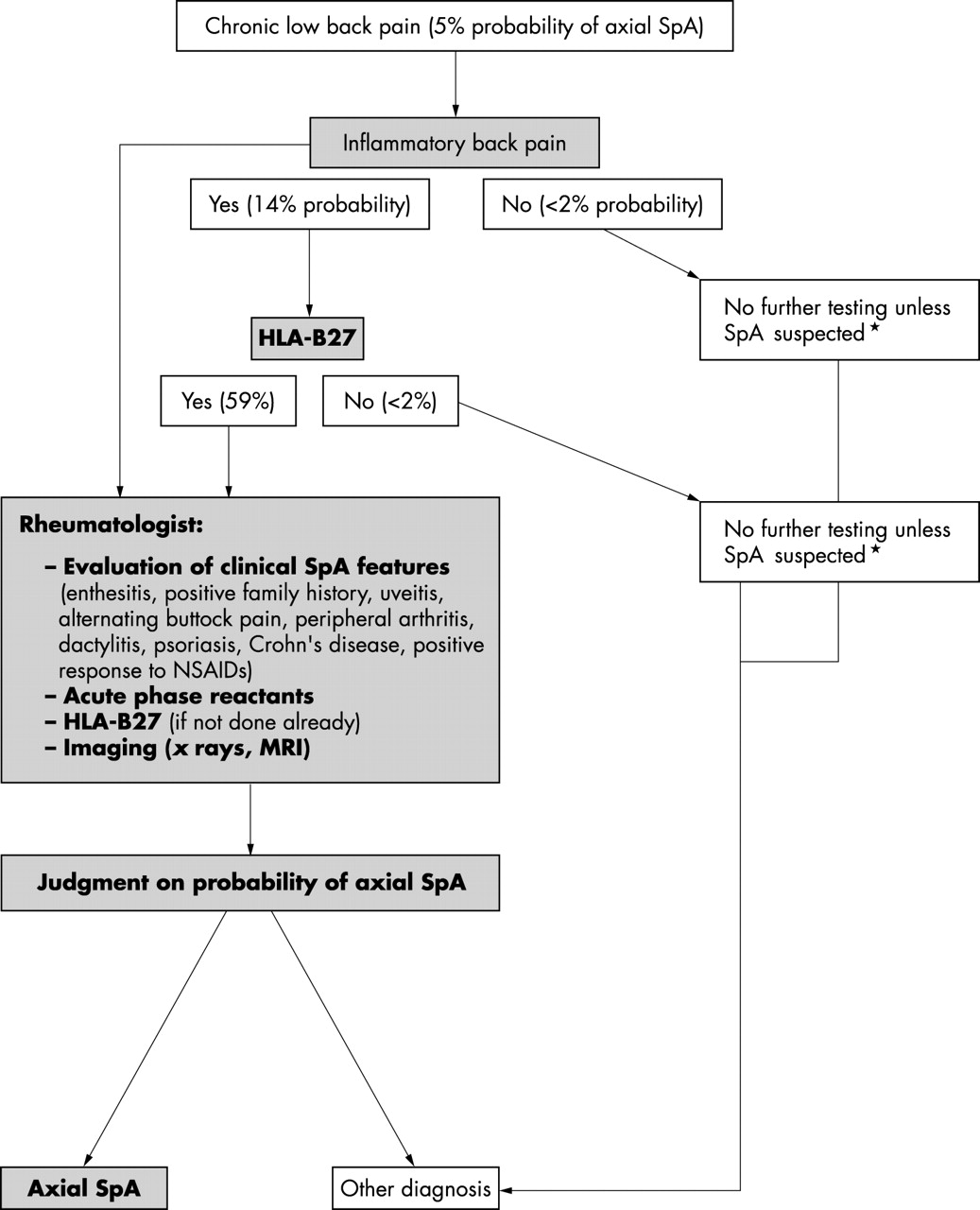
{kind=link}
{kind=link}
Approach to the diagnosis of axial SpA in daily practice for the physician less experienced (GP) in dealing with patients with rheumatic disease. Percentages in brackets indicate the probability of axial SpA before (pretest probability) and after a test has been performed (post-test probability). *Suspicions for SpA could be the presence of several other clinical features.
DISCUSSION
The primary aim of this study is to provide data on the probability of early axial SpA in patients with chronic back pain according to the absence or presence of certain clinical features, laboratory tests, or findings on skeletal imaging. The final post-test probability, which incorporates all relevant SpA features, may then help in confidently making the diagnosis of early axial SpA. The formula applied in this study is based on Bayes’ theorem and allows calculation of the disease probability for any individual patient according to the clinical presentation. In general, the presence of IBP plus three further typical SpA features (table 2) results in a probability of about 90% for axial SpA. If a combination of SpA features with high LR such as acute anterior uveitis (LR 7.3), HLA-B27 (LR 9.0), or MRI (LR 9.0) is present, then the presence of IBP plus two such features may be sufficient to reach a probability of disease of ⩾90%. Such a high disease probability with an acceptable error rate should lend sufficient confidence for making the diagnosis of axial SpA. This is in accord with the generally accepted principles of decision analysis.49 If the probability is 80–89% we would consider the diagnosis of axial SpA as probable or highly probable.
We chose IBP as the entry criterion for the assessment of patients with chronic back pain because IBP is the key symptom of axial involvement in SpA, and is present in the great majority of patients with AS and in about 70% of all patients with SpA.12,14,50 If a patient with chronic LBP does not have IBP the probability of having axial SpA falls to less than 2%. Unless other clinical features such as the presence or history of uveitis, enthesitis, or others strongly suggest the presence of SpA we do not recommend any further testing, including tests for HLA-B27, in such a patient because even a positive test result would not increase the probability of SpA to more than 13%. Using the same methodological approach, we have recently proposed a diagnostic investigation for reactive arthritis, in which peripheral arthritis is the predominant symptom.51
The value of HLA-B27 as a diagnostic tool for early AS has been a subject of longstanding debate that has not yet been clarified. In several papers the advantages and disadvantages of HLA-B27 as a diagnostic test for AS/SpA have been discussed.52–56 Some authors emphasised the great value of HLA-B27,17,34 but it was generally felt that for a patient presenting with only chronic LBP the test would not be of much clinical value because the post-test probability after a positive HLA-B27 test would not exceed 30% assuming a pretest probability of 5%.54,55
The major difference between those earlier studies and our approach is that in the earlier studies HLA-B27 was considered as the only test in the probability calculations, whereas the concept of combining tests,48,49 as we have done, was not used. This is because the data on sensitivity and specificity for most of the clinical features that we have used for our analysis have only recently become available as a result of recent large international studies.14,16,27–31 Our calculations show that HLA-B27 testing makes sense as long as it is used in combination with the relevant clinical, laboratory, or imaging parameters.
The outstanding value (in many but not all population groups) of HLA-B27 compared with other tests for diagnosing SpA is its high sensitivity and high specificity, which results in a high LR. Moreover, unlike the clinical criteria and imaging discussed here, HLA-B27 is neither dependent on the physician’s experience nor on the patient’s memory. HLA-B27 testing is relatively cheap and reliable, it needs to be ordered only once, and it always gives a “yes” or “no” result. It is of note that HLA-B27 was the strongest single parameter in the distinction between SpA and non-SpA in the ESSG classification criteria.14
None the less, HLA-B27 was removed from the set of ESSG criteria because the ESSG criteria had to be applicable to populations in field studies without the need for a laboratory. We would like to point out that in non-white populations, who have either a high background prevalence of HLA-B27 in the general population (resulting in a lower specificity) or a less strong disease association (resulting in a lower sensitivity), the diagnostic value of HLA-B27 will be somewhat different.54,57
The sequence of tests applied in the diagnostic investigation in daily practice is determined by many factors, such as the physician’s preference, clinical experience, and availability of the tests and their costs. In any case, in a search for axial SpA in a patient with back pain the presence or absence of IBP should be examined first. Many rheumatologists classify back pain as IBP if four of the following five features are present: (a) age at onset <40 years; (b) duration of back pain >3 months; (c) insidious onset; (d) morning stiffness; and (e) improvement with exercise.22 If IBP is present the experienced rheumatologist will assess other clinical features (family history, enthesitis of the heel, arthritis, dactylitis, uveitis, good response to NSAIDs, etc) at the initial visit before considering ordering pelvic x ray examinations or tests such as erythrocyte sedimentation rate (ESR), C reactive protein (CRP), or HLA-B27.
We suggest that the non-rheumatologist uses a different approach because most of the parameters listed in fig 1 are often not easy to assess in patients with chronic back pain: after making a diagnosis of IBP (based on appropriate criteria), such a physician may next order an HLA-B27 test. This physician should then refer the patient with a positive test result to a rheumatologist for further evaluation because at this stage the disease probability of axial SpA is about 60% (fig 2). Such a structured approach is likely to decrease rather than increase the overall costs because currently HLA-B27 testing, along with musculoskeletal imaging, is being ordered often inappropriately by primary care physicians.58 To apply this approach in primary care it will be an important task to teach the primary care physicians the characteristics of IBP.21,22 Acute phase reactants such as CRP and ESR are often used for the diagnostic investigation of inflammatory rheumatic diseases. However, their clinical use is somewhat limited for diagnosing axial SpA because of their moderate sensitivity (only about 50%), although they do have some clinical value (with an estimated LR of 2.5).7,12,34–36
As an alternative approach, the non-specialist might be advised to refer to the rheumatologist for further evaluation any patient with the clinical symptom of IBP, or any patient with chronic back pain with a positive HLA-B27 test. Choosing IBP alone would have the advantage that the non-specialist is not encouraged to misuse HLA-B27 testing. However, according to our calculations (post-test probability 14%) the rheumatologist has to see about seven patients to make the diagnosis of axial SpA in one of them. Furthermore, it might not be easy for the non-specialist to assess IBP. The advantage of using HLA-B27 testing as the first and sole test in a patient with chronic LBP (post-test probability 33%) is that no experience in the interpretation of clinical symptoms is necessary for the non-specialist. In this case the rheumatologist has to see three patients to make a diagnosis in one. At this moment we prefer the approach presented in fig 2 (combining assessment of IBP and HLA-B27 testing) before referral to the rheumatologist. Clearly, this issue is open to discussion and preferences will also depend on the local situation and availability.
Imaging is an important tool in the diagnostic investigation. If a pelvic radiograph shows definite sacroiliitis in a patient with IBP, this would be sufficient to classify the disease as AS.10 If, however, the radiograph is negative, the diagnosis of axial SpA can still be made if a high enough disease probability is reached based on the presence of other features. The appearance of radiological changes in the majority of patients with axial SpA is probably only a matter of time, but currently we do not know exactly the proportion of patients progressing to definite AS over time. In one study 60% of such patients had developed definite AS after 10 years of follow up.12 It took an average of 9 years (+/− 6 years) for radiological sacroiliitis to appear in these patients with AS.12 A further 20% still had chronic uSpA and might have developed radiological sacroiliitis if their follow up had been continued for a longer time. It needs to be shown in future studies if radiologically detectable sacroiliitis should be regarded as a surrogate marker for severity, similar to the radiographic erosions in rheumatoid arthritis.
MRI is considered very helpful in detecting signs of sacroiliitis that are not yet visible on plain radiographs. However, special fat suppression techniques or application of gadolinium are necessary for acute inflammatory changes to be detectable on MRI with a high degree (90–100%) of sensitivity and specificity.40–44 None the less, further MRI studies with appropriate techniques and including patients with non-inflammatory (mechanical or non-specific) back pain are warranted to confirm these data. In the absence of such data, we decided to choose rather conservative figures for sensitivity and specificity for our calculations. Moreover, as compared with clinical signs, such as acute anterior uveitis (diagnosed by an ophthalmologist) or an HLA-B27 test, MRI results may be ambiguous, particularly if the sacroiliitis is minor. The limited availability and high costs of MRI further hamper the widespread use of this technology. Therefore, in the diagnostic algorithm proposed herein the ordering of an MRI is the final diagnostic step. If the probability of axial SpA in a given patient with normal or equivocal radiograph of the sacroiliac joints does not exceed 50–70%, a positive MRI scan enables one to make the diagnosis of axial SpA (probability of ⩾90%), whereas a normal finding on MRI may help to render the diagnosis as unlikely (probability 10–20%).
In this study we used sensitivities and specificities from several studies conducted both in AS and the whole group of patients with SpA. We estimated average figures for each diagnostic test based on these studies, but we are well aware that applying different sensitivities and specificities may lead to different probabilities. To illustrate such an effect, we performed sensitivity analyses for the pretest probability by applying prevalence figures for axial SpA of as low as 2–3% and as high as 7%, and also by applying various sensitivities and specificities for enthesitis as one example of the clinical parameters (table 3). The data show that the influence of this range of variation on the final disease probability is moderate to small. The serial application of the various tests assumes that the tests are independent. It is well recognised that often this is not the case. For example, a “positive family history” and “HLA-B27” may not be independent tests. This problem of “convergence” is usually clinically not important if no more than two to three diagnostic components are applied.49 To what extent any convergence will reduce the final post-test probability in the diagnostic investigation of suspected axial SpA cannot be deduced from the data presently available. However, we regard a considerably lower final post-test probability as unlikely. When these limitations are taken into account, the post-test probabilities given herein should be regarded as estimates and the validity of this diagnostic approach has to be confirmed in prospective clinical studies in which the expert’s opinion might serve as the “gold standard”.
Classification criteria do not have the medical standing for making a diagnosis, as discussed by Fries et al.59 Nevertheless, classification criteria are frequently used in daily clinical practice for diagnostic purposes.16,60 In a patient with IBP, the fulfilment of the ESSG criteria for SpA classification requires the presence of only one further feature14; the probability of the presence of SpA in such a clinical setting ranges between 25 and 51% according to our calculations. For use in daily practice just meeting the ESSG criteria with a probability of not more than 51%, however, is in our opinion not sufficient to make a diagnosis of axial SpA. This view is strongly supported by the Spanish study on patients with possible SpA.19
The Amor criteria,15,16 like the ESSG criteria,14 are designed as multiple entry criteria which aim at encompassing the whole spectrum of SpA. In the Spanish follow up study 76.5% of those patients with possible SpA who had initially fulfilled the Amor criteria developed SpA (according to the expert opinion) compared with 46.6% of those who had initially fulfilled the ESSG criteria,19 indicating that the Amor criteria perform somewhat better than the ESSG criteria. The better performance of the Amor criteria can be easily explained by the data on disease probability presented herein because according to our calculations, similar to the Amor criteria, at least three to four features need to be present to make a definite diagnosis. In contrast with the Amor multiple entry criteria, a single entry criterion (IBP) is felt to be more helpful for a structured diagnostic approach in patients with LBP. Furthermore, MRI is not included in the Amor criteria because at the time the criteria were developed this technique had not yet been established in axial SpA.
In summary, we present a new approach to help clinicians diagnose axial SpA at an early stage in patients with IBP but without radiographic sacroiliitis. The decision trees proposed herein were developed by assessing the probabilities of the presence or absence of axial SpA in patients with chronic LBP, according to the presence or absence of the various clinical features, and also using the results of laboratory tests and skeletal imaging. We have shown that in the absence of definite radiological sacroiliitis at least two to three SpA features (clinical findings, laboratory tests, or skeletal imaging), in addition to the IBP as the starting point, are necessary to make a diagnosis of axial SpA with high degree of confidence. Testing for HLA-B27 among patients (of European descent) with IBP who do not show unequivocal radiological sacroiliitis can play a central part in the diagnostic investigation of axial SpA. Furthermore, for the first time, a role for MRI in such a diagnostic investigation has been analysed. A prospective study to confirm the clinical usefulness of this approach is in progress.
Acknowledgments
This study was supported by the BMBF (Kompetenznetz Rheuma), FKZ 01GI9946.