Article Text

Abstract
Objective: to estimate and visualise the efficacy of treatment with etanercept (Enbrel) in patients with rheumatoid arthritis (RA) using colour Doppler and spectral Doppler ultrasonography to determine the possible changes in synovial perfusion during a one year observation period.
Methods: Eleven patients from the European multicentre trial of the efficacy and safety of etanercept were included in this study when transferred into the open label, long term safety, and efficacy study. Before a scheduled dosage increase to 50 mg/week they were examined clinically, serologically, and by ultrasonography using the colour Doppler pixels and the spectral Doppler resistance index (RI) as indicators of inflammation. The patients were re-examined at two weeks and at one year follow up
Results: The clinical activity decreased significantly from baseline to week 2, but no significant changes were seen from baseline to one year. The number of coloured pixels in each region of interest decreased from baseline to week 2 with a median reduction of 60% (p=0.005). This effect on the perfusion in the synovium could not be found after one year of treatment. During the initial treatment we detected an increase in synovial RI by spectral Doppler. The median increase in peripheral resistance from baseline to week 2 as estimated by the mean RI was 22.6% (p=0.005). The increase in peripheral resistance was maintained to some extent after one year (mean RI increased by 18.8% p=0.074).
Conclusion: Ultrasonography seems to be a promising tool for the detection of treatment response using spectral Doppler and pixel estimation.
- etanercept
- Doppler ultrasonography
- rheumatoid arthritis
- RA, rheumatoid arthritis
- RI, resistance index
- ROI, region of interest
- TNFα, tumour necrosis factor α
Statistics from Altmetric.com
Ultrasound can depict soft tissue hyperaemia in musculoskeletal inflammatory disease1 and allows a sensitive detection of synovitis.2–4 Disease activity and treatment response may be estimated by Doppler ultrasound.5,6 In a previous study we found that the Doppler ultrasound technique reliably measured synovial vascularisation (coloured pixels) and flow pattern.6
During the progression of rheumatoid arthritis (RA), angiogenesis in hypervascularised pannus appears to be a prerequisite for damage to cartilage and bone.7,8 The importance of tumour necrosis factor α (TNFα) in the inflammatory process has been indicated by several studies.9,10 The release of TNFα results in local activation of vascular endothelium, release of nitric oxide with vasodilatation, and increased vascular permeability.11
The purpose of this study was to estimate and visualise the efficacy of treatment with etanercept in patients with RA by colour Doppler and spectral Doppler ultrasonography to determine the possible changes in synovial perfusion during one year.
PATIENTS AND METHODS
This study was conducted in accordance with local regulations, with the Declaration of Helsinki, and with the ICH guidelines for Good Clinical Practice in the European Community.
The 11 patients in this study were part of a group of 13 patients who participated in a three month, double blind, placebo controlled, multicentre trial of the efficacy and safety of etanercept (placebo n=3, 10 mg once weekly n=4, 10 mg twice weekly n=1, 25 mg once weekly n=3, and 25 mg twice weekly n=2) and an open label extension study of long term safety and efficacy. Their mean age was 59 years (range 42–70) and mean duration of RA 10 years (range 4–35). The 11 patients who continued in our ultrasound study all had an increase in dose after the baseline evaluation. One of the 11 patients only participated until week 2 of the study, when the patient was excluded owing to a borderline value of anti-DNA antibodies. Two patients from the original etanercept study group were not included in our study as they received an unchanged dose of etanercept 25 mg twice weekly. The patients were evaluated at baseline (n=11), week 2 (n=11), and one year (n=10) of the open label trial to detect clinical, serological, and ultrasonographic changes. No injections of corticosteroids were given during the study.
To avoid bias in the ultrasound examination, five control patients with a similar RA (two wrists and three metacarpophalangeal joints) were also examined. All patients and controls were examined on the same occasions and in a randomised order by an ultrasound specialist not otherwise involved in the treatment.
The baseline values of the 11 patients in this study have been published previously.6
Ultrasonography
An Acuson Sequoia ultrasound system (Mountainview, California, USA) was used for the ultrasonographic examinations equipped with an 8–15 MHz linear array transducer with a centre frequency of 13 MHz.
Blood flow in the synovial membrane of the target joints was visualised with colour Doppler. The Doppler settings were kept unchanged at all measurements. The target joints in this study included five wrists and six metacarpophalangeal joints.
On ultrasound examinations the borders of the region of interest (ROI) were defined by an estimate of the synovial membrane situated between the muscle/tendon above and the bone surfaces below; in all cases examinations were performed by one investigator to reduce variation. The number of coloured pixels was expressed in relation to the total number of pixels in the ROI as previously described.6
The resistance index (RI), defined as (peak systolic velocity − end diastolic velocity)/peak systolic velocity, was measured by spectral Doppler ultrasonography. Three arteries were examined and the mean RI calculated. Low RI values correlate with a low peripheral resistance, indicating an increased tissue perfusion and increased disease activity.12,13
Measurements were repeated on the same joint at two weeks and one year. Standard positioning of the probe in each joint was attempted.
Statistics
Non-parametric statistical methods using the statistical package SPSS version 10.0 (SPSS Inc, Chicago, Illinois) were applied with a level of significance of 0.05.
The visits were compared in pairs using the Wilcoxon signed rank sum test. Correlation between the clinical and ultrasonographic parameters was estimated by Spearman’s rs.
RESULTS
Table 1 gives the clinical and ultrasound data and the changes during treatment with etanercept.
Clinical and ultrasonographic data during the observation period
The clinical activity decreased from baseline to week 2 and similar significant changes were found after one year of treatment. Synovial thickness as measured by ultrasound did not change from baseline to week 2 or from baseline to one year (table 1). During the initial treatment, an increase in synovial RI was detected. The flow profile of the arteries measured with spectral Doppler showed low vascular resistance—that is, they showed a persistent flow during the diastole at baseline. The number of coloured pixels per ROI decreased significantly from baseline to week 2 (figs 1 and 2). This effect on the perfusion in the synovium could not be found after one year of treatment. The mean RI increased from baseline to week 2 and a tendency towards an increase was found after one year, but this was not statistically significant.

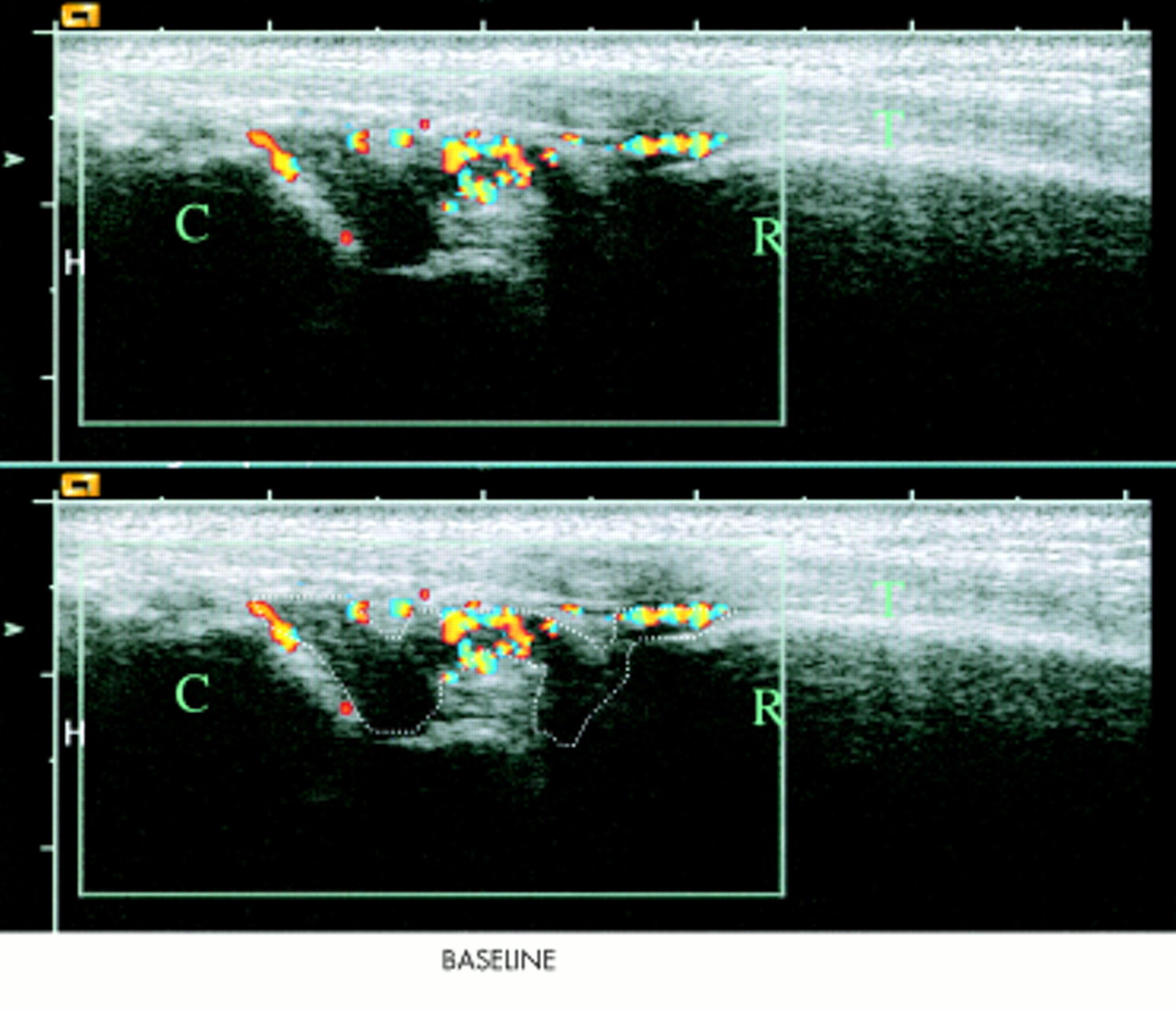
Longitudinal scan of the right wrist at baseline with the radial bone marked as R, the carpus marked as C, and the extensor digitorum tendon marked as T. The hypervascular nature of the synovium is illustrated with colour Doppler and the region of interest (the hypertrophic synovium) is outlined. A false appearance of flow inside the bone is due to an artefact.

{kind=link}
{kind=link}
Longitudinal scan of the right wrist at week 2 with the radial bone marked as R, the carpus marked as C, and the extensor digitorum tendon marked as T. The hypervascular nature of the synovium is illustrated with colour Doppler and the region of interest (the hypertrophic synovium) is outlined. Compared with the baseline examination, there is a marked decline in Doppler activity at week 2 follow up and most of Doppler activity found is localised outside the hypertrophic synovium, and is not used in our measurements.
DISCUSSION
We found that the spectral Doppler examination at baseline was characterised by a diastolic flow—that is, the flow persisted during the diastole. After two weeks of full etanercept treatment, we found an increase in peripheral vascular resistance in the synovium and a diminished number of coloured pixels per ROI, indicating diminished flow in the examined area. This corresponds well with previous findings of decreased vascularity in synovial biopsy tissues from patients treated with etanercept.14
TNFα induces local activation of vascular endothelium, release of nitric oxide with vasodilatation, and increased vascular permeability.11 Treatment which blocks this cytokine would be expected to decrease vascular permeability and diminish vasodilatation. We would expect spectral Doppler ultrasound examination to show that treatment was associated with an increase in RI of the inflamed joint, a decrease in the number of coloured pixels per ROI (diminished vasodilatation), and normalisation of the flow curve—that is, diminished or non-existent diastolic flow. This corresponds with our finding of an increase in peripheral vascular resistance, reflecting a regression in the inflammatory activity.
In accordance with a recent observation of the acute effect of etanercept,15 the most marked effect was seen in our patients within the first two weeks. This was indicated both by the increase in peripheral resistance and the decrease in coloured pixels per ROI, corresponding with the improvement in clinical parameters (including the diminished swelling in the target joint). After one year, there was still a tendency towards an increase in the peripheral resistance (that was not, however, statistically significant at the 5% level), corresponding to an improvement in such clinical variables as visual analogue scale, Health Assessment Questionnaire, morning stiffness, doctor’s global assessment, and patient’s global assessment.
It may be concluded that ultrasonography is a promising tool for the detection of treatment response using spectral Doppler and pixel estimation.
Acknowledgments
The study was supported by Danish Health Foundation and the Oak Foundation.