Article Text

Abstract
Objective: To examine differences in autoantibody response and immunogenetic background between patients with systemic sclerosis (SSc) and those with other autoimmune diseases who had serum anti-Th/To antibodies.
Methods: Serum samples from 1048 Japanese patients with various autoimmune diseases were screened for anti-Th/To antibodies using RNA and protein immunoprecipitation assays. The reactivity to RNase P subunits was examined by immunoprecipitating 35S labelled recombinant Rpp38, Rpp30, and hPop1 produced by in vitro transcription and translation. HLA-DRB1, DQB1, and DPB1 alleles were identified using a polymerase chain reaction followed by a restriction fragment length polymorphism assay.
Results: Serum anti-Th/To antibodies were detected in 14 of 303 patients with SSc and seven of 745 patients without SSc (4.6% v 0.9%; p=0.0003). Similar percentages of patients with and without SSc showed immunoreactivity to Rpp38 and Rpp30, but more patients with SSc than patients without SSc showed a reactivity to hPop1 (93% v 14%; p=0.002). In patients with anti-Th/To antibodies DRB1*1502 or *0802 was detected more often, and the DRB1*0405-DQB1*0401 haplotype less often in patients with SSc than in patients without SSc (79% v 14%, p=0.02, and 7% v 71%, p=0.01, respectively).
Conclusions: Anti-Th/To antibodies were detected in a small proportion of autoimmune patients lacking clinical features related to SSc. A close relationship between disease expression and anti-hPop1 reactivity as well as HLA class II alleles in anti-Th/To positive patients suggests that the process of anti-Th/To antibody production may be different between patients with and those without SSc.
- autoantibody
- scleroderma
- ACA, anticentromere antibodies
- ITP, idiopathic thrombocytopenic purpura
- PCR, polymerase chain reaction
- PM/DM, polymyositis or dermatomyositis
- RA, rheumatoid arthritis
- RNPs, ribonucleoproteins
- SLE, systemic lupus erythematosus
- SS, Sjögren's syndrome
- SSc, systemic sclerosis
- antitopo I, antitopoisomerase I
Statistics from Altmetric.com
- ACA, anticentromere antibodies
- ITP, idiopathic thrombocytopenic purpura
- PCR, polymerase chain reaction
- PM/DM, polymyositis or dermatomyositis
- RA, rheumatoid arthritis
- RNPs, ribonucleoproteins
- SLE, systemic lupus erythematosus
- SS, Sjögren's syndrome
- SSc, systemic sclerosis
- antitopo I, antitopoisomerase I
Anti-Th/To antibody is one of the autoantibodies related to systemic sclerosis (SSc). It is also associated with limited cutaneous SSc, in which there is a low frequency of serious internal organ involvement.1,2 This antibody response was initially reported to be specific for SSc or Raynaud's disease with a short disease duration,1 but was recently detected in patients with localised scleroderma as well.3 The anti-Th/To antibody was first identified as an antinucleolar antibody that immunoprecipitated ribonucleoproteins (RNPs) associated with H1/8–2 and Th/7–2 RNAs,4,5 which are components of the RNA processing enzymes RNase P and RNase MRP, respectively.6 RNase P is involved in the maturation of tRNA and RNase MRP is involved in processing pre-rRNA.6 Because anti-Th/To positive serum precipitates H1 and Th RNAs together, the Th/To antigen is thought to be a protein component shared by RNase P and RNase MRP. Recently, the molecular structure of these two enzymes has been extensively analysed, and several protein subunits were identified by molecular cloning technology. At present, seven human RNase P subunit proteins have been identified and of these, Rpp38, Rpp30, Rpp29/hPop4, and hPop1 are associated physically with both RNase P and RNase MRP.6 Rpp38, Rpp30, and hPop1 have been reported to carry antigenic determinants recognised by anti-Th/To antibodies in patients' serum samples,7,8 but the clinical relevance of these reactivities has not been determined.
In this study, serum samples from patients with various autoimmune diseases were screened for anti-Th/To antibodies, and reactivities to RNase P subunits and HLA class II alleles were compared between patients with and without SSc who had anti-Th/To antibodies.
PATIENTS AND METHODS
Patients and controls
Serum samples from 1048 Japanese patients, including 303 (29%) patients with SSc and 745 (71%) patients with other autoimmune diseases, were examined in this study. All patients with SSc satisfied the American College of Rheumatology preliminary classification criteria for SSc.9 Ninety five (31%) and 208 (69%) patients with SSc were classified as having diffuse and limited cutaneous SSc, respectively. Ninety one (30%) patients were positive for antitopoisomerase I (antitopo I) antibodies and 51 (17%) had anticentromere antibodies (ACA). Organ involvement in SSc was defined according to previously described criteria.2 Patients with other systemic autoimmune diseases included 392 (53%) with systemic lupus erythematosus (SLE), 40 (5%) with polymyositis/dermatomyositis (PM/DM), 148 (20%) with rheumatoid arthritis (RA), and 72 (10%) with primary Sjögren's syndrome (SS). Ninety three patients with idiopathic thrombocytopenic purpura (ITP) who lacked clinical features related to SLE were also analysed as an organ specific autoimmune disease control. Prevalence of Raynaud's phenomenon was 99% in SSc, 29% in SLE, 45% in PM/DM, 9% in RA, and 1% in ITP. All serum samples were obtained within one year after the diagnosis. Blood samples were obtained after the patients gave their written informed consent as approved by the Keio University Institutional Review Board.
Detection of anti-Th/To antibodies
All serum samples were subjected to an RNA immunoprecipitation assay using unlabelled HeLa cell extracts.10 Because anti-SSB/La antibodies immunoprecipitate newly synthesised RNA polymerase III transcripts, including H1 and Th RNAs, the serum samples that precipitated both H1 and Th RNAs were further analysed by protein immunoprecipitation with 35S labelled HeLa cell extracts. Samples that precipitated a group of six proteins ranging in size from 18 kDa to 120 kDa were regarded as positive for anti-Th/To antibodies.11
Reactivities to RNase P subunits
cDNAs encoding the entire open reading frames of Rpp38 and Rpp30 were amplified by a polymerase chain reaction (PCR) from the leukaemia cell line K562 using primer pairs the design of which was based on published sequences.7 A cDNA clone HA01242 (gene name KIAA0061) corresponding to amino acid residues 122–1024 of hPop1 was provided by the Kazusa DNA Research Institute.8 These cDNA constructs were subcloned in frame into the pT7Blue-2 expression vector (Novagen, Darmstadt, Germany). DNA plasmids encoding Rpp38, Rpp30, and hPop1 were individually transcribed with T7 RNA polymerase in the presence of STP3 transcription mix (Novagen). Each transcript was then translated in a nuclease treated rabbit reticulocyte lysate (Novagen) in the presence of 35S-methionine (ICN Biomedicals, Irvine, CA, USA). The presence of antibodies against Rpp38, Rpp30, and hPop1 was determined by immunoprecipitation in vitro of translated 35S labelled Rpp38, Rpp30, and hPop1.12
HLA class II allele typing
DRB1, DQB1, and DPB1 alleles were determined in all anti-Th/To positive patients, using restriction fragment length polymorphisms of PCR amplified DNA as described.13 As controls, HLA class II alleles were typed in 101 patients with SSc but without anti-Th/To antibodies and 104 healthy subjects who were Japanese and unrelated.
Statistical analysis
All comparisons between the two patient groups were performed using the χ2 test.
RESULTS
Frequency of anti-Th/To antibody in patients with and without SSc
Serum anti-Th/To antibodies were detected in 14 patients with SSc (4.6%) and seven patients without SSc (0.9%), and this difference was significant (p=0.0003). The seven patients without SSc but with anti-Th/To antibodies included three with RA, and one each with SLE, PM, primary SS, and ITP (table 1). Raynaud's phenomenon was found in only one of the seven patients without SSc but with anti-Th/To antibodies, and none of these patients had sclerodactyly, nail fold capillary change, or oesophageal hypomotility. Eleven of the 14 anti-Th/To positive patients with SSc had limited cutaneous SSc, and the remaining three patients with diffuse cutaneous SSc had concomitant antitopo I antibodies. Antibodies to ACA and U1RNP were positive in an additional one and two anti-Th/To positive patients with SSc, respectively.
Clinical, immunogenetic, and serological findings in patients with and without SSc with anti-Th/To antibody
Reactivities to RNase P subunits
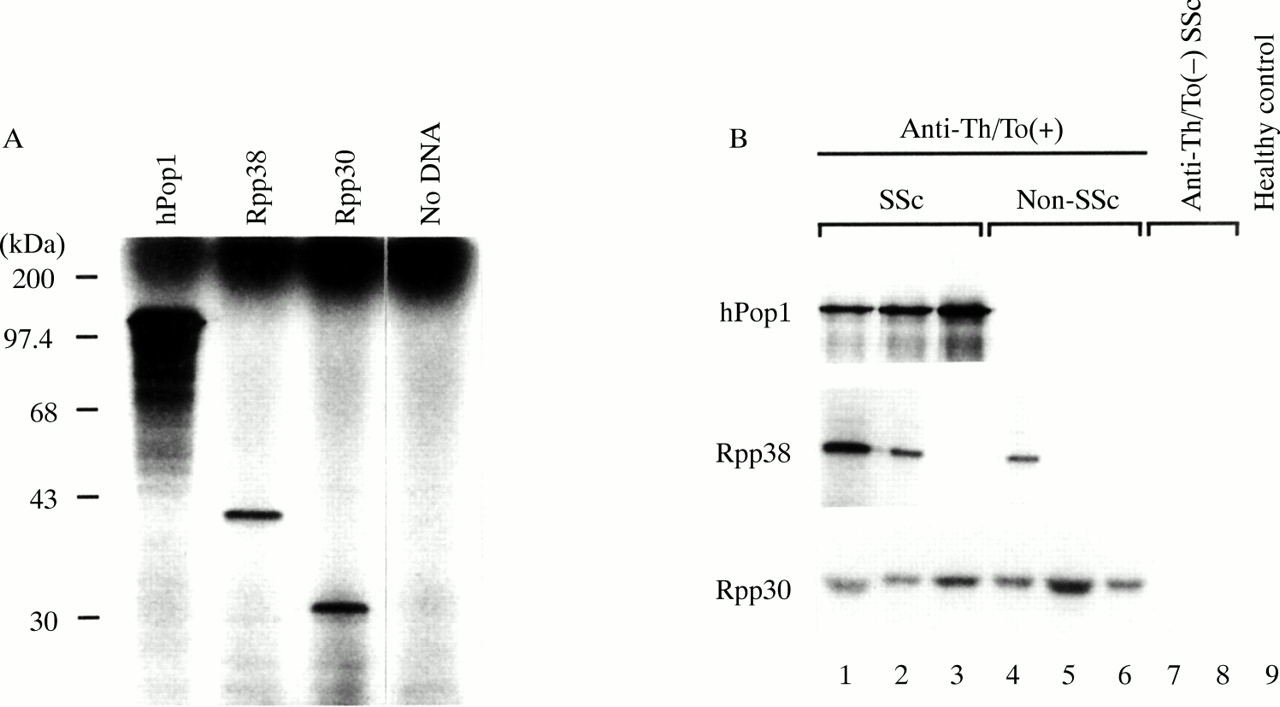
Antibody reactivities to Rpp38, Rpp30, and hPop1 were examined by the immunoprecipitation of in vitro translated recombinant proteins. Figure 1 A shows that recombinant Rpp38, Rpp30, and hPop1 incorporated radioactivity into polypeptides of the appropriate molecular sizes. Representative anti-Th/To positive serum samples with and without SSc immunoprecipitated these three subunits in various combinations (fig 1 B). None of the subunits was recognised by 40 randomly selected anti-Th/To negative SSc serum samples. Rpp38, Rpp30, and hPop1 were recognised by eight (38%), 18 (86%), and 14 (67%) samples that were positive for anti-Th/To antibodies, respectively (table 1). All anti-Th/To positive serum samples reacted with at least one of these subunits. The percentages of patients with SSc and without SSc whose serum recognised Rpp38 and Rpp30 were similar (43% v 29% and 86% v 86%, respectively). By contrast, anti-hPop1 antibody was detected in all but one patient with SSc, compared with only one of seven patients without SSc (93% v 14%; p=0.002).
{kind=link}
(A) The products of in vitro translation of hPop1, Rpp38, and Rpp30. The no DNA lane was loaded with a translation reaction containing a mock transcript without the DNA template. An aliquot of each reaction was fractionated on SDS-10% polyacrylamide gel, and 35S labelled polypeptides were visualised by autoradiography. (B) Representative immunoprecipitation of the translated polypeptides. In vitro translated products were incubated with anti-Th/To positive SSc serum (lanes 1–3), anti-Th/To positive non-SSc serum (lanes 4–6), anti-Th/To-negative SSc serum (lanes 7 and 8), and healthy control serum (lane 9), which were coupled to protein A-sepharose. Immunoprecipitated polypeptides were fractionated on SDS-polyacrylamide gels. Positive reactivities were visualised by autoradiography.
Clinical associations with reactivities to RNase P subunits
No significant association between clinical findings related to SSc and reactivities to Rpp38, Rpp30, and hPop1 were found in 14 anti-Th/To positive patients with SSc (table 1). However, a patient with RA and anti-hPop1 reactivity (patient 106) was the only patient with Raynaud's phenomenon in the non-SSc group; thus, all the patients with anti-hPop1 reactivity had SSc or Raynaud's phenomenon.
HLA class II alleles
HLA class II alleles were determined in all anti-Th/To positive patients with and without SSc, 101 anti-Th/To negative patients with SSc, and 114 healthy controls. Table 1 summarises the DRB1, DQB1, and DPB1 alleles in individual anti-Th/To positive patients. No allele was significantly increased or decreased in any of the anti-Th/To positive patients combined compared with healthy controls. Next, frequencies of individual HLA class II alleles were compared among 14 patients with SSc and anti-Th/To antibodies, 101 patients with SSc without anti-Th/To antibodies, and 114 healthy controls. DRB1*1502 and *0802 were more often found in anti-Th/To positive patients with SSc compared with healthy controls (50% v 24%, p=0.01; and 29% v 7%, p=0.03, respectively), but these frequencies in patients with SSc who were anti-Th/To positive or negative were similar (50% v 42% and 29% v 15%, respectively). Either DRB1*1502 or *0802 was detected in 79% of anti-Th/To positive patients with SSc compared with 29% in healthy controls (p=0.0009) and 51% in anti-Th/To negative patients with SSc (p=0.09).
HLA class II alleles were further compared between anti-Th/To positive patients with and without SSc. DRB1*1502 tended to be more often detected in patients with SSc than in patients without SSc (50% v 14%), but this difference did not reach statistical significance. Four of seven patients with SSc without DRB1*1502 had DRB1*0802. As a result, DRB1*1502 or *0802 was found significantly more often in patients with SSc than those without SSc (79% v 14%, p=0.02). By contrast, the DRB1*0405-DQB1*0401 haplotype was found less often in patients with SSc than those without (7% v 71%; p=0.01).
DISCUSSION
Anti-Th/To antibody was detected in 4.6% of patients with SSc, but also in patients with RA, SLE, PM, and primary SS, and even in a patient with ITP, a typical organ specific autoimmune disease. This finding clearly indicates that serum anti-Th/To antibody can be detected in patients with autoimmune disease without SSc or an SSc related condition, although the possibility that patients without SSc but with anti-Th/To antibodies may develop SSc later in the course of the disease cannot be excluded. In this regard, the originally reported Th serum was obtained from a patient with SLE.4 The percentage of patients with anti-Th/To antibodies was significantly greater for the patients with SSc than for all the patients without SSc combined, but this difference might be partly explained by the low frequency of patients who received immunosuppressive treatment in the SSc groups compared with SLE, PM/DM, or ITP.
Autoantibodies related to SSc are known to be mutually exclusive,14 but six of 14 anti-Th/To positive patients with SSc had concomitant SSc related antibodies, including antitopo I, anti-U1RNP, and ACA. However, anti-Th/To and ACA— autoantibodies associated with limited cutaneous SSc2,14—seem to be mutually exclusive, because coexistence of these two antibodies was found in only one of 303 patients with SSc, including 51 with ACA.
In this study we failed to detect clinical features associated with RNase P subunit reactivities in patients with SSc. This is probably due to a few patients with SSc and anti-Th/To antibody alone. However, antibody reactivity to hPop1 was detected exclusively in patients with SSc or those with Raynaud's phenomenon, suggesting that the presence of anti-hPop1 reactivity is an important clue to the later development of SSc in anti-Th/To positive patients without current SSc. A patient with RA and anti-hPop1 reactivity (patient 106) did not develop SSc over a period of 38 months, but the observation period may not be sufficient. Our preliminary study involving 18 patients with scleroderma spectrum disorder who did not satisfy the SSc criteria showed that all three anti-Th/To positive patients had anti-hPop1 reactivity. Further prospective studies using a larger series of patients with anti-hPop1 reactivity but without SSc is necessary to test this hypothesis.
There was a weak association between anti-Th/To antibody and DRB1*1502/*0802, but this association was not detected when the frequencies were compared between patients with SSc with and without anti-Th/To antibodies. This finding could be explained by the fact that DRB1*1502 and *0802 are associated with antitopo I and anti-U1RNP antibodies, respectively, in Japanese patients with SSc.15 Although Falkner et al reported that anti-Th/To antibody was associated with DRB1*11 in a North American white population,16 DRB1*11 was detected in none of the Japanese anti-Th/To positive patients. This is consistent with the well recognised ethnic difference in the HLA class II associations with autoantibodies related to SSc.14 Interestingly, the same pattern of the HLA class II association was reported in antitopo I antibody response—that is, the association with DRB1*11 in white people and with DRB1*1502 in Japanese people.17
Our comparison of anti-Th/To antibody responses in patients with and without SSc indicated that there is an association between the presence of antibodies that react with subunits of a complex autoantigen and disease expression. A similar finding was reported for the anti-U3 RNP antibody, another autoantibody related to SSc—that is, serum samples from patients with SSc recognised a form of the U3 RNP complex that contains the 34 kDa fibrillarin protein, whereas samples from patients with PM/DM recognised a form of the complex containing 22 to 25 kDa doublet proteins.18 Moreover, in the present study, the immunogenetic background of the anti-Th/To positive patients with or without SSc apparently differed; DRB1*1502/*0802 was found in the patients with SSc and the DRB1*0405-DQB1*0401 haplotype in the patients without SSc. This result may reflect the association of DRB1*1502/*0802 with anti-hPop1 reactivity, because serum samples from all anti-Th/To positive patients possessing DRB1*1502/*0802 reacted with hPop1 (table 1). Recently, we showed that the HLA-DR alleles that are associated with the presence of serum antitopo I antibodies are directly involved in the activation of topo I reactive CD4+ T cells.19 This implies that the HLA-DR alleles that are associated with particular autoantibody reactivities play a key part in the presentation of the antigenic peptides to autoantigen reactive CD4+ T cells. Therefore, the antigenic determinants that trigger and maintain anti-Th/To autoantibody responses may be different in patients with and those without SSc.
Acknowledgments
We are grateful to Ms Mutsuko Ishida for assisting in the RNA immunoprecipitation assay. This work was supported by grants from the Japanese Ministry of Health and Welfare; and from the Japanese Ministry of Education, Science, Sports, and Culture.